Journal of Shanghai Jiao Tong University (Medical Science) ›› 2022, Vol. 42 ›› Issue (7): 885-892.doi: 10.3969/j.issn.1674-8115.2022.07.006
• Clinical research • Previous Articles Next Articles
LAI Xiuxiu1( ), ZHU Qingyan1, TAN Jiaqi2, YANG Ling1, ZHU Yan1, ZHOU Gongmin1()
), ZHU Qingyan1, TAN Jiaqi2, YANG Ling1, ZHU Yan1, ZHOU Gongmin1()
Received:2022-03-09
Accepted:2022-06-10
Online:2022-07-28
Published:2022-07-25
Contact:
ZHOU Gongmin
E-mail:lxx1989lxx@163.com;whazqp@163.com
Supported by:CLC Number:
LAI Xiuxiu, ZHU Qingyan, TAN Jiaqi, YANG Ling, ZHU Yan, ZHOU Gongmin. Clinical study of low dose febuxostat on improving renal function in elderly patients with asymptomatic hyperuricemia[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(7): 885-892.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2022.07.006
| Item | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) | F/χ2 value | P value |
|---|---|---|---|---|---|
| Age/year | 88.66±2.88 | 89.28±3.47 | 89.68±3.35 | 0.824 | 0.442 |
| Male/n (%) | 18 (56.3) | 13 (40.6) | 15 (44.1) | 1.735 | 0.420 |
| SBP/mmHg | 126.34±11.23 | 127.13±8.95 | 126.38±13.92 | 0.046 | 0.955 |
| DBP/mmHg | 65.16±9.04 | 65.91±5.53 | 65.85±9.46 | 0.083 | 0.920 |
| BMI/(kg·m-2) | 24.97±4.08 | 25.20±5.50 | 24.58±3.32 | 0.171 | 0.843 |
| HbA1c/% | 6.34±0.75 | 6.23±0.53 | 6.30±0.66 | 0.204 | 0.816 |
| HB/(g·L-1) | 115.56±16.42 | 121.66±16.89 | 119.94±16.07 | 1.170 | 0.315 |
| Albumin/(g·L-1) | 39.50±3.50 | 39.68±3.64 | 39.65±3.38 | 0.025 | 0.976 |
| TAG/(mmol·L-1) | 1.23±0.53 | 1.37±0.65 | 1.36±0.73 | 0.486 | 0.616 |
| TC/(mmol·L-1) | 3.94±0.95 | 3.72±0.85 | 4.09±0.85 | 1.457 | 0.238 |
| HDL-C/(mmol·L-1) | 1.24±0.24 | 1.22±0.31 | 1.22±0.28 | 0.063 | 0.939 |
| LDL-C/(mmol·L-1) | 2.12±0.95 | 1.89±0.62 | 2.25±0.68 | 1.859 | 0.161 |
| SUA/(μmol·L-1) | 494.16±57.12 | 487.34±70.03 | 492.00±61.98 | 0.097 | 0.907 |
| Scr/(μmol·L-1) | 119.71±24.01 | 115.80±23.52 | 117.33±22.81 | 0.227 | 0.798 |
| Cys-C/(mg·L-1) | 1.71±0.36 | 1.68±0.35 | 1.71±0.37 | 0.109 | 0.897 |
| Ccr/(mL·min-1) | 33.05±8.69 | 31.75±7.55 | 30.18±7.08 | 0.228 | 0.796 |
| eGFR1/[mL·min-1·(1.73 m2)-1] | 48.52±10.47 | 47.28±9.27 | 47.12±7.62 | 0.227 | 0.797 |
| eGFR2/[mL·min-1·(1.73 m2)-1] | 42.91±9.79 | 41.89±8.63 | 41.54±6.91 | 0.230 | 0.795 |
| UACR | 0.06 (0.05, 0.14) | 0.06 (0.04, 0.09) | 0.09 (0.06, 0.13) | 3.547 | 0.170 |
| Hcy/(μmol·L-1) | 17.03±5.23 | 17.51±5.24 | 16.83±5.28 | 0.141 | 0.868 |
| Comorbidity/n (%) | |||||
| Diabetes mellitus | 13 (40.6) | 7 (21.9) | 7 (20.6) | 4.083 | 0.147 |
| Hypertension | 26 (81.3) | 26 (81.3) | 28 (82.4) | 0.018 | 0.991 |
