A meta-analysis of prevalence of mouth opening restriction in patients with oral cancer
YANG Ling,1,2, HOU Lili,2,3, ZHAO Yan2,3, CHEN Weihong1,2, ZHANG Jinfeng4, MAO Yan4
1.Chengdu University of Traditional Chinese Medicine School of Nursing, Chengdu 610075, China
2.Department of Nursing, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
3.Shanghai Jiao Tong University School of Nursing, Shanghai 200025, China
4.Department of Oral Maxillofacial & Head and Neck Oncology, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine; College of Stomatology, Shanghai Jiao Tong University; National Center for Stomatology; National Clinical Research Center for Oral Diseases; Shanghai Key Laboratory of Stomatology, Shanghai 200011, China
目的·通过meta分析研究口腔癌患者张口受限患病率。方法·检索中国知网(CNKI)、中文科技期刊数据库(VIP)、万方数据知识服务平台(Wanfang)、中国生物医学文献数据库(CBM)、PubMed、Ovid、EMbase、Cochrane Library、Web of Science/SciSearch、ClinicalTrials.gov数据库关于口腔癌患者张口受限患病率的观察性研究(包括前瞻性研究、回顾性研究以及横断面研究),检索时限为建库到2022年4月30日。由2位研究人员按照纳入与排除标准对所获文献独立进行筛选、提取,采用非随机对照试验方法学评价指标(methodological index for non-randomized studies,MINORS)进行文献质量评价。以张口受限患病率为结局指标合并数据,采用Stata 15.0软件进行meta分析,并根据检测时间、肿瘤部位和肿瘤分期进行亚组分析。使用GRADE profiler 3.6软件,依据GRADE(Grading of Recommendations Assessment, Development,and Evaluation)证据质量分级系统对结局指标的证据质量进行评价。结果·初检共获得3 719篇文献,最终纳入18篇文献,包括2 701例调查对象。Meta分析结果显示,口腔癌患者张口受限总患病率为42.7%(95%CI 27.0%~59.1%)。亚组分析结果显示,手术前、术后3个月、术后6个月和术后1年及以上的口腔癌患者张口受限患病率分别为29.6%(95%CI 9.0%~55.8%)、75.2%(95%CI 68.3%~81.5%)、59.1%(95%CI 38.8%~77.9%)、22.3%(95%CI 2.0%~54.3%)。T1~T2期和T3~T4期口腔癌患者张口受限患病率分别为38.6%(95%CI 26.0%~52.0%)、99.6%(95%CI 93.9%~100.0%)。磨牙后三角区、牙龈、舌部、唾液腺、口底和唇部口腔癌患者张口受限患病率分别为93.1%(95%CI 68.5%~100.0%)、68.1%(95%CI 52.9%~81.7%)、46.1%(95%CI 11.6%~82.7%)、26.1%(95%CI 15.9%~37.5%)、21.9%(95%CI 0.7%~54.0%)、3.1%(95%CI 0~9.3%)。GRADE证据质量分级系统表明结局指标的证据质量为极低。结论·口腔癌患者张口受限总患病率较高,近50%;其中术后3个月、术后6个月、T3~T4期或肿瘤位于磨牙后三角区的患者患病率更高。
关键词:口腔肿瘤
;
张口受限
;
患病率
;
meta分析
Abstract
Objective ·To study the prevalence of mouth opening restriction in oral cancer patients by meta-analysis. Methods ·China National Knowledge Infrastructure (CNKI), Chinese Science and Technology Journal Database (VIP), Wanfang Data (Wanfang), Chinese BioMedical Literature Database (CBM), PubMed, Ovid, EMbase, Cochrane Library, Web of Science/SciSearch, and ClinicalTrials.gov were searched for observational studies about the prevalence rate of restricted mouth opening in oral cancer patients (including prospective, retrospective, and cross-sectional studies). The time limit for retrieval was from the database establishment to April 30th, 2022. The obtained documents were independently screened and extracted according to the inclusion and exclusion criteria, and the literature quality evaluation was performed by using methodological index for non-randomized studies (MINORS). The data were combined with the mouth-opening-restricted prevalence rate as the outcome indicator, the meta-analysis was performed by using Stata 15.0 software, and the subgroup analysis was performed based on the