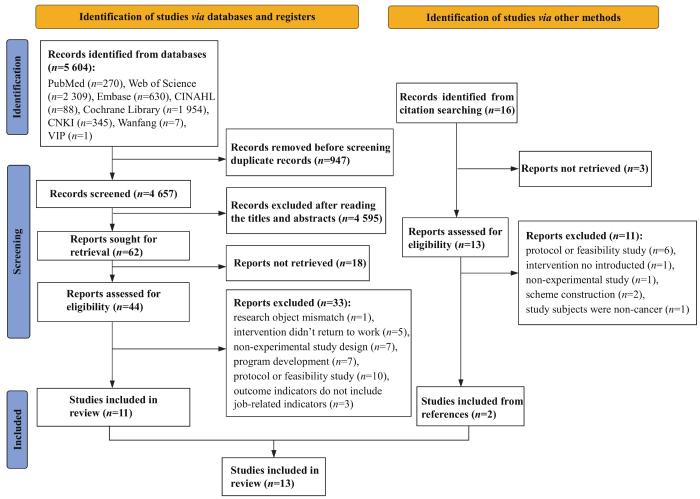
Objective ·To systematically evaluate the application of return-to-work intervention programs to young and middle-aged cancer survivors and its effectiveness in improving work-related outcomes in cancer survivors. Methods ·An initial literature search of eight electronic databases, including PubMed, Cochrane Library, Embase, CNKI and Wanfang was conducted with a time frame from inception to Aug 2nd, 2022 to collect randomized controlled trials (RCTs) and quasi-experimental studies of return-to-work interventions on work-related outcomes among cancer survivors. Two researchers independently conducted literature screening, data extraction, and methodological quality evaluation using the JBI (Joanna Briggs Institute) Methodology Quality Evaluation Tool. Results ·A total of 13 original studies were included, involving 11 return-to-work intervention programs, containing 2 045 cancer survivors. The results of the systematic evaluation showed that 10 of the intervention programs were multidisciplinary, with intervention modules on disease/mental health education, group discussions, physical rehabilitation, work capacity exercises, multidisciplinary team meetings and counselling. Among them, three interventions also included employers in the support program. The duration of the interventions ranged from 7 d to one year. Eight of the included interventions took return-to-work rates as a primary outcome, but only three reported that the difference was statistically significant, two of which were quasi-experimental studies without control group. Besides, no clear positive effects were found on work-related outcome such as length of return-to-work, change of work status, work ability, and work meaning. Conclusion ·The content, format, intensity and frequency of return-to-work intervention programs for cancer survivors vary widely, and the effects of interventions on work-related outcomes are still unclear. Researchers should further explore the mechanisms that influence cancer survivors′ return-to-work, and develop multidisciplinary intervention programs based on this to effectively help young and middle-aged cancer survivors return-to-work and society. In addition, due to the limitations of study quality and intervention program heterogeneity, more high-quality experimental studies are needed to further validate the above findings.
Keywords:cancer survivor
;
young and middle-aged
;
return-to-work
;
program evaluation
;
systematic review
ZHANG Yuanyuan, WU Anqi, WU Jie, ZHU Yaqi, LI Mengyao, YAN Dexiu, ZHANG Yaqing, HOU Lili. Interventions to enhance return-to-work among young and middle-aged cancer survivors: a systematic review. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(3): 333-341 doi:10.3969/j.issn.1674-8115.2023.03.009
如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架。而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与。干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等。FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定。4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次。
Tab 2
表2
表2重返工作干预方案的相关特征
Tab 2 Characteristics of return-to-work interventions
physical exercise (twice a day, 100 h during 4 weeks),
patient education (each day),
group discussion (each day).
