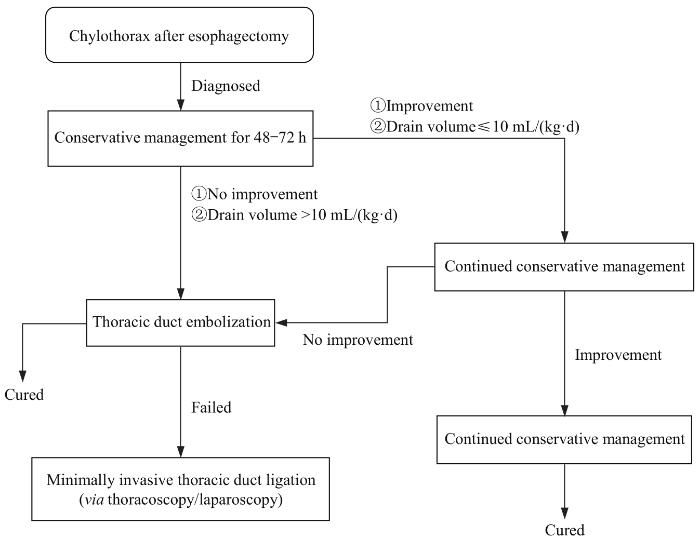
Thoracic duct is the longest lymphatic duct in the human body and plays an important role in maintaining normal metabolism and immune function. Chylothorax is a rare complication after esophageal surgery, which is caused by the injury of the thoracic duct during esophagectomy, resulting in the accumulation of chyle in the pleural cavity. The etiology may be related to anatomical variation, patient's general condition, tumor stage, perioperative intervention and other factors. Preoperative and intraoperative preventive measures can reduce the incidence of chylothorax. Although the incidence rate is low, misdiagnosis or unsuccessful management can increase postoperative complications and lead to serious metabolic disorders and even death. Therefore, early diagnosis and intervention are of paramount importance. Diagnosis should be based on clinical manifestations, supplemented by laboratory and imaging studies. Currently, there is no standard for treatment, which mainly includes conservative treatment, interventional treatment, and surgical treatment. It is necessary to make a comprehensive judgment according to the actual situation and select the appropriate treatment method. In recent years, interventional technology could accurately localize the chylothorax, which is expected to play a more important role in the treatment of chylothorax. This article reviews the latest advances in the etiology, diagnosis, treatment, and prevention of chylothorax after esophagectomy and provides a flow chart of treatment steps to effectively manage this complication.
Keywords:esophageal cancer
;
chylothorax
;
thoracic duct
WANG Xinyu, ZHAO Xiaojing, TANG Jian. Research progress in diagnosis and treatment of chylothorax after esophagectomy. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(2): 244-249 doi:10.3969/j.issn.1674-8115.2023.02.015
ZHANG等[10]的一项meta分析纳入14项研究比较体质量指数(body mass index,BMI)对食管癌术后乳糜胸的影响。结果显示,高BMI的患者术后发生乳糜胸的概率更低(RR=0.98,95%CI 0.96~0.99,P<0.001)。MIAO等[11]的研究也显示术前低BMI(BMI<25 kg/m2)是食管癌术后发生乳糜胸的独立影响因素(HR=9.256,P=0.029)。其中机制尚不明确,可能是由于瘦小的体型胸腔解剖更为清晰,清扫更加彻底,易导致术中胸导管损伤。而脂肪组织可对胸导管有一定的保护作用,从而导致降低乳糜胸发生率。此外,患者若合并基础性疾病,可能会对乳糜胸产生影响。CHENG等[12]比较Child-Pugh A级肝硬化患者与正常患者食管癌术后乳糜胸的发生率,数据显示肝硬化患者术后乳糜胸的发生率显著增加(10% vs 1%,P=0.016),这可能与术中行胸导管结扎及淋巴回流受限有关。
奥曲肽和依替福林对乳糜胸可能具有一定的治疗作用,但现有的证据主要来源于其他病因导致的乳糜漏。奥曲肽是一种长效生长抑素,通过减少内脏血流量降低乳糜液中三酰甘油含量,进而促进瘘口自行愈合的可能,给药2~3 d即可对轻度至中度乳糜胸有效[20]。奥曲肽治疗食管术后的乳糜胸成功率在38%~100%[21]。依替福林是一种α受体激动剂,可引起胸导管平滑肌收缩,进而减缓乳糜液的流速促进瘘口愈合,目前在食管术后相关的乳糜胸应用较少。一项小样本的回顾性研究[22]显示依替福林可以缩短住院天数,但差异尚未达到统计学意义(11.6 d vs 27.8 d,P= 0.078)。因此,依替福林在治疗食管术后的乳糜胸没有显示出显著的疗效,尚无足够的证据推荐常规使用。