detection time, tumor site, and tumor stage. The evidence quality of outcome indicators was evaluated by using GRADE profiler 3.6 software according to GRADE (Grading of Recommendations Assessment, Development, and Evaluation) system. Results ·A total of 3 719 documents were obtained during the initial examination, and 18 documents were finally included, including 2 701 objects. The meta-analysis results showed that the total prevalence rate of mouth opening restriction in oral cancer patients was 42.7% (95%CI 27.0%‒59.1%). The results of subgroup analysis showed that the prevalence rates of mouth opening restriction in patients with oral cancer before surgery, and 3 months, 6 months and 1 year or more after surgery were 29.6% (95%CI 9.0%‒55.8%), 75.2% (95%CI 68.3%‒81.5%), 59.1% (95%CI 38.8%‒77.9%) and 22.3% (95%CI 2.0%‒54.3%), respectively. The prevalence rates of mouth opening restriction in patients with oral cancer at T1‒T2 stage and T3‒T4 stage were 38.6% (95%CI 26.0%‒52.0%) and 99.6% (95%CI 93.9%‒100.0%) respectively. The prevalence rates of mouth opening restriction in patients with oral cancer in the retromolar triangle, the gingiva, the tongue, the salivary gland, the floor of mouth and the lip were 93.1% (95%CI 68.5%‒100.0%), 68.1% (95%CI 52.9%‒81.7%), 46.1% (95%CI 11.6%‒82.7%), 26.1% (95%CI 15.9%‒37.5%), 21.9% (95%CI 0.7%‒54.0%), and 3.1% (95%CI 0‒9.3%), respectively. The GRADE system for evidence quality grading indicated that the quality of evidence for outcome indicator was extremely low. Conclusion ·The total prevalence rate of mouth opening restriction in patients with oral cancer is high, nearly 50%; the patients at 3 months after surgery, at 6 months after surgery, at T3‒T4 stage or whose tumor located in the retromolar triangle have higher prevalence rates.
YANG Ling, HOU Lili, ZHAO Yan, CHEN Weihong, ZHANG Jinfeng, MAO Yan. A meta-analysis of prevalence of mouth opening restriction in patients with oral cancer. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(1): 61-69 doi:10.3969/j.issn.1674-8115.2023.01.008
对纳入研究进行单个率的meta分析,由于纳入研究缺乏对照组,故采用非随机对照试验方法学评价指标(methodological index for non-randomized studies,MINORS)进行文献质量评价[7]。该评价体系由SLIM等制定,共12条评价指标,如果针对无对照组的研究,评价指标仅8条;每1条分值为0~2分,总分为16分。计分方法:0分代表未报道,1分代表有报道但数据不充分,2分代表信息完整。由2位研究者根据评分标准,独立进行评价[8]。
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages.
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes.
在对口腔癌患者张口受限总患病率进行合并时,发现纳入文献存在较大的异质性。因此,本研究根据不同检测时间、肿瘤部位、肿瘤分期,对纳入研究进行亚组分析。亚组分析的异质性检验结果显示,除了术前、术后3个月、术后1年及以上和舌部的口腔癌患者张口受限患病率异质性仍较高,其余各组异质性均明显下降,据此进行亚组分析能够在一定程度上降低组内异质性。本研究发现,不同检测时间、肿瘤分期和肿瘤部位的口腔癌患者张口受限患病率有明显差异。就检测时间而言,口腔癌患者张口受限患病率,在最初就诊时最低,在术后3~6个月上升,在术后1年以后有所下降。WATTERS等[34]的研究也得到了类似的结果:头颈肿瘤张口受限的患病率从基线时的17.3%,上升至6个月时的44.1%,1年后下降至36.1%,3年后下降至32.6%。这可能与术后放疗有关:由于放疗可引起咀嚼肌纤维化,并持续数月,进而导致肌肉组织挛缩,造成张口受限;同时放疗引起的局部血流灌注损失也可加重张口受限[29-30,35]。放疗剂量越高,张口受限越严重,超过60 Gy的水平更容易引起张口受限。与首次接受治疗的患者相比,接受过放疗且目前正在进行放疗的患者出现张口受限的风险更高[29,36]。就肿瘤分期而言,处于早期阶段的口腔癌张口受限患病率较低,处于晚期阶段的口腔癌张口受限患病率高。VAN DER GEER等[20]发现,肿瘤的体积是发生张口受限的影响因素。较大的口腔肿瘤通常涉及部分颌骨切除。下颌骨是颌面部骨中唯一可活动的骨骼,参与构成颌面部下1/3的轮廓外形,在对舌体、下颌牙列以及口底肌肉的支撑中起主要作用,确保咀嚼、吞咽和呼吸等运动的正常进行[37]。因此部分颌骨的切除可能会导致口腔癌患者张口受限。就肿瘤部位而言,各个部位张口受限的患病率各不相同,但高发部位都位于颞下颌关节。这可能由于颞下颌关节的原发性或转移性肿瘤可导致关节结构破坏,使关节无法正常旋转和平移[38-40]。
