Journal of Shanghai Jiao Tong University (Medical Science) ›› 2023, Vol. 43 ›› Issue (3): 333-341.doi: 10.3969/j.issn.1674-8115.2023.03.009
• Evidence-based medicine • Previous Articles
ZHANG Yuanyuan1( ), WU Anqi2, WU Jie1, ZHU Yaqi1, LI Mengyao1, YAN Dexiu1, ZHANG Yaqing1(), HOU Lili3()
), WU Anqi2, WU Jie1, ZHU Yaqi1, LI Mengyao1, YAN Dexiu1, ZHANG Yaqing1(), HOU Lili3()
Received:2023-01-03
Accepted:2023-03-20
Online:2023-03-28
Published:2023-03-28
Contact:
ZHANG Yaqing,HOU Lili
E-mail:zhangyy@shsmu.edu.cn;zhangyqf@shsmu.edu.cn;pisces_liz@163.com
Supported by:CLC Number:
ZHANG Yuanyuan, WU Anqi, WU Jie, ZHU Yaqi, LI Mengyao, YAN Dexiu, ZHANG Yaqing, HOU Lili. Interventions to enhance return-to-work among young and middle-aged cancer survivors: a systematic review[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(3): 333-341.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2023.03.009
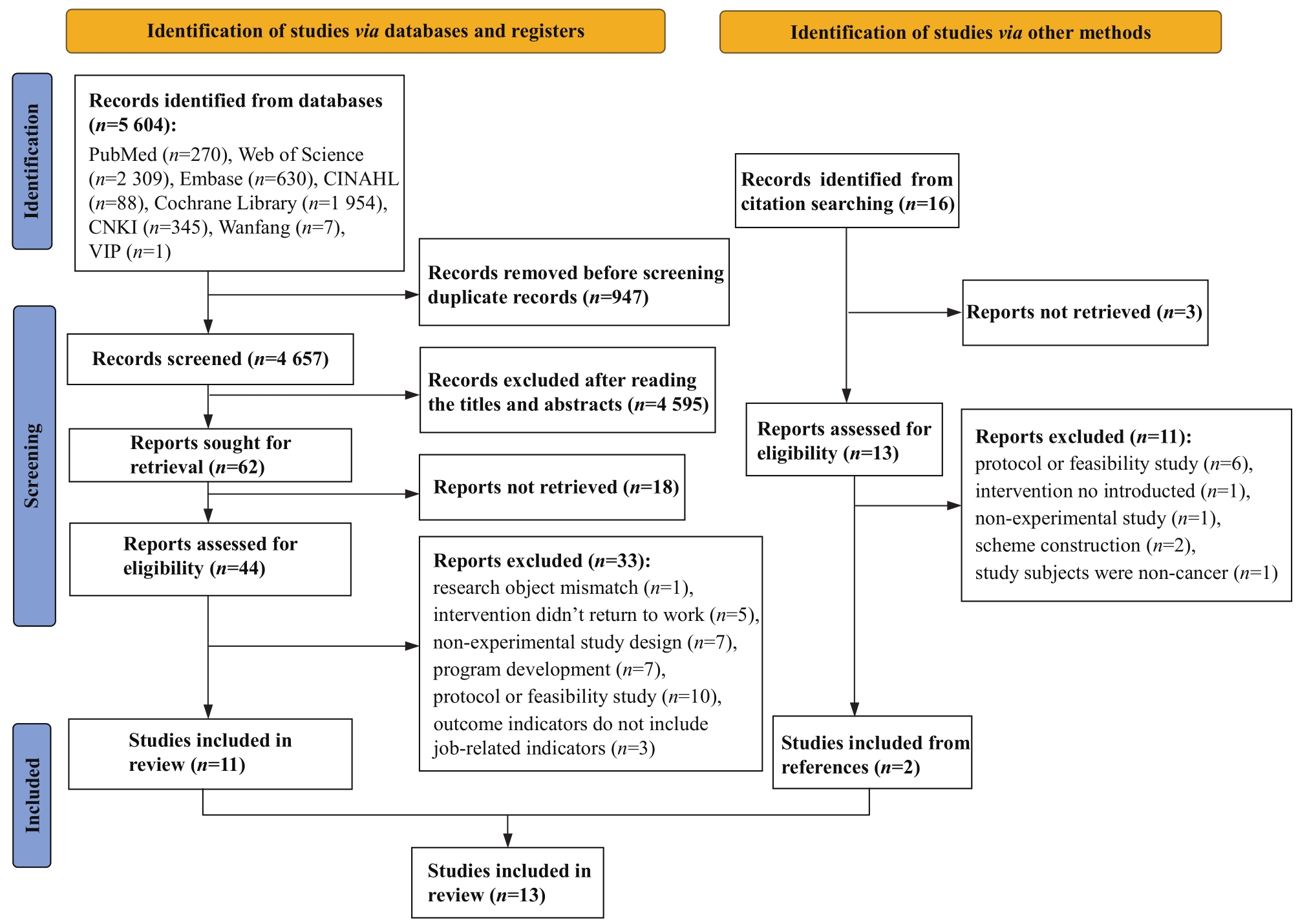
Fig 1 PRISMA flow diagram
| Study | Country | Design | Participants, characteristics in intervention group | Participants, characteristics in control group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (at allocation)/n | Age/year | Gender | Cancer type | Sample size (at allocation) /n | Age/year | Gender | Cancer type | |||
| BJÖRNEKLETT et al, 2013[ | Sweden | ① | 191 | 57.8 (30‒84) | Female: 100% | Breast: 100% | 191 | 58.7 (38‒83) | Female: 100% | Breast: 100% |
FAUSER et al, 2019[ | Germany | ② | 229 | 50.8±7.1 | Female: 71.2% | Breast: 31.4%, digestive tract: 14.4%, lymphatic/related tissue: 15.3%, female genitalia: 15.3% | 255 | 50.3±7.9 | Female: 63.1% | Breast: 28.2%, digestive tract: 18.4%, lymphatic/related tissue: 14.9%, female genitalia: 10.6% |
LEENSEN et al, 2017[ | Netherlands | ④ | 93 | 47.9±7.4 | Female: 90.3% | Breast: 83.9%, colorectal: 8.6%, non-Hodgkin′s lymphoma: 5.4%, other: 2.2% | ‒ | ‒ | ‒ | ‒ |
OLDERVOLL et al, 2013[ | Norway | ③ | 56 | 51 (37‒66) | NR | Breast: 91%, gynecological: 9% | 60 | 50 (32‒67) | NR | Breast: 55%, gynecological: 45% |
MOURGUES et al, 2014[ | France | ① | 85 | 51.9±8.5 | Female: 100% | Breast: 100% | 67 | 51.9±10.3 | Female: 100% | Breast: 100% |
RUSBRIDGE et al, 2013[ | UK | ④ | 34 | 46±11 | Male: 59% | Brain: 100% | ‒ | ‒ | ‒ | ‒ |
| STAPELFELDT et al, 2021[ | Denmark | ① | 83 | 48.2 (44‒56) | Female: 91.6% | Breast: 78.3%, colonrectal: 13.3% | 264 | 50.0 (43.7‒54.6) | Female: 92.8% | Breast: 85.2%, colonrectal: 10.2% |
TAMMINGA et al, 2013[ | Netherlands | ① | 65 | 47.5±8.2 | Female: 99% | Breast: 64%, cervix: 23% | 68 | 47.6±7.8 | Female: 100% | Breast: 60%, cervix: 22% |
TAMMINGA et al, 2019[ | Netherlands | ① | 49 | 47.1±8.2 | Female: 98% | Breast: 61%, cervix: 22% | 57 | 47.8±7.6 | Female: 100% | Breast: 61%, cervix: 23% |
THIJS et al, 2012[ | Netherlands | ③ | 72 | 49±8.3 | Female: 88.9% | Breast: 70.8%, lymphoma: 13.8%, colorectal: 6.9% | 38 | 49±9.2 | Female: 76.3% | Breast: 68.4%, lymphoma: 18.5%, colorectal: 13.2% |
THORSEN et al, 2016[ | Norway | ④ | 106 | 48.8±8.6 | Female: 100% | Breast: 60.4%, gynaecological: 31.1% | ‒ | ‒ | ‒ | ‒ |
ZAMAN et al, 2021[ | Netherlands | ① | 42 | 54±7.7 | Male: 64% | Colonrectal: 88.1% | 46 | 56±6.6 | Male: 67% | Colonrectal: 84.8% |
Tab 1 Basic characteristics of included studies