| Coronary atherosclerotic heart disease | 20 (62.5) | 23 (71.9) | 17 (50.0) | 3.355 | 0.187 |
| Drug/n (%) | |||||
| ACEI/ARB | 17 (53.1) | 12 (37.5) | 12 (35.3) | 2.521 | 0.283 |
| Calcium antagonists | 9 (28.1) | 10 (31.3) | 16 (47.1) | 2.986 | 0.225 |
| Diuretics | 11 (34.4) | 13 (40.6) | 10 (29.4) | 0.917 | 0.632 |
| Sodium bicarbonate | 2 (6.3) | ‒ | ‒ | ‒ | ‒ |
| SGLT2i | ‒ | ‒ | ‒ | ‒ | ‒ |
| Calcium dobesilate | ‒ | 1 (3.1) | ‒ | ‒ | ‒ |
Tab 1 Clinical characteristics of patients at baseline in the three groups
| Item | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) | F/χ2 value | P value |
|---|---|---|---|---|---|
| Age/year | 88.66±2.88 | 89.28±3.47 | 89.68±3.35 | 0.824 | 0.442 |
| Male/n (%) | 18 (56.3) | 13 (40.6) | 15 (44.1) | 1.735 | 0.420 |
| SBP/mmHg | 126.34±11.23 | 127.13±8.95 | 126.38±13.92 | 0.046 | 0.955 |
| DBP/mmHg | 65.16±9.04 | 65.91±5.53 | 65.85±9.46 | 0.083 | 0.920 |
| BMI/(kg·m-2) | 24.97±4.08 | 25.20±5.50 | 24.58±3.32 | 0.171 | 0.843 |
| HbA1c/% | 6.34±0.75 | 6.23±0.53 | 6.30±0.66 | 0.204 | 0.816 |
| HB/(g·L-1) | 115.56±16.42 | 121.66±16.89 | 119.94±16.07 | 1.170 | 0.315 |
| Albumin/(g·L-1) | 39.50±3.50 | 39.68±3.64 | 39.65±3.38 | 0.025 | 0.976 |
| TAG/(mmol·L-1) | 1.23±0.53 | 1.37±0.65 | 1.36±0.73 | 0.486 | 0.616 |
| TC/(mmol·L-1) | 3.94±0.95 | 3.72±0.85 | 4.09±0.85 | 1.457 | 0.238 |
| HDL-C/(mmol·L-1) | 1.24±0.24 | 1.22±0.31 | 1.22±0.28 | 0.063 | 0.939 |
| LDL-C/(mmol·L-1) | 2.12±0.95 | 1.89±0.62 | 2.25±0.68 | 1.859 | 0.161 |
| SUA/(μmol·L-1) | 494.16±57.12 | 487.34±70.03 | 492.00±61.98 | 0.097 | 0.907 |
| Scr/(μmol·L-1) | 119.71±24.01 | 115.80±23.52 | 117.33±22.81 | 0.227 | 0.798 |
| Cys-C/(mg·L-1) | 1.71±0.36 | 1.68±0.35 | 1.71±0.37 | 0.109 | 0.897 |
| Ccr/(mL·min-1) | 33.05±8.69 | 31.75±7.55 | 30.18±7.08 | 0.228 | 0.796 |
| eGFR1/[mL·min-1·(1.73 m2)-1] | 48.52±10.47 | 47.28±9.27 | 47.12±7.62 | 0.227 | 0.797 |
| eGFR2/[mL·min-1·(1.73 m2)-1] | 42.91±9.79 | 41.89±8.63 | 41.54±6.91 | 0.230 | 0.795 |
| UACR | 0.06 (0.05, 0.14) | 0.06 (0.04, 0.09) | 0.09 (0.06, 0.13) | 3.547 | 0.170 |
| Hcy/(μmol·L-1) | 17.03±5.23 | 17.51±5.24 | 16.83±5.28 | 0.141 | 0.868 |
| Comorbidity/n (%) | |||||
| Diabetes mellitus | 13 (40.6) | 7 (21.9) | 7 (20.6) | 4.083 | 0.147 |
| Hypertension | 26 (81.3) | 26 (81.3) | 28 (82.4) | 0.018 | 0.991 |
| Coronary atherosclerotic heart disease | 20 (62.5) | 23 (71.9) | 17 (50.0) | 3.355 | 0.187 |
| Drug/n (%) | |||||
| ACEI/ARB | 17 (53.1) | 12 (37.5) | 12 (35.3) | 2.521 | 0.283 |
| Calcium antagonists | 9 (28.1) | 10 (31.3) | 16 (47.1) | 2.986 | 0.225 |