HOU Lili, YANG Ling and ZHAO Yan were responsible for the conception and design of the research; YANG Ling and ZHAO Yan were responsible for literature retrieval; YANG Ling and CHEN Weihong were responsible for data extraction and statistical analysis; MAO Yan and ZHANG Jinfeng were responsible for literature quality evaluation; YANG Ling was responsible for thesis writing; ZHAO Yan and MAO Yan were responsible for thesis revision; HOU Lili was responsible for the final review of the paper. All the authors have read and agreed to the submission of the final manuscript.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249.
JOHNSON J, VAN AS-BROOKS C J, FAGERBERG-MOHLIN B, et al. Trismus in head and neck cancer patients in Sweden: incidence and risk factors[J]. Med Sci Monit, 2010, 16(6): CR278-CR282.
LEE L Y, CHEN S C, CHEN W C, et al. Postradiation trismus and its impact on quality of life in patients with head and neck cancer[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2015, 119(2): 187-195.
GARCÍA-PERIS P, PARÓN L, VELASCO C, et al. Long-term prevalence of oropharyngeal dysphagia in head and neck cancer patients: impact on quality of life[J]. Clin Nutr, 2007, 26(6): 710-717.
SLIM K, NINI E, FORESTIER D, et al. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument[J]. ANZ J Surg, 2003, 73(9): 712-716.
ZENG X T, ZHUANG L P, YANG Z G, et al. Meta-analysis series, 7: quality assessment tools for non-randomized experimental studies, diagnostic tests and animal experiments[J]. Chinese Journal of Evidence-Based Cardiovascular Medicine, 2012, 4(6): 496-499.
FU S, FAN L N, ZHOU W T. Clinical research for preoperative chemotherapy, radiotherapy combined with surgery to treat middle-late squamous cell carcinoma of oral[J]. Journal of Clinical Stomatology, 2014, 30(10): 619-622.
GONDIVKAR S M, GADBAIL A R, SARODE S C, et al. Prevalence of trismus and its impact on oral health-related quality of life in patients treated for oral squamous cell carcinoma[J]. Asian Pac J Cancer Prev, 2021, 22(8): 2437-2444.
MARTINS C A, GOLDENBERG D C, NARIKAWA R, et al. Trismus and oral health conditions during diagnosis of malignant oral neoplasms[J]. Braz J Otorhinolaryngol, 2020, 86(5): 552-557.
PANTVAIDYA G, SIVASANKER M, RANGANATHAN P, et al. Prospective cross-sectional study assessing prevalence and factors affecting trismus after multimodal treatment for oral cancers[J]. Head Neck, 2019, 41(2): 286-290.
AGARWAL P, SHIVA KUMAR H R, RAI K K. Trismus in oral cancer patients undergoing surgery and radiotherapy[J]. J Oral Biol Craniofac Res, 2016, 6(Suppl 1): S9-S13.
MINHAS S, KASHIF M, ALTAF W, et al. Concomitant-chemoradiotherapy-associated oral lesions in patients with oral squamous-cell carcinoma[J]. Cancer Biol Med, 2017, 14(2): 176-182.