| Study | Country | Design | Participants, characteristics in intervention group | Participants, characteristics in control group | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Sample size (at allocation)/n | Age/year | Gender | Cancer type | Sample size (at allocation) /n | Age/year | Gender | Cancer type | |||
| BJÖRNEKLETT et al, 2013[ | Sweden | ① | 191 | 57.8 (30‒84) | Female: 100% | Breast: 100% | 191 | 58.7 (38‒83) | Female: 100% | Breast: 100% |
FAUSER et al, 2019[ | Germany | ② | 229 | 50.8±7.1 | Female: 71.2% | Breast: 31.4%, digestive tract: 14.4%, lymphatic/related tissue: 15.3%, female genitalia: 15.3% | 255 | 50.3±7.9 | Female: 63.1% | Breast: 28.2%, digestive tract: 18.4%, lymphatic/related tissue: 14.9%, female genitalia: 10.6% |
LEENSEN et al, 2017[ | Netherlands | ④ | 93 | 47.9±7.4 | Female: 90.3% | Breast: 83.9%, colorectal: 8.6%, non-Hodgkin′s lymphoma: 5.4%, other: 2.2% | ‒ | ‒ | ‒ | ‒ |
OLDERVOLL et al, 2013[ | Norway | ③ | 56 | 51 (37‒66) | NR | Breast: 91%, gynecological: 9% | 60 | 50 (32‒67) | NR | Breast: 55%, gynecological: 45% |
MOURGUES et al, 2014[ | France | ① | 85 | 51.9±8.5 | Female: 100% | Breast: 100% | 67 | 51.9±10.3 | Female: 100% | Breast: 100% |
RUSBRIDGE et al, 2013[ | UK | ④ | 34 | 46±11 | Male: 59% | Brain: 100% | ‒ | ‒ | ‒ | ‒ |
| STAPELFELDT et al, 2021[ | Denmark | ① | 83 | 48.2 (44‒56) | Female: 91.6% | Breast: 78.3%, colonrectal: 13.3% | 264 | 50.0 (43.7‒54.6) | Female: 92.8% | Breast: 85.2%, colonrectal: 10.2% |
TAMMINGA et al, 2013[ | Netherlands | ① | 65 | 47.5±8.2 | Female: 99% | Breast: 64%, cervix: 23% | 68 | 47.6±7.8 | Female: 100% | Breast: 60%, cervix: 22% |
TAMMINGA et al, 2019[ | Netherlands | ① | 49 | 47.1±8.2 | Female: 98% | Breast: 61%, cervix: 22% | 57 | 47.8±7.6 | Female: 100% | Breast: 61%, cervix: 23% |
THIJS et al, 2012[ | Netherlands | ③ | 72 | 49±8.3 | Female: 88.9% | Breast: 70.8%, lymphoma: 13.8%, colorectal: 6.9% | 38 | 49±9.2 | Female: 76.3% | Breast: 68.4%, lymphoma: 18.5%, colorectal: 13.2% |
THORSEN et al, 2016[ | Norway | ④ | 106 | 48.8±8.6 | Female: 100% | Breast: 60.4%, gynaecological: 31.1% | ‒ | ‒ | ‒ | ‒ |
ZAMAN et al, 2021[ | Netherlands | ① | 42 | 54±7.7 | Male: 64% | Colonrectal: 88.1% | 46 | 56±6.6 | Male: 67% | Colonrectal: 84.8% |
| Study | Intervention group | Control group | Outcome | ||||
|---|---|---|---|---|---|---|---|
| Content | Type | Who | How long | Where | |||
| BJÖRNEKLETT et al, 2013[ | Information-based support program: information about cancer illnesses, aetiology, risk factors, etc; physical exercise, relaxation training, qi-gong and nonverbal communication; social activities such as concerts, and visits to museums and restaurants | A | Oncologists (n=4), social workers (n=2), art therapists (n=2), masseuses (n=2), a person trained in qi-gong and mental visualization (n=1) | 7 d followed by a 4-day follow-up 2 months after the initial visit | Resort | Standard follow-up routine | b |
FAUSER et al, 2019[ | Work-related medical rehabilitation: work-related diagnostics (at least 60 min), and multiprofessional team meetings; work-related functional capacity training (at least 360 min), work-related psychosocial groups (at least 240 min), and intensified social counseling (at least 90 min) | A, B | Physician, psychologist, occupational therapist, physiotherapist, social worker | 25 d in average | Rehabilitation center | Traditional medical rehabilitation program | a, c |
