目的·探讨急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)血管内治疗(endovascular therapy,EVT)的早期有效性和安全性。方法·回顾性连续纳入2016年6月—2022年10月在上海交通大学医学院附属第六人民医院脑卒中绿色通道收治的急诊EVT辅助标准内科治疗的31例LVO-MIS患者(EVT组),以及同期仅采用标准内科治疗的32例LVO-MIS患者(对照组)。收集2组患者的一般临床资料和血管内治疗相关资料。其中,主要结局为早期有效,即治疗后第7日美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分(NIHSS at seventh day after treatment,d7NIHSS)较基线NIHSS评分下降≥3分或直接下降到0分;次要结局包括血管成功再通、早期神经功能恶化;安全性评价包括症状性颅内出血、死亡。对2组患者的主要结局、次要结局进行分析,以评估EVT早期有效性。对2组患者的安全性评价指标进行分析,以评估EVT的安全性。采用Kruskal-Wallis H检验对EVT组中24例实际行EVT的患者治疗前后的NIHSS评分进行分析。结果·2组患者的一般临床资料以及闭塞部位、发病至入院时间等血管内治疗相关资料间差异均无统计学意义。EVT组患者的基线NIHSS评分[5.0(3.0,5.0)分]高于对照组[3.5(2.0,5.0)分](P=0.001),其d7NIHSS评分[1.0(0,3.0)分]低于对照组[2.0(1.0,5.8)分](P=0.040)。2组患者中共有24例(38.1%)患者达早期有效,其中EVT组16例、对照组8例;且EVT组的有效率较对照组更高(χ2=4.729,P=0.030)。EVT组患者的早期神经功能恶化率较对照组更低(χ2 =6.097,P=0.014),且EVT组中血管成功再通为29例(93.5%)。2组患者在症状性颅内出血率、死亡率间差异无统计学意义。EVT组中,24例患者基线NIHSS评分[5.0(3.0,5.0)分]、术后24 h的NIHSS评分[2.0(0.3,3.8)分]、d7NIHSS评分[1.0(0,2.8)分]间差异具有统计学意义(H=16.997,P=0.000)。结论·血管内治疗LVO-MIS是安全有效的;该疗法的早期效果优于标准内科治疗,早期神经功能恶化率更低且不增加症状性颅内出血的风险。
关键词:轻型卒中
;
大血管闭塞
;
血管内治疗
;
早期神经功能恶化
Abstract
Objective ·To investigate the early efficiency and safety of endovascular therapy (EVT) for patients with acute mild ischemic stroke with large vessel occlusion (LVO-MIS). Methods ·A total of 31 patients with LVO-MIS who received emergency EVT-assisted standard medical treatment at the Green Channel of Stroke in Shanghai Sixth People's Hospital, Shanghai Jiao Tong University School of Medicine from June 2016 to October 2022 were retrospectively included as endovascular therapy group (EVT group), and 32 LVO-MIS patients who only received standard medical treatment in the same period were selected as the control group. General clinical data and parameters related to EVT of the two groups were collected. The primary outcome was early efficacy, that is, the NIHSS at seventh day after treatment (d7NIHSS) score decreased by ≥3 points or directly to 0 points from baseline NIHSS score. Secondary outcomes included successful revascularization of blood vessels and early neurological deterioration (END), and safety outcomes included symptomatic intracranial hemorrhage (sICH) and mortality. The primary and secondary outcomes of the two groups of patients were analyzed to evaluate the early efficiency of EVT, and the safety evaluation indicators of the two groups of patients were analyzed to evaluate the safety of EVT. Kruskal-Wallis H test was used to analyze the NIHSS scores of 24 patients in the EVT group who underwent EVT before and after treatment. Results ·There was no statistically significant difference in the general clinical data between the two groups, as well as parameters related to EVT such as occlusion site, and onset-to-admission time. The baseline NIHSS score of the EVT group [5.0 (3.0, 5.0) points] was higher than that of the control group [3.5 (2.0, 5.0) points] (P=0.001), and their d7NIHSS score [1.0 (0, 3.0) points] was lower than that of the control group [2.0 (1.0, 5.8) points] (P=0.040). A total of 24 patients (38.1%) in the two groups achieved early efficacy, including 16 cases in the EVT group and 8 cases in the control group; and the early efficacy rate of the EVT group was higher than that of the control group (χ2=4.729, P=0.030). The END rate in the EVT group was lower than that in the control group (χ2 =6.097, P=0.014), and there were 29 cases (93.5%) in the EVT group of patients whose blood vessels were successfully reopened. There was no statistically significant difference in sICH rate and mortality rate between the two groups. In the EVT group, there was a statistically significant difference (H=16.997, P=0.000) among the baseline NIHSS scores [5.0 (3.0, 5.0) points] of 24 patients, postoperative 24hNIHSS score [2.0 (0.3, 3.8) points] and d7NIHSS scores [1.0 (0, 2.8) points]. Conclusion ·EVT is safe and effective in treating LVO-MIS, and the early efficacy rate of EVT is superior to standard medicine treatment, with a lower rate of END and no increased risk of sICH.