胸腔注入粘连剂,如四环素、米诺环素、博来霉素、OK-432、高糖或滑石粉等,促使胸膜粘连,消灭胸膜残腔,以减少乳糜液的渗出[23]。富血小板纤维蛋白凝胶(platelet-rich plasma and fibrin glue,PRFG)是通过提取外周血小板浓缩物,具有抗感染、组织修复、促进创面愈合等作用,近年来在口腔颌面外科、骨科应用较多。PRFG在乳糜胸中的治疗应用目前相关文献较少,已有在肺切除术和心脏手术后成功治疗乳糜胸的报道[24]。ALAMDARI等[25]尝试在胸管中注入PRFG,并与胸导管结扎术对比疗效差异。结果显示,在26例乳糜胸患者中使用PRFG治愈率达100%,高于手术组(76.9%,P= 0.009),且住院时间远低于手术组[(36.04 ± 8.22)d vs (53.50±16.66)d,P<0.001)。作者建议针对所有食管癌术后乳糜胸的患者在一般保守治疗无效后、外科手术干预前尝试使用[25]。目前PRFG治疗乳糜胸的研究多为小样本或病例报道,需大样本的前瞻性、随机对照研究去验证其治疗效果。
The manuscript was drafted by WANG Xinyu and revised by ZHAO Xiaojing and TANG Jian. ZHAO Xiaojing and TANG Jian also participated in the conception of the paper. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
FEI X, WANG X Y, LU Q J, et al. The influence of thoracic duct ligation on long-term survival of patients with esophageal cancer: a propensity score-matched analysis[J]. J Thorac Dis, 2020, 12(10): 5532-5541.
JOHNSON O W, CHICK J F, CHAUHAN N R, et al. The thoracic duct: clinical importance, anatomic variation, imaging, and embolization[J]. Eur Radiol, 2016, 26(8): 2482-2493.
MIRANDA GARCÉS M, MIRAPEIX R, PONS G, et al. A comprehensive review of the natural lymphaticovenous communications and their role in lymphedema surgery[J]. J Surg Oncol, 2016, 113(4): 374-380.
OHKURA Y, UENO M, SHINDOH J, et al. Risk factors for postoperative chylothorax after radical subtotal esophagectomy[J]. Ann Surg Oncol, 2018, 25(9): 2739-2746.
GRONNIER C, TRÉCHOT B, DUHAMEL A, et al. Impact of neoadjuvant chemoradiotherapy on postoperative outcomes after esophageal cancer resection: results of a European multicenter study[J]. Ann Surg, 2014, 260(5): 764-770; discussion 770-771.
YANG H, LIU H, CHEN Y P, et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): a phase Ⅲ multicenter, randomized, open-label clinical trial[J]. J Clin Oncol, 2018, 36(27): 2796-2803.
ZHANG S S, YANG H, LUO K J, et al. The impact of body mass index on complication and survival in resected oesophageal cancer: a clinical-based cohort and meta-analysis[J]. Br J Cancer, 2013, 109(11): 2894-2903.
CHENG C, WEN Y W, TSAI C Y, et al. Impact of Child-Pugh class A liver cirrhosis on perioperative outcomes of patients with oesophageal cancer: a propensity score-matched analysis[J]. Eur J Cardiothorac Surg, 2020: ezaa334.
MALIBARY N, MANFREDELLI S, ALMUTTAWA A, et al. Evaluating the surgeon's experience as a risk factor for post-esophagectomy chylothorax on a four-year cohort[J]. Cureus, 2020, 12(6): e8696.