LEENSEN et al, 2017[ | Multidisciplinary intervention: personal counselling on work-related issues (1‒3 sessions), and supervised physical exercise (2 times per week, 12 weeks) | B | Oncological occupational physician, sport physician, physiotherapist | 4 months in average | Hospital | Without control | a①, d①, e②, f①, g① |
OLDERVOLL et al, 2013[ | Inpatient rehabilitation program: physical exercise (twice a day, 100 h during 4 weeks), patient education (each day), group discussion (each day). The focus of patient education and group discussion session: cancer treatment and side effect, physical activity, nutrition, economy and work situation, factors of return-to-work, partnership and sexuality, and psychological reaction | A | Multiprofessional team | 4 weeks | Rehabilitation center | Outpatient rehabilitation program: delivered at an academic cancer hospital, lasted for seven weeks. The focus were the same | h |
MOURGUES et al, 2014[ | Thermal water treatment: physiotherapy (2 h/d, supervised by physiotherapist), thermal water treatment (30 min/d), and basic dietary follow-up (each day) | A | Physician, nutritionist, physiotherapist | 15 d | Resort | Standard follow-up routine | a③, d④ |
RUSBRIDGE et al, 2013[ | Occupational rehabilitation program: patients-based symptom management (fatigue management, psychological support, and cognitive rehabilitation), work place intervention involving employers | B | Occupational therapist and/or neuropsychologist | 11 h sessions over 5 months | Hospital | Without control | a⑤ |
| STAPELFELDT et al, 2021[ | Early, individualized vocational rehabilitation intervention: return-to-work readiness and need assessment by social worker, tailored return to work plan development by social worker, coordinating the return-to-work plan with the participant′s employer, assessing participants′ rehabilitation needs other than vocational | B | Social worker trained by psychologist | Continued until the participants returned to work or for 1 year | Hospital | Municipal sickness benefit management by Danish Sickness Benefit Act | a |
TAMMINGA et al, 2013[ TAMMINGA et al, 2019[ | Hospital-based work support intervention: delivering patient education and support at the hospital, as part of usual psycho-oncology care; improving communication between the treating physician and the occupational physician; drawing up a concrete and gradual return-to-work plan in collaboration with the cancer patient, the occupational physician, and the employer | B | Oncology nurse, medical social worker, occupational physician | A few weeks to 14 months | Hospital | Standard program by Dutch government | 1 year follow-up: a, b, d, g; 2 year follow-up: a, b, d, g |
THIJS et al, 2012[ | High-intensity physical training: strength and interval training, home-based activities | B | Physiotherapist | 18 weeks | Hospital | Standard medical care(without physical rehabilitation program) | a, b, i⑥ |
THORSEN et al, 2016[ | Rapid return-to-work program (a full day weekly): patient education (2 h), group discussion (1 h), and physical activity (60‒120 min). The first two sessions covered the topics related to cancer treatment, side effects, partnership and sexuality, economy and work situation, nutrition, physical exercise and coping strategies | B | Relevant health professionals, physiotherapist | 7 weeks | Outpatient | Without control | h (36% did not improve work status) |