Keywords:mild ischemic stroke
;
large vessel occlusion (LVO)
;
endovascular therapy (EVT)
;
early neurological deterioration (END)
NI Ruilong, ZHAO Fei, CAO Li, DENG Jiangshan. Analysis of early efficacy and safety of endovascular therapy for acute mild ischemic stroke with large vessel occlusion. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(10): 1268-1273 doi:10.3969/j.issn.1674-8115.2023.10.007
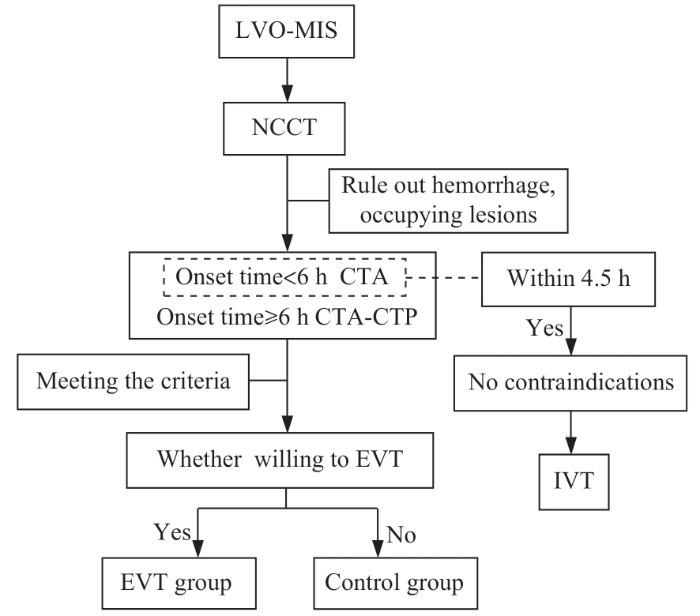
据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2]。目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议。国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高。个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似。也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力。且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9]。由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考。
Tab 1 Comparison of general clinical data and baseline characteristics related to EVT between the two groups of patients
Item
EVT group
(n=31)
Control group (n=32)
P value
Age/year
67.8±14.3
66.6±14.7
0.483
Male/n(%)
24 (77.4)
28 (87.5)
0.292
Smokinga/n(%)
10 (32.3)
10 (31.3)
0.932
Drinkinga/n(%)
8 (25.8)
8 (25.0)
0.941
Medical historyb/n(%)
Hypertension
19 (61.3)
25 (78.1)
0.146
Diabetes
8 (25.8)
8 (25.0)
0.941
Atrial fibrillation
12 (38.7)
7 (21.9)
0.146
Ischemic stroke or TIA
5 (16.1)
10 (31.3)
0.159
Coronary heart disease
1 (3.2)
4 (12.5)
0.173
Occlusion site/n(%)
ICA
5 (16.1)
7 (21.9)
0.561
MCA (M1)
21 (67.7)
16 (50.0)
0.153
MCA (M2)
2 (6.5)
2 (6.3)
0.974
VB/BA
3 (9.7)
7 (21.9)
0.185
Baseline NIHSS score/score
5.0 (3.0, 5.0)
3.5 (2.0, 5.0)
0.001
Onset-to-admission time/min
230 (70, 222)
270 (86, 436)
0.209
Note:a Current or within the prior 5 years. b Patient self-report or family report. ICA—internal carotid artery; MCA—middle cerebral artery; VB—vertebral artery; BA—basilar artery.