| Diuretics | 11 (34.4) | 13 (40.6) | 10 (29.4) | 0.917 | 0.632 |
| Sodium bicarbonate | 2 (6.3) | ‒ | ‒ | ‒ | ‒ |
| SGLT2i | ‒ | ‒ | ‒ | ‒ | ‒ |
| Calcium dobesilate | ‒ | 1 (3.1) | ‒ | ‒ | ‒ |
| Group | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) | P value① | P value② |
|---|---|---|---|---|---|
| SUA/(μmol·L-1) | |||||
| Baseline | 494.16±57.12 | 487.34±70.03 | 492.00±61.98 | 0.884 | 0.775 |
| 1 month after treatment | 233.00±89.20③ | 267.87±52.98③ | 448.79±46.74 | 0.000 | 0.000 |
| 3 months after treatment | 245.28±86.41③ | 269.78±58.87③ | 439.15±64.21③ | 0.000 | 0.000 |
| Scr/(μmol·L-1) | |||||
| Baseline | 119.71±24.01 | 115.80±23.52 | 117.33±22.81 | 0.681 | 0.789 |
| 1 month after treatment | 120.00±25.76 | 109.85±18.80④ | 117.95±25.20 | 0.745 | 0.146 |
| 3 months after treatment | 117.41±32.71 | 109.13±20.11⑤ | 120.42±24.30 | 0.671 | 0.045 |
| Ccr/(mL·min-1) | |||||
| Baseline | 33.05±8.69 | 31.75±7.55 | 30.18±7.08 | 0.120 | 0.329 |
| 1 month after treatment | 33.17±9.47 | 33.64±8.95⑥ | 29.96±7.27 | 0.126 | 0.070 |
| 3 months after treatment | 34.46±10.44 | 33.97±9.01⑥ | 29.21±7.07 | 0.019 | 0.019 |
| eGFR1/[mL·min-1·(1.73 m2)-1] | |||||
| Baseline | 48.52±10.47 | 47.28±9.27 | 47.12±7.62 | 0.536 | 0.941 |
| 1 month after treatment | 48.67±11.35 | 50.27±11.31⑦ | 47.12±8.27 | 0.528 | 0.200 |
| 3 months after treatment | 51.20±13.49④ | 50.65±11.00⑦ | 45.28±6.97 | 0.027 | 0.020 |
| eGFR2/[mL·min-1·(1.73 m2)-1] | |||||
| Baseline | 42.91±9.79 | 41.89±8.63 | 41.54±6.91 | 0.511 | 0.855 |
| 1 month after treatment | 43.04±10.57 | 44.62±10.35⑧ | 41.55±7.56 | 0.511 | 0.170 |
| 3 months after treatment | 45.54±12.65⑨ | 44.98±10.15⑩ | 40.07±6.44 | 0.029 | 0.021 |
Tab 2 Comparison of the changes in SUA and renal function among the three groups
| Group | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) | P value① | P value② |
|---|---|---|---|---|---|
| SUA/(μmol·L-1) | |||||
| Baseline | 494.16±57.12 | 487.34±70.03 | 492.00±61.98 | 0.884 | 0.775 |
| 1 month after treatment | 233.00±89.20③ | 267.87±52.98③ | 448.79±46.74 | 0.000 | 0.000 |
| 3 months after treatment | 245.28±86.41③ | 269.78±58.87③ | 439.15±64.21③ | 0.000 | 0.000 |
| Scr/(μmol·L-1) | |||||
| Baseline | 119.71±24.01 | 115.80±23.52 | 117.33±22.81 | 0.681 | 0.789 |
| 1 month after treatment | 120.00±25.76 | 109.85±18.80④ | 117.95±25.20 | 0.745 | 0.146 |
| 3 months after treatment | 117.41±32.71 | 109.13±20.11⑤ | 120.42±24.30 | 0.671 | 0.045 |
| Ccr/(mL·min-1) | |||||
| Baseline | 33.05±8.69 | 31.75±7.55 | 30.18±7.08 | 0.120 | 0.329 |