OWOSHO A A, PEDREIRA RAMALHO L M, ROSENBERG H I, et al. Objective assessment of trismus in oral and oropharyngeal cancer patients treated with intensity-modulated radiation therapy (IMRT)[J]. J Craniomaxillofac Surg, 2016, 44(9): 1408-1413.
SCOTT B, D'SOUZA J, PERINPARAJAH N, et al. Longitudinal evaluation of restricted mouth opening (trismus) in patients following primary surgery for oral and oropharyngeal squamous cell carcinoma[J]. Br J Oral Maxillofac Surg, 2011, 49(2): 106-111.
WETZELS J W G H, MERKX M A W, DE HAAN A F J, et al. Maximum mouth opening and trismus in 143 patients treated for oral cancer: a 1-year prospective study[J]. Head Neck, 2014, 36(12): 1754-1762.
HSIEH L C, CHEN J W, WANG LY, et al. Predicting the severity and prognosis of trismus after intensity-modulated radiation therapy for oral cancer patients by magnetic resonance imaging[J]. PLoS One, 2014, 9(3): e92561.
VAN DER GEER S J, VAN RIJN P V, KAMSTRA J I, et al. Prevalence and prediction of trismus in patients with head and neck cancer: a cross-sectional study[J]. Head Neck, 2019, 41(1): 64-71.
STEINER F, EVANS J, MARSH R, et al. Mouth opening and trismus in patients undergoing curative treatment for head and neck cancer[J]. Int J Oral Maxillofac Surg, 2015, 44(3): 292-296.
ASTRADSSON T, LAURELL G, AHLBERG A, et al. Trismus in patients with head and neck cancer and 5-year overall survival[J]. Acta Otolaryngol, 2018, 138(12): 1123-1127.
PEI-LING K, TSAE-JYY W, MING-HSIOU L, et al. Trismus and its influencing factors in oral cancer patients[J]. Supportive Care Cancer, 2019, 27(Suppl 1): S58-S59.
BATISTA D P F, BAGAROLLO M F, NAGAE M H. Airway management of patients undergoing oral cancer surgery: a retrospective study[J]. Int Arch Otorhinolaryngol, 2017, 21(S112): 2.
NIKHAR S A, SHARMA A, RAMDASPALLY M, et al. Airway management of patients undergoing oral cancer surgery: a retrospective analysis of 156 patients[J]. Turk J Anaesthesiol Reanim, 2017, 45(2): 108-111.
LEE R, SLEVIN N, MUSGROVE B, et al. Prediction of post-treatment trismus in head and neck cancer patients[J]. Br J Oral Maxillofac Surg, 2012, 50(4): 328-332.
PAULI N, JOHNSON J, FINIZIA C, et al. The incidence of trismus and long-term impact on health-related quality of life in patients with head and neck cancer[J]. Acta Oncol, 2013, 52(6): 1137-1145.
RAPIDIS A D, DIJKSTRA P U, ROODENBURG J L N, et al. Trismus in patients with head and neck cancer: etiopathogenesis, diagnosis and management[J]. Clin Otolaryngol, 2015, 40(6): 516-526.
LOH S Y, MCLEOD R W J, ELHASSAN H A. Trismus following different treatment modalities for head and neck cancer: a systematic review of subjective measures[J]. Eur Arch Otorhinolaryngol, 2017, 274(7): 2695-2707.
BENSADOUN R J, RIESENBECK D, LOCKHART P B, et al. A systematic review of trismus induced by cancer therapies in head and neck cancer patients[J]. Support Care Cancer, 2010, 18(8): 1033-1038.
TANG Y, SHEN Q, WANG Y, et al. A randomized prospective study of rehabilitation therapy in the treatment of radiation-induced dysphagia and trismus[J]. Strahlenther Onkol, 2011, 187(1): 39-44.
WATTERS A L, COPE S, KELLER M N, et al. Prevalence of trismus in patients with head and neck cancer: a systematic review with meta-analysis[J]. Head Neck, 2019, 41(9): 3408-3421.
CHAN Y W, CHOW V L Y, WEI W I. Quality of life of patients after salvage nasopharyngectomy for recurrent nasopharyngeal carcinoma[J]. Cancer, 2012, 118(15): 3710-3718.