The focus of patient education and group discussion session:
cancer treatment and side effect, physical activity, nutrition, economy and work situation, factors of return-to-work, partnership and sexuality, and psychological reaction
A
Multiprofessional team
4 weeks
Rehabilitation center
Outpatient rehabilitation program: delivered at an academic cancer hospital, lasted for seven weeks. The focus were the same
The first two sessions covered the topics related to cancer treatment, side effects, partnership and sexuality, economy and work situation, nutrition, physical exercise and coping strategies
individual meetings of psychosocial work-related support (30 min each);
work related support: fatigue, pain and lack of support from family and friends (support Ⅰ); lack of support in work environment and neuropsychological problems (support Ⅱ); a combination of factors (support Ⅲ)
B
Support Ⅰ: oncological gastrointestinal nurse;
support Ⅱ: oncological occupational physicians (OOP);
support Ⅲ: multidisciplinary team (including at least a oncology nurse, a physician and a OOP)
Maximum of 9 months
Hospital
Standard psychological care provided by oncological nurse
a, b
Note: A represents group intervention, B represents individualized intervention. a represents return-to-work rate, b represents time to return, c represents role function, d represents work ability, e represents meaning of work, f represents return-to-work self-efficacy, g represents work limitation, h represents work status, i represents weekly working hour reduction. ①P<0.001, ②P=0.005, ③P=0.0025, ④P=0.033, ⑤P<0.01, ⑥P=0.03.
This manuscript was designed by ZHANG Yuanyuan, ZHANG Yaqing, and HOU Lili. Information retrieval, data selection, data extraction and synthesis were conducted by ZHANG Yuanyuan, WU Anqi, WU Jie, ZHU Yaqi, LI Mengyao and YAN Dexiu. The manuscript was drafted by ZHANG Yuanyuan and WU Anqi, and revised and proofed by ZHANG Yaqing and HOU Lili. All authors has read the last version of manuscript and approved the submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
FENG R M, ZONG Y N, CAO S M, et al. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics?[J]. Cancer Commun, 2019, 39(1): 22.
MILLER K D, FIDLER-BENAOUDIA M, KEEGAN T H, et al. Cancer statistics for adolescents and young adults, 2020[J]. CA Cancer J Clin, 2020, 70(6): 443-459.
RINGASH J, BERNSTEIN L J, DEVINS G, et al. Head and neck cancer survivorship: learning the needs, meeting the needs[J]. Semin Radiat Oncol, 2018, 28(1): 64-74.
CHECK D K, HUTCHESON K A, POISSON L M, et al. Factors associated with employment discontinuation among older and working age survivors of oropharyngeal cancer[J]. Head Neck, 2019, 41(11): 3948-3959.
BJÖRNEKLETT H G, ROSENBLAD A, LINDEMALM C, et al. A randomized controlled trial of support group intervention after breast cancer treatment: results on sick leave, health care utilization and health economy[J]. Acta Oncol, 2013, 52(1): 38-47.
FAUSER D, WIENERT J, BEINERT T, et al. Work-related medical rehabilitation in patients with cancer-postrehabilitation results from a cluster-randomized multicenter trial[J]. Cancer, 2019, 125(15): 2666-2674.
LEENSEN M C J, GROENEVELD I F, VAN DER HEIDE I, et al. Return to work of cancer patients after a multidisciplinary intervention including occupational counselling and physical exercise in cancer patients: a prospective study in the Netherlands[J]. BMJ Open, 2017, 7(6): e014746.
OLDERVOLL L M, THORSEN L, KAASA S, et al. Inpatient versus outpatient rehabilitation after breast and gynecological cancers: a comparative study[J]. Int J Phys Med Rehabil, 2013, 2(2): 1-7.
MOURGUES C, GERBAUD L, LEGER S, et al. Positive and cost-effectiveness effect of spa therapy on the resumption of occupational and non-occupational activities in women in breast cancer remission: a French multicentre randomised controlled trial[J]. Eur J Oncol Nurs, 2014, 18(5): 505-511.
RUSBRIDGE S L, WALMSLEY N C, GRIFFITHS S B, et al. Predicting outcomes of vocational rehabilitation in patients with brain tumours[J]. Psycho-oncology, 2013, 22(8): 1907-1911.
STAPELFELDT C M, MOMSEN A M H, JENSEN A B, et al. Municipal return to work management in cancer survivors: a controlled intervention study[J]. Acta Oncol, 2021, 60(3): 370-378.
TAMMINGA S J, VERBEEK J H A M, BOS M M E M, et al. Effectiveness of a hospital-based work support intervention for female cancer patients: a multi-centre randomised controlled trial[J]. PLoS One, 2013, 8(5): e63271.