| 1 month after treatment | 33.17±9.47 | 33.64±8.95⑥ | 29.96±7.27 | 0.126 | 0.070 |
| 3 months after treatment | 34.46±10.44 | 33.97±9.01⑥ | 29.21±7.07 | 0.019 | 0.019 |
| eGFR1/[mL·min-1·(1.73 m2)-1] | |||||
| Baseline | 48.52±10.47 | 47.28±9.27 | 47.12±7.62 | 0.536 | 0.941 |
| 1 month after treatment | 48.67±11.35 | 50.27±11.31⑦ | 47.12±8.27 | 0.528 | 0.200 |
| 3 months after treatment | 51.20±13.49④ | 50.65±11.00⑦ | 45.28±6.97 | 0.027 | 0.020 |
| eGFR2/[mL·min-1·(1.73 m2)-1] | |||||
| Baseline | 42.91±9.79 | 41.89±8.63 | 41.54±6.91 | 0.511 | 0.855 |
| 1 month after treatment | 43.04±10.57 | 44.62±10.35⑧ | 41.55±7.56 | 0.511 | 0.170 |
| 3 months after treatment | 45.54±12.65⑨ | 44.98±10.15⑩ | 40.07±6.44 | 0.029 | 0.021 |
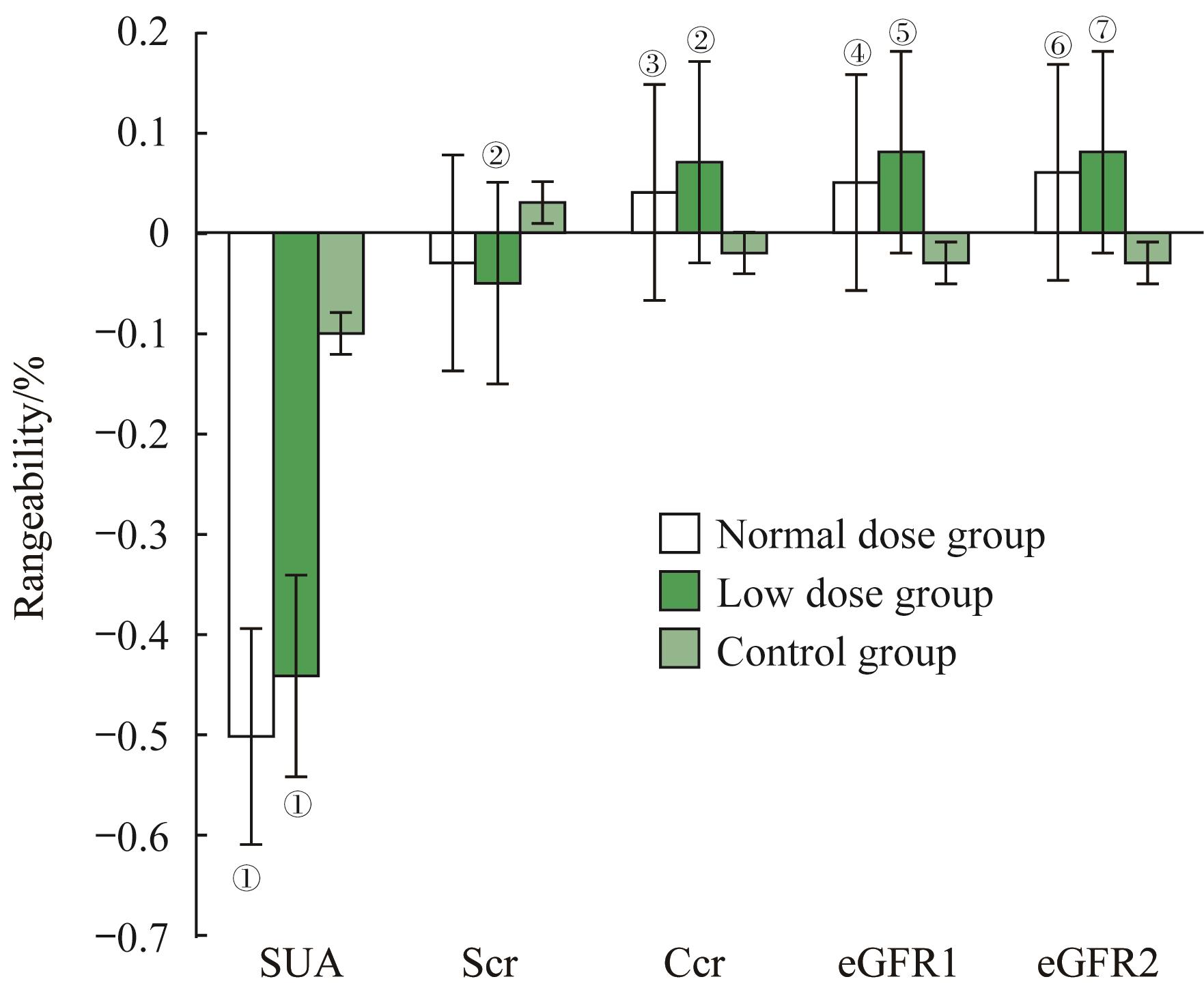
Fig 1 Comparison of changes in SUA, Scr, Ccr, eGFR among the three groups
| Adverse event | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) |
|---|---|---|---|
| Gout/n (%) | 0 (0) | 0 (0) | 0 (0) |
| Rash/n (%) | 1 (3.1) | 0 (0) | 0 (0) |
| Cardiovascular and cerebrovascular event/n (%) | 0 (0) | 0 (0) | 0 (0) |
| Gastrointestinal event/n (%) | 1 (3.1) | 1 (3.1) | 0 (0) |
| Respiratory event/n (%) | 6 (18.8) | 7 (21.9) | 5 (14.7) |
| Hepatic dysfunction/n (%) | 3 (9.4) | 1 (3.1) | 2 (5.9) |
| Pollakiuria/n (%) | 0 (0) | 1 (3.1) | 0 (0) |
| Allergy/n (%) | 0 (0) | 0 (0) | 0 (0) |
Tab 3 Adverse events in the three groups
| Adverse event | Normal dose group (n=32) | Low dose group (n=32) | Control group (n=34) |
|---|---|---|---|
| Gout/n (%) | 0 (0) | 0 (0) | 0 (0) |
| Rash/n (%) | 1 (3.1) | 0 (0) | 0 (0) |
| Cardiovascular and cerebrovascular event/n (%) | 0 (0) | 0 (0) | 0 (0) |
| Gastrointestinal event/n (%) | 1 (3.1) | 1 (3.1) | 0 (0) |
| Respiratory event/n (%) | 6 (18.8) | 7 (21.9) | 5 (14.7) |
| Hepatic dysfunction/n (%) | 3 (9.4) | 1 (3.1) | 2 (5.9) |
| Pollakiuria/n (%) | 0 (0) | 1 (3.1) | 0 (0) |
| Allergy/n (%) | 0 (0) | 0 (0) | 0 (0) |
| 1 | 赵芳雅, 陆俊茜, 张磊, 等. 上海地区糖尿病人群高尿酸血症的易患因素及肾功能预后分析[J]. 上海交通大学学报(医学版), 2019, 39(7): 783-788. |
| ZHAO F Y, LU J Q, ZHANG L, et al. Analysis of risk factors of hyperuricemia and its outcomes of renal function in diabetes mellitus in Shanghai[J]. J Shanghai Jiao Tong Univ (Med Sci), 2019, 39(7): 783-788. | |
| 2 | LI L, YANG C, ZHAO Y L, et al. Is hyperuricemia an independent risk factor for new-onset chronic kidney disease? A systematic review and meta-analysis based on observational cohort studies[J]. BMC Nephrol, 2014, 15: 122. |
| 3 | 赖秀秀, 来芹美, 周公民, 等. 高龄女性血尿酸水平与肾功能的关联性[J]. 温州医科大学学报, 2020, 50(5): 401-405. |