CHEN H W. Research on the effect of remote supervision and guidance on postoperative masticatory function rehabilitation training in patients with oral tumors[D]. Shenyang: China Medical University, 2020.
KRUSE A L D, LUEBBERS H T, OBWEGESER J A, et al. Temporomandibular disorders associated with metastases to the temporomandibular joint: a review of the literature and 3 additional cases[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2010, 110(2): e21-e28.
HAN Z X, CHEN M J, YANG C, et al. Recurrent synovial chondromatosis of the temporomandibular joint: report of two cases[J]. Br J Oral Maxillofac Surg, 2017, 55(9): 965-967.
ABBOUD W, YAHALOM R, LEIBA M, et al. Temporomandibular joint involvement in patients with multiple myeloma: a retrospective study[J]. Int J Oral Maxillofac Surg, 2016, 45(12): 1545-1550.
CHEE S Z, BYRNES Y M, CHORATH K T, et al. Interventions for trismus in head and neck cancer patients: a systematic review of randomized controlled trials[J]. Integr Cancer Ther, 2021, 20: 15347354211006474.
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... 对纳入研究进行单个率的meta分析,由于纳入研究缺乏对照组,故采用非随机对照试验方法学评价指标(methodological index for non-randomized studies,MINORS)进行文献质量评价[7].该评价体系由SLIM等制定,共12条评价指标,如果针对无对照组的研究,评价指标仅8条;每1条分值为0~2分,总分为16分.计分方法:0分代表未报道,1分代表有报道但数据不充分,2分代表信息完整.由2位研究者根据评分标准,独立进行评价[8]. ...
1
... 对纳入研究进行单个率的meta分析,由于纳入研究缺乏对照组,故采用非随机对照试验方法学评价指标(methodological index for non-randomized studies,MINORS)进行文献质量评价[7].该评价体系由SLIM等制定,共12条评价指标,如果针对无对照组的研究,评价指标仅8条;每1条分值为0~2分,总分为16分.计分方法:0分代表未报道,1分代表有报道但数据不充分,2分代表信息完整.由2位研究者根据评分标准,独立进行评价[8]. ...
1
... 对纳入研究进行单个率的meta分析,由于纳入研究缺乏对照组,故采用非随机对照试验方法学评价指标(methodological index for non-randomized studies,MINORS)进行文献质量评价[7].该评价体系由SLIM等制定,共12条评价指标,如果针对无对照组的研究,评价指标仅8条;每1条分值为0~2分,总分为16分.计分方法:0分代表未报道,1分代表有报道但数据不充分,2分代表信息完整.由2位研究者根据评分标准,独立进行评价[8]. ...
1
... 使用GRADE profiler 3.6软件,依据GRADE(Grading of Recommendations Assessment,Development,and Evaluation)证据质量分级系统对结局指标的证据质量进行评价[9].主要从5个方面进行评价:偏倚性、不一致性、间接性、精确性和发表偏倚.证据质量分级包括高、中、低和极低4个等级. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
2
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
4
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
4
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
3
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... 在对口腔癌患者张口受限总患病率进行合并时,发现纳入文献存在较大的异质性.因此,本研究根据不同检测时间、肿瘤部位、肿瘤分期,对纳入研究进行亚组分析.亚组分析的异质性检验结果显示,除了术前、术后3个月、术后1年及以上和舌部的口腔癌患者张口受限患病率异质性仍较高,其余各组异质性均明显下降,据此进行亚组分析能够在一定程度上降低组内异质性.本研究发现,不同检测时间、肿瘤分期和肿瘤部位的口腔癌患者张口受限患病率有明显差异.就检测时间而言,口腔癌患者张口受限患病率,在最初就诊时最低,在术后3~6个月上升,在术后1年以后有所下降.WATTERS等[34]的研究也得到了类似的结果:头颈肿瘤张口受限的患病率从基线时的17.3%,上升至6个月时的44.1%,1年后下降至36.1%,3年后下降至32.6%.这可能与术后放疗有关:由于放疗可引起咀嚼肌纤维化,并持续数月,进而导致肌肉组织挛缩,造成张口受限;同时放疗引起的局部血流灌注损失也可加重张口受限[29-30,35].放疗剂量越高,张口受限越严重,超过60 Gy的水平更容易引起张口受限.与首次接受治疗的患者相比,接受过放疗且目前正在进行放疗的患者出现张口受限的风险更高[29,36].就肿瘤分期而言,处于早期阶段的口腔癌张口受限患病率较低,处于晚期阶段的口腔癌张口受限患病率高.VAN DER GEER等[20]发现,肿瘤的体积是发生张口受限的影响因素.较大的口腔肿瘤通常涉及部分颌骨切除.下颌骨是颌面部骨中唯一可活动的骨骼,参与构成颌面部下1/3的轮廓外形,在对舌体、下颌牙列以及口底肌肉的支撑中起主要作用,确保咀嚼、吞咽和呼吸等运动的正常进行[37].因此部分颌骨的切除可能会导致口腔癌患者张口受限.就肿瘤部位而言,各个部位张口受限的患病率各不相同,但高发部位都位于颞下颌关节.这可能由于颞下颌关节的原发性或转移性肿瘤可导致关节结构破坏,使关节无法正常旋转和平移[38-40]. ...