TAMMINGA S J, VERBEEK J M, BOS M M, et al. Two-year follow-up of a multi-centre randomized controlled trial to study effectiveness of a hospital-based work support intervention for cancer patients[J]. J Occup Rehabil, 2019, 29(4): 701-710.
THIJS K M, DE BOER A G E M, VREUGDENHIL G, et al. Rehabilitation using high-intensity physical training and long-term return-to-work in cancer survivors[J]. J Occup Rehabil, 2012, 22(2): 220-229.
THORSEN L, DAHL A A, NYSTAD R, et al. Baseline characteristics in female cancer patients with unimproved work status after an outpatient rehabilitation program and health changes during the intervention[J]. Springerplus, 2016, 5(1): 1009.
ZAMAN A M, TYTGAT K J, KLINKENBIJL J G, et al. Effectiveness of a tailored work-related support intervention for patients diagnosed with gastrointestinal cancer: a multicenter randomized controlled trial[J]. J Occup Rehabil, 2021, 31(2): 323-338.
TAMMINGA S J, HOVING J L, FRINGS-DRESEN M H W, et al. Cancer@Work: a nurse-led, stepped-care, e-health intervention to enhance the return to work of patients with cancer: study protocol for a randomized controlled trial[J]. Trials, 2016, 17(1): 453.
GUO Y J, TANG J, LI J M, et al. Exploration of interventions to enhance return-to-work for cancer patients: a scoping review[J]. Clin Rehabil, 2021, 35(12): 1674-1693.
LIANG L L, ZHANG Y, SHI Y, et al. Research progress on application of timing theory in disease nursing[J]. Chinese Nursing Research, 2016, 30(5): 524-525.
CHEN S C, HUANG B S, HUNG T M, et al. Impact of physical and psychosocial dysfunction on return to work in survivors of oral cavity cancer[J]. Psycho-oncology, 2019, 28(9): 1910-1917.
RANGABASHYAM M, KOH S Q, SULTANA R, et al. Factors associated with returning to work in head and neck cancer survivors in Singapore: a preliminary exploratory mixed-methods approach study[J]. Head Neck, 2021, 43(5): 1451-1464.
KJÆR T, BØJE C R, OLSEN M H, et al. Affiliation to the work market after curative treatment of head-and-neck cancer: a population-based study from the DAHANCA database[J]. Acta Oncol, 2013, 52(2): 430-439.
BAXI S S, SALZ T, XIAO H, et al. Employment and return to work following chemoradiation in patient with HPV-related oropharyngeal cancer[J]. Cancers Head Neck, 2016, 1: 4.
AGARWAL J, KRISHNATRY R, CHATURVEDI P, et al. Survey of return to work of head and neck cancer survivors: a report from a tertiary cancer center in India[J]. Head Neck, 2017, 39(5): 893-899.
GREIDANUS M A, DE BOER A G E M, DE RIJK A E, et al. Perceived employer-related barriers and facilitators for work participation of cancer survivors: a systematic review of employers′ and survivors′ perspectives[J]. Psycho-oncology, 2018, 27(3): 725-733.
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... Characteristics of return-to-work interventionsTab 2
Study
Intervention group
Control group
Outcome
Content
Type
Who
How long
Where
BJÖRNEKLETT et al, 2013[8]
Information-based support program: ...
5
... et al, 2019[9-10] ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...
... 如表2所示,纳入的13篇研究中仅有1篇研究报告了理论框架,即STAPELFELDT等[15]指出应用“癌症和工作模型(the cancer and work model)”[21]作为构建重返工作方案的理论框架.而从干预类别上看,10种干预方案[8-17,19-20]均为多学科团队介入的干预,干预内容包含疾病/心理健康教育、小组讨论、物理康复、工作能力锻炼、多学科团队会议和咨询等模块,且肿瘤科护士、肿瘤科医师、物理康复治疗师、职业康复治疗师、心理治疗师、艺术治疗师等多角色参与.干预频次从每日1次到间隔数月1次,干预持续时间从7 d到1年不等.FAUSER等[9-10]的方案中仅对各模块需要的最少时长进行了规定.4项干预方案[14-17,20]根据患者的个体化需求来确定模块的内容和频次. ...



{kind=link}
{kind=link}