| LAI X X, LAI Q M, ZHOU G M, et al. Association between serum uric level and renal function in elderly women[J]. J Wenzhou Med Univ, 2020, 50(5): 401-405. | |
| 4 | HU A M, BROWN J N. Comparative effect of allopurinol and febuxostat on long-term renal outcomes in patients with hyperuricemia and chronic kidney disease: a systematic review[J]. Clin Rheumatol, 2020, 39(11): 3287-3294. |
| 5 | BECKER M A, SCHUMACHER H R, ESPINOZA L R, et al. The urate-lowering efficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: the CONFIRMS trial[J]. Arthritis Res Ther, 2010, 12(2): R63. |
| 6 | HOSOYA T, OHNO I. A repeated oral administration study of febuxostat (TMX-67), a non-purine-selective inhibitor of xanthine oxidase, in patients with impaired renal function in Japan: pharmacokinetic and pharmacodynamic study[J]. J Clin Rheumatol, 2011, 17(4 Suppl 2): S27-S34. |
| 7 | SEZAI A, SOMA M, NAKATA K I, et al. Comparison of febuxostat and allopurinol for hyperuricemia in cardiac surgery patients with chronic kidney disease (NU-FLASH trial for CKD)[J]. J Cardiol, 2015, 66(4): 298-303. |
| 8 | BEDDHU S, FILIPOWICZ R, WANG B, et al. A randomized controlled trial of the effects of febuxostat therapy on adipokines and markers of kidney fibrosis in asymptomatic hyperuricemic patients with diabetic nephropathy[J]. Can J Kidney Health Dis, 2016, 3: 2054358116675343. |
| 9 | 孙蔚楠, 朱清, 阎磊, 等. 非布司他治疗3~5期伴高尿酸血症老年慢性肾脏病的疗效与安全性[J]. 中国老年学杂志, 2019, 39(4): 862-865. |
| SUN W N, ZHU Q, YAN L, et al. Efficacy and safety of febuxostat in the treatment of hyperuricemia with chronic kidney disease stage 3‒5[J]. Chin J Gerontol, 2019, 39(4): 862-865. | |
| 10 | MATSUO H, ISHIKAWA E, MACHIDA H, et al. Efficacy of xanthine oxidase inhibitor for chronic kidney disease patients with hyperuricemia[J]. Clin Exp Nephrol, 2020, 24(4): 307-313. |
| 11 | 邓卫, 谢辉, 张海红, 等. 无症状高尿酸血症患者综合干预的疗效观察[J]. 实用医学杂志, 2017, 33(3): 443-446 |
| DENG W, XIE H, ZHANG H H, et al. Clinical effect of comprehensive intervention on 182 cases of asymptomatic hyperuricemia[J]. J Pract Med, 2017, 33(3): 443-446. | |
| 12 | Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 clinical practice guideline for the management of glomerular diseases[J]. Kidney Int, 2021, 100(4S): S1-S276. |
| 13 | FITZGERALD J D, DALBETH N, MIKULS T, et al. 2020 American college of rheumatology guideline for the management of gout[J]. Arthritis Care Res (Hoboken), 2020, 72(6): 744-760. |
| 14 | COCKCROFT D W, GAULT M H. Prediction of creatinine clearance from serum creatinine[J]. Nephron, 1976, 16(1): 31-41. |