ZAMAN et al, 2021[ | Early tailored work-related support intervention: individual meetings of psychosocial work-related support (30 min each); work related support: fatigue, pain and lack of support from family and friends (support Ⅰ); lack of support in work environment and neuropsychological problems (support Ⅱ); a combination of factors (support Ⅲ) | B | Support Ⅰ: oncological gastrointestinal nurse; support Ⅱ: oncological occupational physicians (OOP); support Ⅲ: multidisciplinary team (including at least a oncology nurse, a physician and a OOP) | Maximum of 9 months | Hospital | Standard psychological care provided by oncological nurse | a, b |
Tab 2 Characteristics of return-to-work interventions
| Study | Intervention group | Control group | Outcome | ||||
|---|---|---|---|---|---|---|---|
| Content | Type | Who | How long | Where | |||
| BJÖRNEKLETT et al, 2013[ | Information-based support program: information about cancer illnesses, aetiology, risk factors, etc; physical exercise, relaxation training, qi-gong and nonverbal communication; social activities such as concerts, and visits to museums and restaurants | A | Oncologists (n=4), social workers (n=2), art therapists (n=2), masseuses (n=2), a person trained in qi-gong and mental visualization (n=1) | 7 d followed by a 4-day follow-up 2 months after the initial visit | Resort | Standard follow-up routine | b |
FAUSER et al, 2019[ | Work-related medical rehabilitation: work-related diagnostics (at least 60 min), and multiprofessional team meetings; work-related functional capacity training (at least 360 min), work-related psychosocial groups (at least 240 min), and intensified social counseling (at least 90 min) | A, B | Physician, psychologist, occupational therapist, physiotherapist, social worker | 25 d in average | Rehabilitation center | Traditional medical rehabilitation program | a, c |
LEENSEN et al, 2017[ | Multidisciplinary intervention: personal counselling on work-related issues (1‒3 sessions), and supervised physical exercise (2 times per week, 12 weeks) | B | Oncological occupational physician, sport physician, physiotherapist | 4 months in average | Hospital | Without control | a①, d①, e②, f①, g① |
OLDERVOLL et al, 2013[ | Inpatient rehabilitation program: physical exercise (twice a day, 100 h during 4 weeks), patient education (each day), group discussion (each day). The focus of patient education and group discussion session: cancer treatment and side effect, physical activity, nutrition, economy and work situation, factors of return-to-work, partnership and sexuality, and psychological reaction | A | Multiprofessional team | 4 weeks | Rehabilitation center | Outpatient rehabilitation program: delivered at an academic cancer hospital, lasted for seven weeks. The focus were the same | h |
MOURGUES et al, 2014[ | Thermal water treatment: physiotherapy (2 h/d, supervised by physiotherapist), thermal water treatment (30 min/d), and basic dietary follow-up (each day) | A | Physician, nutritionist, physiotherapist | 15 d | Resort | Standard follow-up routine | a③, d④ |