MATSUTANI T, HIRAKATA A, NOMURA T, et al. Transabdominal approach for chylorrhea after esophagectomy by using fluorescence navigation with indocyanine green[J]. Case Rep Surg, 2014, 2014: 464017.
NIU L L, QIU L, YANG M D, et al. Diagnostic value and influencing factors of chylous test of pleural effusion after thoracic surgery[J]. Chinese Journal of Clinical Thoracic and Cardiovascular Surgery, 2021, 28(9): 1037-1043.
HYUN D, LEE H Y, CHO J H, et al. Pragmatic role of noncontrast magnetic resonance lymphangiography in postoperative chylothorax or cervical chylous leakage as a diagnostic and preprocedural planning tool[J]. Eur Radiol, 2022, 32(4): 2149-2157.
LOW D E, ALDERSON D, CECCONELLO I, et al. International consensus on standardization of data collection for complications associated with esophagectomy: Esophagectomy Complications Consensus Group (ECCG)[J]. Ann Surg, 2015, 262(2): 286-294.
MISTHOS P, KANAKIS M A, LIOULIAS A G. Chylothorax complicating thoracic surgery: conservative or early surgical management?[J]. Updates Surg, 2012, 64(1): 5-11.
ISMAIL N A, GORDON J, DUNNING J. The use of octreotide in the treatment of chylothorax following cardiothoracic surgery[J]. Interact Cardiovasc Thorac Surg, 2015, 20(6): 848-854.
POWER R, SMYTH P, DONLON N E, et al. Management of chyle leaks following esophageal resection: a systematic review[J]. Dis Esophagus, 2021, 34(11): doab012.
OHKURA Y, UENO M, IIZUKA T, et al. Effectiveness of etilefrine regimen for chylothorax after esophagectomy with thoracic duct resection[J]. Esophagus, 2018, 15(1): 33-38.
TASHNIZI M A, MALEKI M H, JAVEDANFAR O, et al. Platelet-rich plasma fibrin glue for treatment of chylothorax following cavopulmonary connections[J]. Eur J Cardiothorac Surg, 2020, 58(6): 1269-1273.
ALAMDARI D H, ASADI M, RAHIM A N, et al. Efficacy and safety of pleurodesis using platelet-rich plasma and fibrin glue in management of postoperative chylothorax after esophagectomy[J]. World J Surg, 2018, 42(4): 1046-1055.
COPE C. Diagnosis and treatment of postoperative chyle leakage via percutaneous transabdominal catheterization of the cisterna chyli: a preliminary study[J]. J Vasc Interv Radiol, 1998, 9(5): 727-734.
CHEN C S, KIM J W, SHIN J H, et al. Lymphatic imaging and intervention for chylothorax following thoracic aortic surgery[J]. Medicine (Baltimore), 2020, 99(34): e21725.
KIM P H, TSAUO J, SHIN J H. Lymphatic interventions for chylothorax: a systematic review and meta-analysis[J]. J Vasc Interv Radiol, 2018, 29(2): 194-202.e4.
MARTHALLER K J, JOHNSON S P, PRIDE R M, et al. Percutaneous embolization of thoracic duct injury post-esophagectomy should be considered initial treatment for chylothorax before proceeding with open re-exploration[J]. Am J Surg, 2015, 209(2): 235-239.
JEON Y J, CHO J H, HYUN D, et al. Management of chyle leakage after general thoracic surgery: impact of thoracic duct embolization[J]. Thorac Cancer, 2021, 12(9): 1382-1386.
NOVELLI P M, CHAN E G, FRAZIER A A, et al. Interventional therapies for thoracic duct injury and intractable chylothorax[J]. J Thorac Imaging, 2019, 34(4): 258-265.
MISHRA P K, SALUJA S S, RAMASWAMY D, et al. Thoracic duct injury following esophagectomy in carcinoma of the esophagus: ligation by the abdominal approach[J]. World J Surg, 2013, 37(1): 141-146.