| 15 | 张博旦, 李寒, 孙倩美. 不同肾小球滤过率评估公式在老年人中的适用性分析[J]. 中华老年多器官疾病杂志, 2018, 17(4): 313-317. |
| ZHANG B D, LI H, SUN Q M. Applicability analyses for glomerular filtration rate evaluation formula in the elderly[J]. Chin J Mult Organ Dis Elderly, 2018, 17(4): 313-317. | |
| 16 | MEEUSEN J W, KASOZI R N, LARSON T S, et al. Clinical impact of the refit CKD-EPI 2021 creatinine-based eGFR equation[J]. Clin Chem, 2022, 68(4): 534-539. |
| 17 | 高尿酸血症相关疾病诊疗多学科共识专家组. 中国高尿酸血症相关疾病诊疗多学科专家共识[J]. 中华内科杂志, 2017, 56(3): 235-248. |
| Multi-Disciplinary Expert Task Force on Hyperuricemia and Its Related Diseases. Chinese multi-disciplinary consensus on the diagnosis and treatment of hyperuricemia and its related diseases[J].Chin J Intern Med, 2017, 56(3): 235-248. | |
| 18 | KAMEI K, KONTA T, HIRAYAMA A, et al. A slight increase within the normal range of serum uric acid and the decline in renal function: associations in a community-based population[J]. Nephrol Dial Transplant, 2014, 29(12): 2286-2292. |
| 19 | 王贵红, 夏江莉, 周胜利, 等. 逐步增加口服非布司他剂量降尿酸治疗减少痛风性关节炎发作[J]. 中华风湿病学杂志, 2020, 24(6): 388-391. |
| WANG G H, XIA J L, ZHOU S L, et al. Reduced gout flares with stepwise dose increase of febuxostat during the initial introduction of urate-lowering therapy[J]. Chin J Rheumatol, 2020, 24(6): 388-391. | |
| 20 | YAMANAKA H, TAMAKI S, IDE Y, et al. Stepwise dose increase of febuxostat is comparable with colchicine prophylaxis for the prevention of gout flares during the initial phase of urate-lowering therapy: results from FORTUNE-1, a prospective, multicentre randomised study[J]. Ann Rheum Dis, 2018, 77(2): 270-276. |
| 21 | TOJIMBARA T, NAKAJIMA I, YASHIMA J, et al. Efficacy and safety of febuxostat, a novel nonpurine selective inhibitor of xanthine oxidase for the treatment of hyperuricemia in kidney transplant recipients[J]. Transplant Proc, 2014, 46(2): 511-513. |
| 22 | LIANG N, SUN M S, SUN R X, et al. Baseline urate level and renal function predict outcomes of urate-lowering therapy using low doses of febuxostat and benzbromarone: a prospective, randomized controlled study in a Chinese primary gout cohort[J]. Arthritis Res Ther, 2019, 21(1): 200. |
| 23 | LEE J W, LEE K H. Comparison of renoprotective effects of febuxostat and allopurinol in hyperuricemic patients with chronic kidney disease[J]. Int Urol Nephrol, 2019, 51(3): 467-473. |
| 24 | TSUJI T, OHISHI K, TAKEDA A, et al. The impact of serum uric acid reduction on renal function and blood pressure in chronic kidney disease patients with hyperuricemia[J]. Clin Exp Nephrol, 2018, 22(6): 1300-1308. |