RUSBRIDGE et al, 2013[ | Occupational rehabilitation program: patients-based symptom management (fatigue management, psychological support, and cognitive rehabilitation), work place intervention involving employers | B | Occupational therapist and/or neuropsychologist | 11 h sessions over 5 months | Hospital | Without control | a⑤ |
| STAPELFELDT et al, 2021[ | Early, individualized vocational rehabilitation intervention: return-to-work readiness and need assessment by social worker, tailored return to work plan development by social worker, coordinating the return-to-work plan with the participant′s employer, assessing participants′ rehabilitation needs other than vocational | B | Social worker trained by psychologist | Continued until the participants returned to work or for 1 year | Hospital | Municipal sickness benefit management by Danish Sickness Benefit Act | a |
TAMMINGA et al, 2013[ TAMMINGA et al, 2019[ | Hospital-based work support intervention: delivering patient education and support at the hospital, as part of usual psycho-oncology care; improving communication between the treating physician and the occupational physician; drawing up a concrete and gradual return-to-work plan in collaboration with the cancer patient, the occupational physician, and the employer | B | Oncology nurse, medical social worker, occupational physician | A few weeks to 14 months | Hospital | Standard program by Dutch government | 1 year follow-up: a, b, d, g; 2 year follow-up: a, b, d, g |
THIJS et al, 2012[ | High-intensity physical training: strength and interval training, home-based activities | B | Physiotherapist | 18 weeks | Hospital | Standard medical care(without physical rehabilitation program) | a, b, i⑥ |
THORSEN et al, 2016[ | Rapid return-to-work program (a full day weekly): patient education (2 h), group discussion (1 h), and physical activity (60‒120 min). The first two sessions covered the topics related to cancer treatment, side effects, partnership and sexuality, economy and work situation, nutrition, physical exercise and coping strategies | B | Relevant health professionals, physiotherapist | 7 weeks | Outpatient | Without control | h (36% did not improve work status) |
ZAMAN et al, 2021[ | Early tailored work-related support intervention: individual meetings of psychosocial work-related support (30 min each); work related support: fatigue, pain and lack of support from family and friends (support Ⅰ); lack of support in work environment and neuropsychological problems (support Ⅱ); a combination of factors (support Ⅲ) | B | Support Ⅰ: oncological gastrointestinal nurse; support Ⅱ: oncological occupational physicians (OOP); support Ⅲ: multidisciplinary team (including at least a oncology nurse, a physician and a OOP) | Maximum of 9 months | Hospital | Standard psychological care provided by oncological nurse | a, b |
| 1 | SHAPIRO C L. Cancer survivorship[J]. N Engl J Med, 2018, 379(25): 2438-2450. |
| 2 | FENG R M, ZONG Y N, CAO S M, et al. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics?[J]. Cancer Commun, 2019, 39(1): 22. |
| 3 | 郑莹. 上海市肿瘤预防控制工作70年回顾[J]. 中国卫生资源, 2019, 22(4): 269-273, 289. |
| ZHENG Y. Seventy years of cancer prevention and control in Shanghai[J]. Chinese Health Resources, 2019, 22(4): 269-273, 289. | |