4
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
4
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... Basic characteristics of the included studiesTab 1
Study
Research type
Population
n
Outcome index
FU, et al (2014)[10]
Prospective study
Oral cancer patients
104
①②
GONDIVKAR, et al (2021)[11]
Prospective study
Oral cancer patients
100
①②③④
MARTINS, et al (2020)[12]
Prosepctive study
Oral cancer patients
35
①③
PANTVAIDYA, et al (2019)[13]
Prosepctive study
Oral cancer patients
401
①②
AGARWAL, et al (2016)[14]
Prosepctive study
Oral cancer patients
30
②③④
MINHAS, et al (2017)[15]
Cross-sectional study
Patients with oral squamous cell carcinoma
81
①
OWOSHO, et al (2016)[16]
Retrospectivel study
Oral cancer patients
54
①③
SCOTT, et al (2011)[17]
Prosepctive study
Oral cancer patients
98
②
WETZELS, et al (2014)[18]
Prospective study
Oral cancer patients
143
②
HSIEH, et al (2014)[19]
Prospective study
Patients with oral squamous cell carcinoma
22
①
VAN DER GEER, et al (2019)[20]
Cross-sectional study
Oral cancer patients
730
③
STEINER, et al (2015)[21]
Prospective study
Oral cancer patients
45
①
ASTRADSSON, et al (2018)[22]
Prospective study
Oral cancer patients
27
①②
JOHNSON, et al (2010)[3]
Prospective study
Oral cancer patients
246
③
PEI-LING, et al (2019)[23]
Cross-sectional study
Oral cancer patients
69
②
BATISTA, et al (2017)[24]
Prospective study
Oral cancer patients
100
①
NIKHAR, et al (2017)[25]
Prospective study
Oral cancer patients
156
①
MISHRA, et al (2005)[26]
Prospective study
Oral cancer patients
260
①
Note: ① The overall rate of mouth opening restriction. ② The rates of mouth opening restriction at different time points. ③ The rates of mouth opening restriction of the patients with lesions in different locations. ④ The rates of mouth opening restriction of the patients with different TNM tumor stages. ...