TANG H X, BAI Y Q, SHEN W L, et al. Anastomosis of the thoracic duct and the azygos vein for the treatment of recurrent chylothoraxes[J]. Eur J Cardiothorac Surg, 2018, 53(5): 1093-1094.
YUAN Y, CHEN L Q, ZHAO Y F. Anastomosis between thoracic duct and azygos vein during esophagectomy: a novel technique with 3-year follow-up[J]. World J Surg, 2016, 40(12): 2984-2987.
SHEN Y X, FENG M X, KHAN M A, et al. A simple method minimizes chylothorax after minimally invasive esophagectomy[J]. J Am Coll Surg, 2014, 218(1): 108-112.
DU Z S, LI X Y, LUO H S, et al. Preoperative administration of olive oil reduces chylothorax after minimally invasive esophagectomy[J]. Ann Thorac Surg, 2019, 107(5): 1540-1543.
VECCHIATO M, MARTINO A, SPONZA M, et al. Thoracic duct identification with indocyanine green fluorescence during minimally invasive esophagectomy with patient in prone position[J]. Dis Esophagus, 2020, 33(12): doaa030.
CRUCITTI P, MANGIAMELI G, PETITTI T, et al. Does prophylactic ligation of the thoracic duct reduce chylothorax rates in patients undergoing oesophagectomy? A systematic review and meta-analysis[J]. Eur J Cardiothorac Surg, 2016, 50(6): 1019-1024.
GUO W, ZHAO Y P, JIANG Y G, et al. Prevention of postoperative chylothorax with thoracic duct ligation during video-assisted thoracoscopic esophagectomy for cancer[J]. Surg Endosc, 2012, 26(5): 1332-1336.
CHEN J Y, LIU Q W, ZHANG S S, et al. Prophylactic thoracic duct ligation is associated with poor prognosis and regional lymph node relapse in esophageal squamous cell carcinoma[J]. J Surg Oncol, 2020, 122(2): 336-343.
BÉDAT B, SCARPA C R, SADOWSKI S M, et al. Acute pancreatitis after thoracic duct ligation for iatrogenic chylothorax. A case report[J]. BMC Surg, 2017, 17(1): 9.
LIN Y D, LI Z H, LI G, et al. Selective en masse ligation of the thoracic duct to prevent chyle leak after esophagectomy[J]. Ann Thorac Surg, 2017, 103(6): 1802-1807.
BROWN S, ABANA C O, HAMMAD H, et al. Low-dose radiation therapy is an effective treatment for refractory postoperative chylous ascites: a case report[J]. Pract Radiat Oncol, 2019, 9(3): 153-157.
... ZHANG等[10]的一项meta分析纳入14项研究比较体质量指数(body mass index,BMI)对食管癌术后乳糜胸的影响.结果显示,高BMI的患者术后发生乳糜胸的概率更低(RR=0.98,95%CI 0.96~0.99,P<0.001).MIAO等[11]的研究也显示术前低BMI(BMI<25 kg/m2)是食管癌术后发生乳糜胸的独立影响因素(HR=9.256,P=0.029).其中机制尚不明确,可能是由于瘦小的体型胸腔解剖更为清晰,清扫更加彻底,易导致术中胸导管损伤.而脂肪组织可对胸导管有一定的保护作用,从而导致降低乳糜胸发生率.此外,患者若合并基础性疾病,可能会对乳糜胸产生影响.CHENG等[12]比较Child-Pugh A级肝硬化患者与正常患者食管癌术后乳糜胸的发生率,数据显示肝硬化患者术后乳糜胸的发生率显著增加(10% vs 1%,P=0.016),这可能与术中行胸导管结扎及淋巴回流受限有关. ...