| 4 | MILLER K D, FIDLER-BENAOUDIA M, KEEGAN T H, et al. Cancer statistics for adolescents and young adults, 2020[J]. CA Cancer J Clin, 2020, 70(6): 443-459. |
| 5 | SIEGEL R L, MILLER K D, JEMAL A. Cancer statistics, 2020[J]. CA A Cancer J Clin, 2020, 70(1): 7-30. |
| 6 | RINGASH J, BERNSTEIN L J, DEVINS G, et al. Head and neck cancer survivorship: learning the needs, meeting the needs[J]. Semin Radiat Oncol, 2018, 28(1): 64-74. |
| 7 | CHECK D K, HUTCHESON K A, POISSON L M, et al. Factors associated with employment discontinuation among older and working age survivors of oropharyngeal cancer[J]. Head Neck, 2019, 41(11): 3948-3959. |
| 8 | BJÖRNEKLETT H G, ROSENBLAD A, LINDEMALM C, et al. A randomized controlled trial of support group intervention after breast cancer treatment: results on sick leave, health care utilization and health economy[J]. Acta Oncol, 2013, 52(1): 38-47. |
| 9 | FAUSER D, WIENERT J, BEINERT T, et al. Work-related medical rehabilitation in patients with cancer-postrehabilitation results from a cluster-randomized multicenter trial[J]. Cancer, 2019, 125(15): 2666-2674. |
| 10 | FAUSER D, WIENERT J, ZOMORODBAKHSCH B, et al. Work-related medical rehabilitation in cancer: a cluster-randomized multicenter study[J]. Dtsch Arztebl Int, 2019, 116(35/36): 592-599. |
| 11 | LEENSEN M C J, GROENEVELD I F, VAN DER HEIDE I, et al. Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: a prospective study in the Netherlands[J]. BMJ Open, 2017, 7(6): e014746. |
| 12 | OLDERVOLL L M, THORSEN L, KAASA S, et al. Inpatient versus outpatient rehabilitation after breast and gynecological cancers: a comparative study[J]. Int J Phys Med Rehabil, 2013, 2(2): 1-7. |
| 13 | MOURGUES C, GERBAUD L, LEGER S, et al. Positive and cost-effectiveness effect of spa therapy on the resumption of occupational and non-occupational activities in women in breast cancer remission: a French multicentre randomised controlled trial[J]. Eur J Oncol Nurs, 2014, 18(5): 505-511. |
| 14 | RUSBRIDGE S L, WALMSLEY N C, GRIFFITHS S B, et al. Predicting outcomes of vocational rehabilitation in patients with brain tumours[J]. Psycho-oncology, 2013, 22(8): 1907-1911. |
| 15 | STAPELFELDT C M, MOMSEN A M H, JENSEN A B, et al. Municipal return to work management in cancer survivors: a controlled intervention study[J]. Acta Oncol, 2021, 60(3): 370-378. |
| 16 | TAMMINGA S J, VERBEEK J H A M, BOS M M E M, et al. Effectiveness of a hospital-based work support intervention for female cancer patients: a multi-centre randomised controlled trial[J]. PLoS One, 2013, 8(5): e63271. |
| 17 | TAMMINGA S J, VERBEEK J M, BOS M M, et al. Two-year follow-up of a multi-centre randomized controlled trial to study effectiveness of a hospital-based work support intervention for cancer patients[J]. J Occup Rehabil, 2019, 29(4): 701-710. |
| 18 | THIJS K M, DE BOER A G E M, VREUGDENHIL G, et al. Rehabilitation using high-intensity physical training and long-term return-to-work in cancer survivors[J]. J Occup Rehabil, 2012, 22(2): 220-229. |
| 19 | THORSEN L, DAHL A A, NYSTAD R, et al. Baseline characteristics in female cancer patients with unimproved work status after an outpatient rehabilitation program and health changes during the intervention[J]. Springerplus, 2016, 5(1): 1009. |