... Quality evaluation results of the included studiesTab 2
Study
Score of item/point
Total score of MINORS/point
①
②
③
④
⑤
⑥
⑦
⑧
FU, et al (2014)[10]
2
2
2
2
0
2
2
0
12
GONDIVKAR, et al (2021)[11]
2
2
2
2
0
0
2
2
12
MARTINS, et al (2020)[12]
2
2
2
2
0
2
2
0
12
PANTVAIDYA, et al (2019)[13]
2
2
2
2
0
2
2
0
12
AGARWAL, et al (2016)[14]
2
2
2
2
0
2
2
0
12
MINHAS, et al (2017)[15]
2
2
2
2
0
2
2
0
12
OWOSHO, et al (2016)[16]
2
2
2
2
0
0
2
2
12
SCOTT, et al (2011)[17]
2
2
2
2
0
2
2
0
12
WETZELS, et al (2014)[18]
2
2
2
2
0
2
2
0
12
HSIEH, et al (2014)[19]
2
2
2
2
0
2
2
0
12
VAN DER GEER, et al (2019)[20]
2
2
2
2
0
2
2
0
12
STEINER, et al (2015)[21]
2
2
2
2
0
2
2
0
12
ASTRADSSON, et al (2018)[22]
2
0
2
2
0
0
2
2
10
JOHNSON, et al (2010)[3]
2
2
2
2
0
2
2
0
12
PEI-LING, et al (2019)[23]
2
2
2
2
0
2
2
0
12
BATISTA, et al (2017)[24]
2
2
2
2
0
0
0
0
8
NIKHAR, et al (2017)[25]
2
2
2
2
0
2
2
0
12
MISHRA, et al (2005)[26]
2
2
2
2
0
2
2
0
12
Note: ① A clearly stated aim: the question addressed should be precise and relevant in the light of available literature. ② Inclusion of consecutive patients: all patients potentially fit for inclusion (satisfying the criteria for inclusion) have been included in the study during the study period (no exclusion or details about the reasons for exclusion). ③ Prospective collection of data: data were collected according to a protocol established before the beginning of the study. ④ Endpoints appropriate to the aim of the study: unambiguous explanation of the criteria was used to evaluate the main outcome which should be in accordance with the question addressed by the study. Also the endpoints should be assessed on an intention-to-treat basis. ⑤ Unbiased assessment of the study endpoint: blind evaluation of objective endpoints and double-blind evaluation of subjective endpoints. Otherwise the reasons for not blinding should be stated. ⑥ Follow-up period appropriate to the aim of the study: the follow-up should be sufficiently long to allow the assessment of the main endpoint and possible adverse events. ⑦ Loss to follow up less than 5%: all patients should be included in the follow up. Otherwise the proportion lost to follow up should not exceed the proportion experiencing the major endpoint. ⑧ Prospective calculation of the study size: information of the size of detectable difference of interest with a calculation of 95% confidence interval according to the expected incidence of the outcome event, and information about the level for statistical significance and estimates of power when comparing the outcomes. ...
... 在对口腔癌患者张口受限总患病率进行合并时,发现纳入文献存在较大的异质性.因此,本研究根据不同检测时间、肿瘤部位、肿瘤分期,对纳入研究进行亚组分析.亚组分析的异质性检验结果显示,除了术前、术后3个月、术后1年及以上和舌部的口腔癌患者张口受限患病率异质性仍较高,其余各组异质性均明显下降,据此进行亚组分析能够在一定程度上降低组内异质性.本研究发现,不同检测时间、肿瘤分期和肿瘤部位的口腔癌患者张口受限患病率有明显差异.就检测时间而言,口腔癌患者张口受限患病率,在最初就诊时最低,在术后3~6个月上升,在术后1年以后有所下降.WATTERS等[34]的研究也得到了类似的结果:头颈肿瘤张口受限的患病率从基线时的17.3%,上升至6个月时的44.1%,1年后下降至36.1%,3年后下降至32.6%.这可能与术后放疗有关:由于放疗可引起咀嚼肌纤维化,并持续数月,进而导致肌肉组织挛缩,造成张口受限;同时放疗引起的局部血流灌注损失也可加重张口受限[29-30,35].放疗剂量越高,张口受限越严重,超过60 Gy的水平更容易引起张口受限.与首次接受治疗的患者相比,接受过放疗且目前正在进行放疗的患者出现张口受限的风险更高[29,36].就肿瘤分期而言,处于早期阶段的口腔癌张口受限患病率较低,处于晚期阶段的口腔癌张口受限患病率高.VAN DER GEER等[20]发现,肿瘤的体积是发生张口受限的影响因素.较大的口腔肿瘤通常涉及部分颌骨切除.下颌骨是颌面部骨中唯一可活动的骨骼,参与构成颌面部下1/3的轮廓外形,在对舌体、下颌牙列以及口底肌肉的支撑中起主要作用,确保咀嚼、吞咽和呼吸等运动的正常进行[37].因此部分颌骨的切除可能会导致口腔癌患者张口受限.就肿瘤部位而言,各个部位张口受限的患病率各不相同,但高发部位都位于颞下颌关节.这可能由于颞下颌关节的原发性或转移性肿瘤可导致关节结构破坏,使关节无法正常旋转和平移[38-40]. ...