1
... ZHANG等[10]的一项meta分析纳入14项研究比较体质量指数(body mass index,BMI)对食管癌术后乳糜胸的影响.结果显示,高BMI的患者术后发生乳糜胸的概率更低(RR=0.98,95%CI 0.96~0.99,P<0.001).MIAO等[11]的研究也显示术前低BMI(BMI<25 kg/m2)是食管癌术后发生乳糜胸的独立影响因素(HR=9.256,P=0.029).其中机制尚不明确,可能是由于瘦小的体型胸腔解剖更为清晰,清扫更加彻底,易导致术中胸导管损伤.而脂肪组织可对胸导管有一定的保护作用,从而导致降低乳糜胸发生率.此外,患者若合并基础性疾病,可能会对乳糜胸产生影响.CHENG等[12]比较Child-Pugh A级肝硬化患者与正常患者食管癌术后乳糜胸的发生率,数据显示肝硬化患者术后乳糜胸的发生率显著增加(10% vs 1%,P=0.016),这可能与术中行胸导管结扎及淋巴回流受限有关. ...
1
... ZHANG等[10]的一项meta分析纳入14项研究比较体质量指数(body mass index,BMI)对食管癌术后乳糜胸的影响.结果显示,高BMI的患者术后发生乳糜胸的概率更低(RR=0.98,95%CI 0.96~0.99,P<0.001).MIAO等[11]的研究也显示术前低BMI(BMI<25 kg/m2)是食管癌术后发生乳糜胸的独立影响因素(HR=9.256,P=0.029).其中机制尚不明确,可能是由于瘦小的体型胸腔解剖更为清晰,清扫更加彻底,易导致术中胸导管损伤.而脂肪组织可对胸导管有一定的保护作用,从而导致降低乳糜胸发生率.此外,患者若合并基础性疾病,可能会对乳糜胸产生影响.CHENG等[12]比较Child-Pugh A级肝硬化患者与正常患者食管癌术后乳糜胸的发生率,数据显示肝硬化患者术后乳糜胸的发生率显著增加(10% vs 1%,P=0.016),这可能与术中行胸导管结扎及淋巴回流受限有关. ...
... 奥曲肽和依替福林对乳糜胸可能具有一定的治疗作用,但现有的证据主要来源于其他病因导致的乳糜漏.奥曲肽是一种长效生长抑素,通过减少内脏血流量降低乳糜液中三酰甘油含量,进而促进瘘口自行愈合的可能,给药2~3 d即可对轻度至中度乳糜胸有效[20].奥曲肽治疗食管术后的乳糜胸成功率在38%~100%[21].依替福林是一种α受体激动剂,可引起胸导管平滑肌收缩,进而减缓乳糜液的流速促进瘘口愈合,目前在食管术后相关的乳糜胸应用较少.一项小样本的回顾性研究[22]显示依替福林可以缩短住院天数,但差异尚未达到统计学意义(11.6 d vs 27.8 d,P= 0.078).因此,依替福林在治疗食管术后的乳糜胸没有显示出显著的疗效,尚无足够的证据推荐常规使用. ...
1
... 奥曲肽和依替福林对乳糜胸可能具有一定的治疗作用,但现有的证据主要来源于其他病因导致的乳糜漏.奥曲肽是一种长效生长抑素,通过减少内脏血流量降低乳糜液中三酰甘油含量,进而促进瘘口自行愈合的可能,给药2~3 d即可对轻度至中度乳糜胸有效[20].奥曲肽治疗食管术后的乳糜胸成功率在38%~100%[21].依替福林是一种α受体激动剂,可引起胸导管平滑肌收缩,进而减缓乳糜液的流速促进瘘口愈合,目前在食管术后相关的乳糜胸应用较少.一项小样本的回顾性研究[22]显示依替福林可以缩短住院天数,但差异尚未达到统计学意义(11.6 d vs 27.8 d,P= 0.078).因此,依替福林在治疗食管术后的乳糜胸没有显示出显著的疗效,尚无足够的证据推荐常规使用. ...
1
... 奥曲肽和依替福林对乳糜胸可能具有一定的治疗作用,但现有的证据主要来源于其他病因导致的乳糜漏.奥曲肽是一种长效生长抑素,通过减少内脏血流量降低乳糜液中三酰甘油含量,进而促进瘘口自行愈合的可能,给药2~3 d即可对轻度至中度乳糜胸有效[20].奥曲肽治疗食管术后的乳糜胸成功率在38%~100%[21].依替福林是一种α受体激动剂,可引起胸导管平滑肌收缩,进而减缓乳糜液的流速促进瘘口愈合,目前在食管术后相关的乳糜胸应用较少.一项小样本的回顾性研究[22]显示依替福林可以缩短住院天数,但差异尚未达到统计学意义(11.6 d vs 27.8 d,P= 0.078).因此,依替福林在治疗食管术后的乳糜胸没有显示出显著的疗效,尚无足够的证据推荐常规使用. ...