Tab 2 Comparison of early efficacy and safety between the two groups of patients
Outcome
EVT group (n=31)
Control group (n=32)
χ2
value
P value
Primary outcome/n(%)
Early efficiency
16 (51.6)
8 (25.0)
4.729
0.030
Secondary outcome/n(%)
mTICI 2b-3
29 (93.5)
6① (46.2)②
13.089
0.000
END
1 (3.2)
8 (25.0)
6.097
0.014
Safety outcome
sICH
1 (3.2)
1 (3.1)
0.001
0.982
Death in hospital
0
0
‒
‒
Note:①The n=6 was referred to the number of IVT patients' angiography showing revascularization in the EVT group; ②The rate of mTICI 2b-3 in the control group was referred to the IVT data of EVT group (6/13).
本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高。DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗。在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗。BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25]。本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26]。静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27]。在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌。在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡。继而提示,患者在安全性方面的组间无差异。
本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30]。在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31]。既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32]。因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义。
NI Ruilong performed the statistical analysis and drafted the manuscript. DENG Jiangshan, CAO Li and ZHAO Fei were responsible for the research design and paper revision. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
DARGAZANLI C, ARQUIZAN C, GORY B, et al. Mechanical thrombectomy for minor and mild stroke patients harboring large vessel occlusion in the anterior circulation: a multicenter cohort study[J]. Stroke, 2017, 48(12): 3274-3281.
HELDNER M R, CHALOULOS-IAKOVIDIS P, PANOS L, et al. Outcome of patients with large vessel occlusion in the anterior circulation and low NIHSS score[J]. J Neurol, 2020, 267(6): 1651-1662.
Chinese Society of Neurology, Chinese Stroke Society, Neurovascular Intervention Group of Chinese Society of Neurology Chinese. Chinese guidelines for the endovascular treatment of acute ischemic stroke 2022[J]. Chin J Neurol, 2022, 55(6): 565-580.
POWERS W J, DERDEYN C P, BILLER J, et al. 2015 American heart association/American stroke association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American heart association/American stroke association[J]. Stroke, 2015, 46(10): 3020-3035.
MANNO C, DISANTO G, BIANCO G, et al. Outcome of endovascular therapy in stroke with large vessel occlusion and mild symptoms[J]. Neurology, 2019, 93(17): e1618-e1626.
DOBROCKY T, PIECHOWIAK E I, VOLBERS B, et al. Treatment and outcome in stroke patients with acute M2 occlusion and minor neurological deficits[J]. Stroke, 2021, 52(3): 802-810.
HAUSSEN D C, LIMA F O, BOUSLAMA M, et al. Thrombectomy versus medical management for large vessel occlusion strokes with minimal symptoms: an analysis from STOPStroke and GESTOR cohorts[J]. J Neurointerv Surg, 2018, 10(4): 325-329.
WANG G F, YANG X Q, XIAO Y L, et al. Safety and efficacy of mechanical thrombectomy in minor stroke with large vessel occlusion[J]. Chin J Neuromed, 2020, 19(7): 711-714.
ALBERS G W, MARKS M P, KEMP S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging[J]. N Engl J Med, 2018, 378(8): 708-718.
Chinese Society of Neurology, Chinese Stroke Society. Chinese guidelines for diagnosis and treatment of acute ischemic stroke 2018[J]. Chin J Neurol, 2018, 51(9): 666-682.
ZAIDAT O O, YOO A J, KHATRI P, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement[J]. Stroke, 2013, 44(9): 2650-2663.
CHEN S, WANG C, WANG W, et al. Risk factors of early neurological deterioration after endovascular therapy recanalization for acute intracranial anterior circulation large vessel occlusion[J]. Chinese Journal of Cerebrovascular Diseases, 2022, 19(2): 73-78, 108.
SENERS P, BEN HASSEN W, LAPERGUE B, et al. Prediction of early neurological deterioration in individuals with minor stroke and large vessel occlusion intended for intravenous thrombolysis alone[J]. JAMA Neurol, 2021, 78(3): 321-328.
SALEEM Y, NOGUEIRA R G, RODRIGUES G M, et al. Acute neurological deterioration in large vessel occlusions and mild symptoms managed medically[J]. Stroke, 2020, 51(5): 1428-1434.
WANG G F, ZHAO X, LIU S P, et al. Efficacy and safety of mechanical thrombectomy for acute mild ischemic stroke with large vessel occlusion[J]. Med Sci Monit, 2020, 26: e926110.
TURC G, BHOGAL P, FISCHER U, et al. European Stroke Organisation (ESO)-European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke[J]. J Neurointerv Surg, 2019, 11(6): 535-538.