... [29,36].就肿瘤分期而言,处于早期阶段的口腔癌张口受限患病率较低,处于晚期阶段的口腔癌张口受限患病率高.VAN DER GEER等[20]发现,肿瘤的体积是发生张口受限的影响因素.较大的口腔肿瘤通常涉及部分颌骨切除.下颌骨是颌面部骨中唯一可活动的骨骼,参与构成颌面部下1/3的轮廓外形,在对舌体、下颌牙列以及口底肌肉的支撑中起主要作用,确保咀嚼、吞咽和呼吸等运动的正常进行[37].因此部分颌骨的切除可能会导致口腔癌患者张口受限.就肿瘤部位而言,各个部位张口受限的患病率各不相同,但高发部位都位于颞下颌关节.这可能由于颞下颌关节的原发性或转移性肿瘤可导致关节结构破坏,使关节无法正常旋转和平移[38-40]. ...


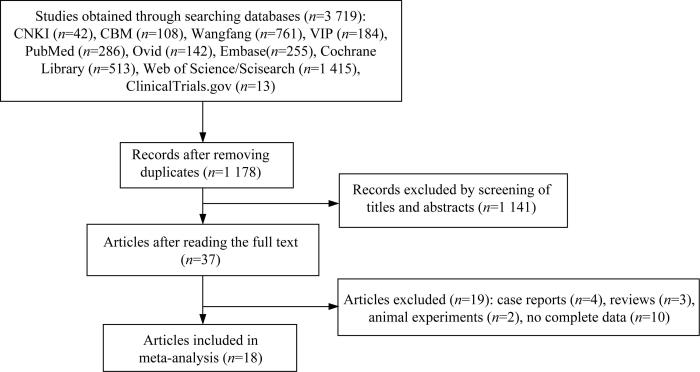
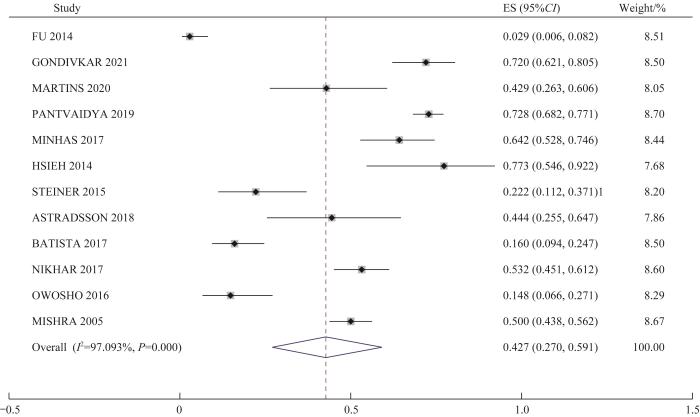
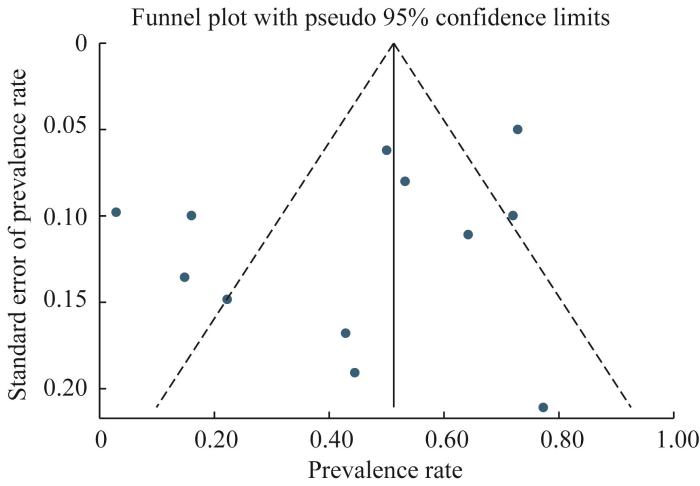

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}