| 25 | KIMURA K, HOSOYA T, UCHIDA S, et al. Febuxostat therapy for patients with stage 3 CKD and asymptomatic hyperuricemia: a randomized trial[J]. Am J Kidney Dis, 2018, 72(6): 798-810. |
| 26 | ZHU W, PANG M, DONG L, et al. Anti-inflammatory and immunomodulatory effects of iridoid glycosides from Paederia scandens (LOUR.) MERRILL (Rubiaceae) on uric acid nephropathy rats[J]. Life Sci, 2012, 91(11-12): 369-376. |
| 27 | SÁNCHEZ-LOZADA L G, LANASPA M A, CRISTÓBAL-GARCÍA M, et al. Uric acid-induced endothelial dysfunction is associated with mitochondrial alterations and decreased intracellular ATP concentrations[J]. Nephron Exp Nephrol, 2012, 121(3/4): e71-e78. |
| 28 | ZHOU Y, FANG L, JIANG L, et al. Uric acid induces renal inflammation via activating tubular NF-κB signaling pathway[J]. PLoS One, 2012, 7(6): e39738. |
| 29 | CORRY D B, ESLAMI P, YAMAMOTO K, et al. Uric acid stimulates vascular smooth muscle cell proliferation and oxidative stress via the vascular renin-angiotensin system[J]. J Hypertens, 2008, 26(2): 269-275. |
| 30 | TANAKA K, NAKAYAMA M, KANNO M, et al. Renoprotective effects of febuxostat in hyperuricemic patients with chronic kidney disease: a parallel-group, randomized, controlled trial[J]. Clin Exp Nephrol, 2015, 19(6): 1044-1053. |
| 31 | SÁNCHEZ-LOZADA L G, TAPIA E, SOTO V, et al. Effect of febuxostat on the progression of renal disease in 5/6 nephrectomy rats with and without hyperuricemia[J]. Nephron Physiol, 2008, 108(4): p69-p78. |
| 32 | OMORI H, KAWADA N, INOUE K, et al. Use of xanthine oxidase inhibitor febuxostat inhibits renal interstitial inflammation and fibrosis in unilateral ureteral obstructive nephropathy[J]. Clin Exp Nephrol, 2012, 16(4): 549-556. |
| [1] | Lu Bohan, Hu Cuirong, Wang Jinkun, Lu Jifang, Jin Haijiao, Wang Ling, Jiang Na, Mou Shan. Association between hyperuricemia and metabolic syndrome in adults [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(4): 486-495. |
| [2] | HAO Mingxiu, CHEN Hongwei, WANG Junlin, TANG Yinhan, WU Yunyun, JIN Yuhua, HU Yaomin. Investigation and epidemiological analysis of chronic diseases and comorbidities in hospitalized patients [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(4): 462-468. |
| [3] | XIE Lin, CHENG Ye, ZHENG Qimin, ZHANG Xi, FU Lili, CHEN Min, WANG Yi, MEI Changlin, XIE Jingyuan, GU Xiangchen. Preventive effect of icariin on transition from acute kidney injury to chronic kidney disease in mouse model [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(1): 8-19. |