DA ROS V, CORTESE J, CHASSIN O, et al. Thrombectomy or intravenous thrombolysis in patients with NIHSS of 5 or less?[J]. J De Neuroradiol, 2019, 46(4): 225-230.
YANG P, ZHANG Y, ZHANG L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke[J]. N Engl J Med, 2020, 382(21): 1981-1993.
TONG X, WANG Y L, FIEHLER J, et al. Thrombectomy versus combined thrombolysis and thrombectomy in patients with acute stroke: a matched-control study[J]. Stroke, 2021, 52(5): 1589-1600.
BROEG-MORVAY A, MORDASINI P, BERNASCONI C, et al. Direct mechanical intervention versus combined intravenous and mechanical intervention in large artery anterior circulation stroke: a matched-pairs analysis[J]. Stroke, 2016, 47(4): 1037-1044.
BHATIA R, HILL M D, SHOBHA N, et al. Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: real-world experience and a call for action[J]. Stroke, 2010, 41(10): 2254-2258.
LIU L P, CHEN W Q, DUAN W Y, et al. Chinese stroke association guidelines for clinical management of cerebrovascular disorders (excerpts): clinical management of ischemic cerebrovascular disorders[J]. Chinese Journal of Stroke, 2019, 14(7): 709-726.
ZHONG W S, ZHOU Y, ZHANG K M, et al. Minor non-disabling stroke patients with large vessel severe stenosis or occlusion might benefit from thrombolysis[J]. Brain Sci, 2021, 11(7): 945.
LAU H L, GARDENER H, COUTTS S B, et al. Radiographic characteristics of mild ischemic stroke patients with visible intracranial occlusion: the INTERRSeCT study[J]. Stroke, 2022, 53(3): 913-920.
SUN X, YANG M, YU Z Q, et al. Chinese experts consensus on endovascular treatment for symptomatic intracranial atherosclerotic stenosis 2022[J]. Chinese Journal of Stroke, 2022, 17(8): 863-888.
SUN L L, ZHANG J P, SONG Y, et al. Safety and efficacy of tirofiban in rescue treatment for acute intracranial intraprocedural stent thrombosis[J]. Front Neurol, 2020, 11: 492.
RESCUE BT Trial Investigators, QIU Z M, LI F L, et al. Effect of intravenous tirofiban vs placebo before endovascular thrombectomy on functional outcomes in large vessel occlusion stroke: the RESCUE BT randomized clinical trial[J]. JAMA, 2022, 328(6): 543-553.
CAMPBELL B C, CHRISTENSEN S, TRESS B M, et al. Failure of collateral blood flow is associated with infarct growth in ischemic stroke[J]. J Cereb Blood Flow Metab, 2013, 33(8): 1168-1172.
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
1
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
1
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
1
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
2
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
2
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
1
... 据报道,急性大血管闭塞性轻型卒中(acute mild ischemic stroke with large vessel occlusion,LVO-MIS)的神经功能缺损症状表现较轻,但神经功能恶化风险较高[1-2].目前,国内外相关指南[3-4]均推荐对于美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分≥6分的急性大血管闭塞性卒中(acute ischemic stroke with large vessel occlusion,LVO-AIS)行血管内治疗(endovascular therapy,EVT),而对NIHSS<6分(即LVO-MIS)没有明确的指导建议.国外一项多中心回顾性研究[5]显示,对LVO-MIS患者行EVT的良好预后并不优于标准内科治疗,且出血风险更高.个别研究[6-7]报道,对行EVT的LVO-MIS患者进行随访观察后发现,其3个月时的独立生活能力与行标准内科治疗的该类患者的结果相似.也有研究[2,8]显示,行EVT的LVO-MIS患者在出院时、长期随访中均具有较强的独立生活能力.且国内有少量病例报道显示,对LVO-MIS行EVT是安全有效的[9].由于国内关于EVT与标准内科治疗在LVO-MIS早期有效性、安全性方面的研究较少,本研究以LVO-MIS患者为研究对象,针对NIHSS评分变化、早期神经功能恶化(early neurological deterioration,END)、症状性颅内出血(symptomatic intracerebral hemorrhage,sICH)等指标进行回顾性分析,以期为LVO-MIS治疗提供参考. ...
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究的次要结局指标为血管成功再通、END.采用改良脑梗死溶栓分级(modified Thrombolysis in Cerebral Infarction Score,mTICI)评估责任血管的再通情况,其中mTICI 2b~3级定义为血管成功再通[12].将患者入院72 h内NIHSS评分比基线评分增加≥4分[13-14]定义为END. ...