| 20 | ZAMAN A M, TYTGAT K J, KLINKENBIJL J G, et al. Effectiveness of a tailored work-related support intervention for patients diagnosed with gastrointestinal cancer: a multicenter randomized controlled trial[J]. J Occup Rehabil, 2021, 31(2): 323-338. |
| 21 | TAMMINGA S J, HOVING J L, FRINGS-DRESEN M H W, et al. Cancer@Work: a nurse-led, stepped-care, e-health intervention to enhance the return to work of patients with cancer: study protocol for a randomized controlled trial[J]. Trials, 2016, 17(1): 453. |
| 22 | YOUNG A E, ROESSLER R T, WASIAK R, et al. A developmental conceptualization of return to work[J]. J Occup Rehabil, 2005, 15(4): 557-568. |
| 23 | GUO Y J, TANG J, LI J M, et al. Exploration of interventions to enhance return-to-work for cancer patients: a scoping review[J]. Clin Rehabil, 2021, 35(12): 1674-1693. |
| 24 | FITCH M I, NICOLL I. Returning to work after cancer: survivors′, caregivers′, and employers′ perspectives[J]. Psycho-oncology, 2019, 28(4): 792-798. |
| 25 | 梁莉莉, 张艳, 史岩, 等. 时机理论在疾病护理中的应用研究进展[J]. 护理研究, 2016, 30(5): 524-525. |
| LIANG L L, ZHANG Y, SHI Y, et al. Research progress on application of timing theory in disease nursing[J]. Chinese Nursing Research, 2016, 30(5): 524-525. | |
| 26 | SEIFART U, SCHMIELAU J. Return to work of cancer survivors[J]. Oncol Res Treat, 2017, 40(12): 760-763. |
| 27 | CHEN S C, HUANG B S, HUNG T M, et al. Impact of physical and psychosocial dysfunction on return to work in survivors of oral cavity cancer[J]. Psycho-oncology, 2019, 28(9): 1910-1917. |
| 28 | RANGABASHYAM M, KOH S Q, SULTANA R, et al. Factors associated with returning to work in head and neck cancer survivors in Singapore: a preliminary exploratory mixed-methods approach study[J]. Head Neck, 2021, 43(5): 1451-1464. |
| 29 | KJÆR T, BØJE C R, OLSEN M H, et al. Affiliation to the work market after curative treatment of head-and-neck cancer: a population-based study from the DAHANCA database[J]. Acta Oncol, 2013, 52(2): 430-439. |
| 30 | BAXI S S, SALZ T, XIAO H, et al. Employment and return to work following chemoradiation in patient with HPV-related oropharyngeal cancer[J]. Cancers Head Neck, 2016, 1: 4. |
| 31 | AGARWAL J, KRISHNATRY R, CHATURVEDI P, et al. Survey of return to work of head and neck cancer survivors: a report from a tertiary cancer center in India[J]. Head Neck, 2017, 39(5): 893-899. |
| 32 | GREIDANUS M A, DE BOER A G E M, DE RIJK A E, et al. Perceived employer-related barriers and facilitators for work participation of cancer survivors: a systematic review of employers′ and survivors′ perspectives[J]. Psycho-oncology, 2018, 27(3): 725-733. |
| [1] | FANG Fang, TAI Rui, YU Qian, ZHANG Yaqing. Effect of prehabilitation on outcomes in patients undergoing elective gastrointestinal surgery: a systematic review [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(1): 70-78. |
| [2] | WU Sheng-jia, LI Xian-hua, KANG Lei, XIN Xiao, NI Xue-ping, SONG Ting. Study on social participation and influencing factors in young and middle-aged patients after coronary artery bypass grafting [J]. , 2020, 40(2): 247-. |
| [3] | JIN Jing, HU Yao-min, LIU Wei. Systematic evaluation of selenium in treatment of autoimmune thyroiditis [J]. , 2010, 30(11): 1356-. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||