| [4] | WANG Yakun, XU Jiarui, WU Qianqian, ZHANG Xiaohua, ZHU Yingchun, BAI Shoujun. Effect of combination of medical care and nursing on the quality of life and mental state of elderly patients with chronic kidney disease in Shanghai suburbs [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(7): 904-910. |
| [5] | WEI Shan, JI Ouyang, CHEN Zhihao, HUANG Zehui, LI Pu, FANG Junyan, LIU Yingli. Development and validation of a knowledge, attitude, belief and practice scale for safe medication in patients with chronic kidney disease [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(12): 1729-1738. |
| [6] | Hua-jie DAI, Li-ping XUAN, Jia-li XIANG, Hong LIN, Zhi-yun ZHAO, Tian-ge WANG, Mian LI, Yu XU, Jie-li LU, Wei-qing WANG, Yu-fang BI, Min XU. Correlation between healthy vascular aging and prevalent cardiovascular disease risk in middle-aged and elderly people in the community of Shanghai [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2021, 41(2): 223-227. |
| [7] | LUAN Wei, ZHU Zhu, ZHU Dong-ping, GE Wen-jing, ZHU Qun-mei, JIANG Yan-qing, LI Jin, JIANG An-li. Relationship of health promotion lifestyle with social support and self-efficacy of the elderly in urban-rural communities [J]. , 2020, 40(1): 107-. |
| [8] | XU Ji-chao, HU Hao-lu, DING Wei . Association between level of vitamin D in serum and peripheral neuropathy in elderly patients with type 2 diabetes [J]. , 2017, 37(5): 684-. |
| [9] | LIANG Wei, TIAN Shu-ya, REN Yan, SHEN Lin-hui . Serum CTRP1 level and its relationship with serum adiponectin level in elderly male metabolic syndrome patients [J]. , 2017, 37(2): 218-. |
| [10] | WANG Hong-yu, ZHANG Lin. Reliability and validity of short form Quality Life Scale (SF-12) for elderly persons in countryside [J]. , 2016, 36(7): 1070-. |
| [11] | SONG Tai-xia, MA Chao-qun, FU Guang-jian, et al. Effects of smoking on cognitive impairment of elderly people [J]. , 2014, 34(8): 1225-. |
| [12] | YANG Yang, ZHOU Pei-Jun, XU Da, et al. Reducing dosage of corticosteroid by mycophenolate acid therapeutic drug monitoring for renal allograft recipients [J]. , 2014, 34(10): 1534-. |
| [13] | YANG Bin, WU Yan, LI De-yan, et al. Application of CARE kV technique in chest CT scanning [J]. , 2013, 33(8): 1117-. |
| [14] | ZHOU Xiao-kai, YI Cheng-qing, MA Chun-hui, et al. Two cases report of hip arthroplasty for patients with femoral neck fracture aged more than 100 [J]. , 2012, 32(12): 1564-. |
| [15] | NIE Xiu-li, JIANG Ying, YAN Wei-li, et al. One case report of nodular goiter (Ⅲ) complicated with hyperthyroidism treated by 131iodine [J]. , 2010, 30(9): 1081-. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||