1
... 胸腔注入粘连剂,如四环素、米诺环素、博来霉素、OK-432、高糖或滑石粉等,促使胸膜粘连,消灭胸膜残腔,以减少乳糜液的渗出[23].富血小板纤维蛋白凝胶(platelet-rich plasma and fibrin glue,PRFG)是通过提取外周血小板浓缩物,具有抗感染、组织修复、促进创面愈合等作用,近年来在口腔颌面外科、骨科应用较多.PRFG在乳糜胸中的治疗应用目前相关文献较少,已有在肺切除术和心脏手术后成功治疗乳糜胸的报道[24].ALAMDARI等[25]尝试在胸管中注入PRFG,并与胸导管结扎术对比疗效差异.结果显示,在26例乳糜胸患者中使用PRFG治愈率达100%,高于手术组(76.9%,P= 0.009),且住院时间远低于手术组[(36.04 ± 8.22)d vs (53.50±16.66)d,P<0.001).作者建议针对所有食管癌术后乳糜胸的患者在一般保守治疗无效后、外科手术干预前尝试使用[25].目前PRFG治疗乳糜胸的研究多为小样本或病例报道,需大样本的前瞻性、随机对照研究去验证其治疗效果. ...
1
... 胸腔注入粘连剂,如四环素、米诺环素、博来霉素、OK-432、高糖或滑石粉等,促使胸膜粘连,消灭胸膜残腔,以减少乳糜液的渗出[23].富血小板纤维蛋白凝胶(platelet-rich plasma and fibrin glue,PRFG)是通过提取外周血小板浓缩物,具有抗感染、组织修复、促进创面愈合等作用,近年来在口腔颌面外科、骨科应用较多.PRFG在乳糜胸中的治疗应用目前相关文献较少,已有在肺切除术和心脏手术后成功治疗乳糜胸的报道[24].ALAMDARI等[25]尝试在胸管中注入PRFG,并与胸导管结扎术对比疗效差异.结果显示,在26例乳糜胸患者中使用PRFG治愈率达100%,高于手术组(76.9%,P= 0.009),且住院时间远低于手术组[(36.04 ± 8.22)d vs (53.50±16.66)d,P<0.001).作者建议针对所有食管癌术后乳糜胸的患者在一般保守治疗无效后、外科手术干预前尝试使用[25].目前PRFG治疗乳糜胸的研究多为小样本或病例报道,需大样本的前瞻性、随机对照研究去验证其治疗效果. ...
2
... 胸腔注入粘连剂,如四环素、米诺环素、博来霉素、OK-432、高糖或滑石粉等,促使胸膜粘连,消灭胸膜残腔,以减少乳糜液的渗出[23].富血小板纤维蛋白凝胶(platelet-rich plasma and fibrin glue,PRFG)是通过提取外周血小板浓缩物,具有抗感染、组织修复、促进创面愈合等作用,近年来在口腔颌面外科、骨科应用较多.PRFG在乳糜胸中的治疗应用目前相关文献较少,已有在肺切除术和心脏手术后成功治疗乳糜胸的报道[24].ALAMDARI等[25]尝试在胸管中注入PRFG,并与胸导管结扎术对比疗效差异.结果显示,在26例乳糜胸患者中使用PRFG治愈率达100%,高于手术组(76.9%,P= 0.009),且住院时间远低于手术组[(36.04 ± 8.22)d vs (53.50±16.66)d,P<0.001).作者建议针对所有食管癌术后乳糜胸的患者在一般保守治疗无效后、外科手术干预前尝试使用[25].目前PRFG治疗乳糜胸的研究多为小样本或病例报道,需大样本的前瞻性、随机对照研究去验证其治疗效果. ...



{kind=link}
{kind=link}