| 1 |
AOYAMA T, MURAKAWA M, KATAYAMA Y, et al. Impact of postoperative complications on survival and recurrence in pancreatic cancer[J]. Anticancer Res, 2015, 35(4): 2401-2409.
|
| 2 |
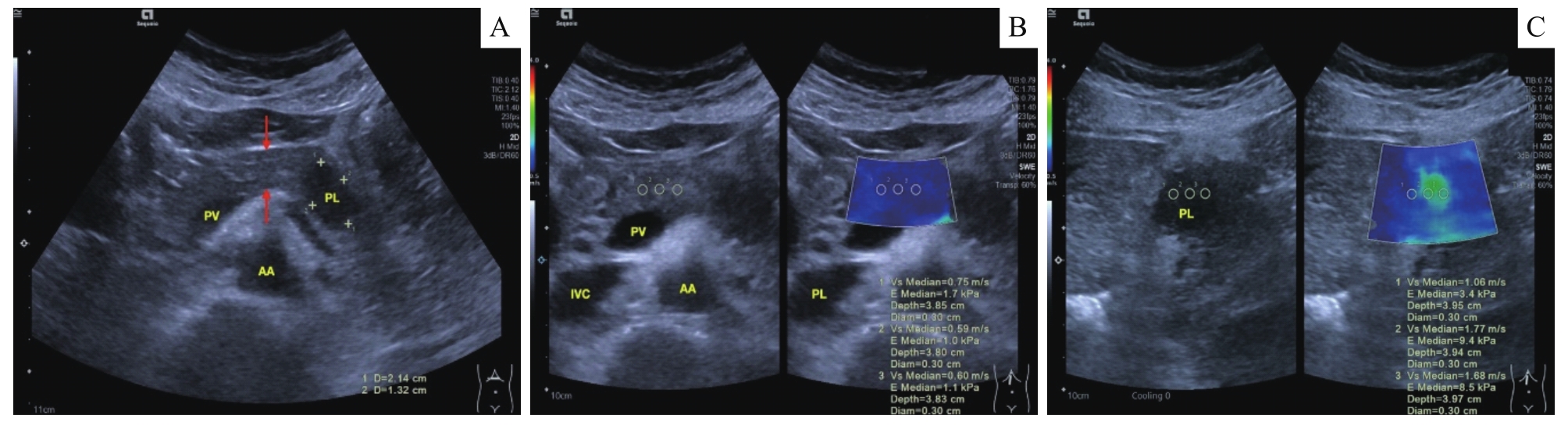
TIAN X F, KUANG T T, DONG Y, et al. Prediction of pancreatic fistula after pancreatectomy by virtual touch tissue imaging and quantification (VTIQ) technology[J]. Pancreatology, 2021, 21(8): 1498-1505.
|
| 3 |
BASSI C, MARCHEGIANI G, DERVENIS C, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after[J]. Surgery, 2017, 161(3): 584-591.
|
| 4 |
KAWAIDA H, KONO H, HOSOMURA N, et al. Surgical techniques and postoperative management to prevent postoperative pancreatic fistula after pancreatic surgery[J]. World J Gastroenterol, 2019, 25(28): 3722-3737.
|
| 5 |
WILLIAMSSON C, ANSARI D, ANDERSSON R, et al. Postoperative pancreatic fistula-impact on outcome, hospital cost and effects of centralization[J]. HPB (Oxford), 2017, 19(5): 436-442.
|
| 6 |
CALLERY M P, PRATT W B, KENT T S, et al. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy[J]. J Am Coll Surg, 2013, 216(1): 1-14.
|
| 7 |
MUNGROOP T H, VAN RIJSSEN L B, VAN KLAVEREN D, et al. Alternative fistula risk score for pancreatoduodenectomy (a-FRS): design and international external validation[J]. Ann Surg, 2019, 269(5): 937-943.
|
| 8 |
HATANO M, WATANABE J, KUSHIHATA F, et al. Quantification of pancreatic stiffness on intraoperative ultrasound elastography and evaluation of its relationship with postoperative pancreatic fistula[J]. Int Surg, 2015, 100(3): 497-502.
|
| 9 |
KUWAHARA T, HIROOKA Y, KAWASHIMA H, et al. Quantitative evaluation of pancreatic tumor fibrosis using shear wave elastography[J]. Pancreatology, 2016, 16(6): 1063-1068.
|
| 10 |
罗海峰, 高雪, 杜渐, 等. 胰十二指肠切除术后胰瘘发生的危险因素分析[J]. 中华消化外科杂志, 2017, 16(10): 1036-1041.
|
|
LUO H F, GAO X, DU J, et al. Analysis of risk factors of postoperative pancreatic fistula after pancreaticoduodenectomy[J]. Chinese Journal of Digestive Surgery, 2017, 16(10): 1036-1041.
|
| 11 |
TAJIMA Y, KAWABATA Y, HIRAHARA N. Preoperative imaging evaluation of pancreatic pathologies for the objective prediction of pancreatic fistula after pancreaticoduodenectomy[J]. Surg Today, 2018, 48(2): 140-150.
|
| 12 |
LEE T K, KANG C M, PARK M S, et al. Prediction of postoperative pancreatic fistulas after pancreatectomy: assessment with acoustic radiation force impulse elastography[J]. J Ultrasound Med, 2014, 33(5): 781-786.
|
| 13 |
SHI H Y, LU Z P, LI M N, et al. Dual-energy CT iodine concentration to evaluate postoperative pancreatic fistula after pancreatoduodenectomy[J]. Radiology, 2022, 304(1): 65-72.
|
| 14 |
YOON J H, LEE J M, LEE K B, et al. Pancreatic steatosis and fibrosis: quantitative assessment with preoperative multiparametric MR imaging[J]. Radiology, 2016, 279(1): 140-150.
|
| 15 |
FUJITA Y, KITAGO M, ABE T, et al. Evaluation of pancreatic fibrosis with acoustic radiation force impulse imaging and automated quantification of pancreatic tissue components[J]. Pancreas, 2018, 47(10): 1277-1282.
|
 ), DONG Yi1,2(
), DONG Yi1,2(