1
... 本研究的次要结局指标为血管成功再通、END.采用改良脑梗死溶栓分级(modified Thrombolysis in Cerebral Infarction Score,mTICI)评估责任血管的再通情况,其中mTICI 2b~3级定义为血管成功再通[12].将患者入院72 h内NIHSS评分比基线评分增加≥4分[13-14]定义为END. ...
1
... 本研究的次要结局指标为血管成功再通、END.采用改良脑梗死溶栓分级(modified Thrombolysis in Cerebral Infarction Score,mTICI)评估责任血管的再通情况,其中mTICI 2b~3级定义为血管成功再通[12].将患者入院72 h内NIHSS评分比基线评分增加≥4分[13-14]定义为END. ...
2
... 本研究的次要结局指标为血管成功再通、END.采用改良脑梗死溶栓分级(modified Thrombolysis in Cerebral Infarction Score,mTICI)评估责任血管的再通情况,其中mTICI 2b~3级定义为血管成功再通[12].将患者入院72 h内NIHSS评分比基线评分增加≥4分[13-14]定义为END. ...
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...
1
... 安全性评价指标为sICH、死亡.参照欧洲协作组急性卒中研究Ⅲ(European Cooperative Acute Stroke Study Ⅲ,ECASS Ⅲ)[15]的试验标准,将术后24 h复查影像存在颅内出血的证据,且颅内出血导致NIHSS评分增加≥4分或导致死亡定义为sICH. ...
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
0
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究发现,与对照组相比,EVT组患者的早期有效率较高、END发生率较低;EVT组患者的血管成功再通率为93.5%,与静脉溶栓相比,EVT成功再通率更高.DA ROS等研究[19]显示,采用EVT治疗LVO-MIS的再通率高于静脉溶栓治疗.在针对LVO-AIS的中国急性大血管闭塞性缺血性卒中直接动脉治疗的疗效评估(Direct Intraarterial Thrombectomy to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals:a Multicenter Randomized Clinical Trial,DIRECT-MT)、急性缺血性卒中血管内治疗关键技术及急救流程改进研究(Endovascular Treatment Key Technique and Emergency Work Flow Improvement of Acute Ischemic Stroke,ANGEL-ACT)等研究[20-22]的结果显示,直接行EVT不劣于桥接治疗.BHATIA等[23]研究显示阿替普酶静脉溶栓在大脑中动脉M1段的再通率为32.3%,在颈内动脉的再通率仅为4.4%;这与本研究结果(46.2%)相比,LVO-MIS静脉溶栓治疗显然是获益的[24-25].本研究中静脉溶栓再通率(46.2%)相对较高,可能与LVO-MIS患者的早期血栓负荷小、血栓通透性高有关[26].静脉溶栓后观察和等待溶栓效果会延长入院到完成穿刺时间、增加sICH和栓子破碎导致的栓塞风险[27].在安全性方面,本研究的2组中各有1例患者发生sICH,且相关研究[11]显示静脉溶栓出血风险低,微小动脉瘤(<10 mm)是溶栓的相对禁忌.在这2例sICH中,1例为合并颅内微小动脉瘤患者(EVT组)静脉溶栓后出血,直接行EVT或可避免静脉溶栓导致动脉瘤破裂出血的风险;另1例为脑梗死出血转化(对照组),且住院期间2组患者均未发生死亡.继而提示,患者在安全性方面的组间无差异. ...
1
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...
1
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...
0
1
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...
1
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...
1
... 本研究的EVT组中有2例LVO-MIS患者未成功再通,其病因均为大动脉粥样硬化性狭窄;针对该种情况,传统的支架取栓联合负压抽吸难以去除狭窄远端血栓,而采用远端取栓支架保护下的球囊血管成形术(balloon angioplasty with the distal protection of stent retriever,BASIS)同时应用GPI则可显著降低传统支架取栓后再闭塞的风险,从而可改善患者的预后[28-30].在本研究超溶栓时间窗的分析中发现EVT可显著降低患者的END,继而提示针对超溶栓时间窗的LVO-MIS患者开展EVT或更有意义[31].既往研究发现,LVO-MIS患者的END与侧支循环衰竭、近端闭塞及血栓长度等高度相关[14,32].因此,结合影像学检查行综合评估以筛选END高危患者进而开展EVT干预可能更有意义. ...



{kind=link}
{kind=link}