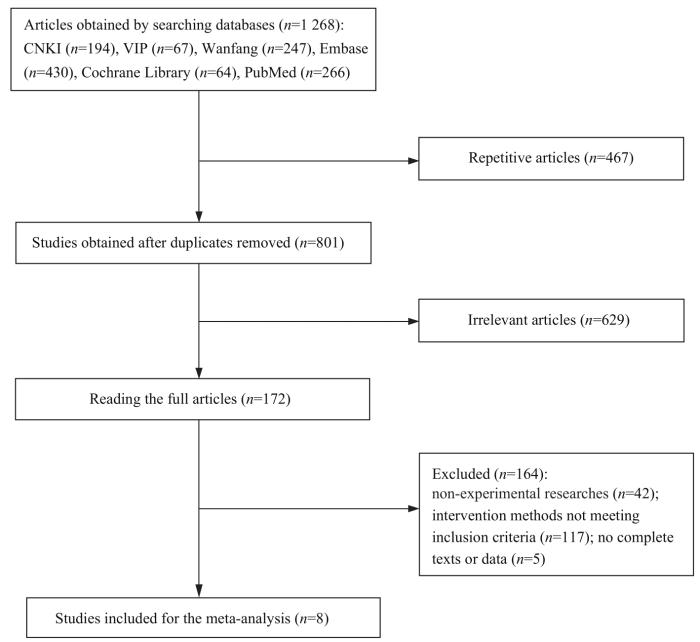
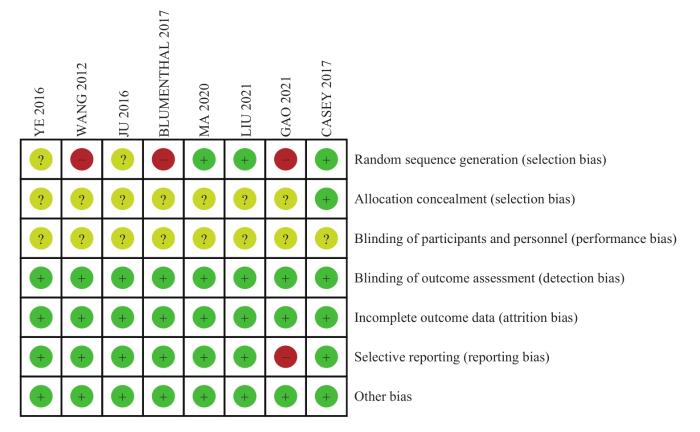
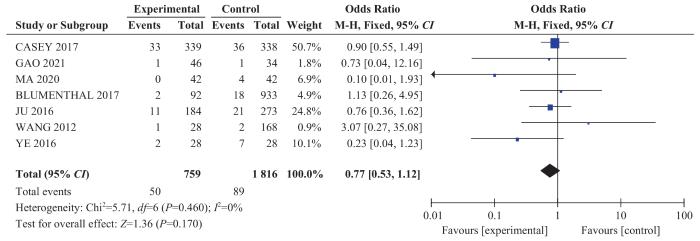
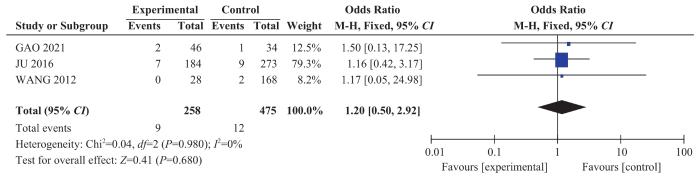
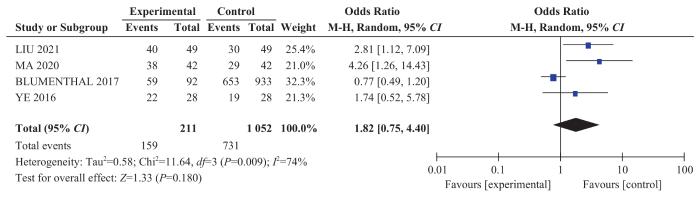
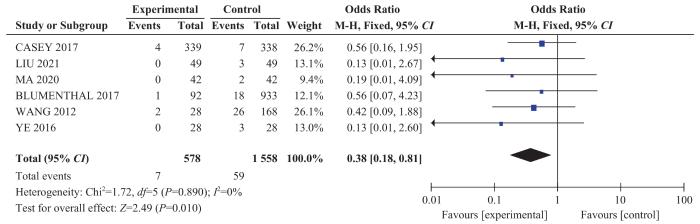
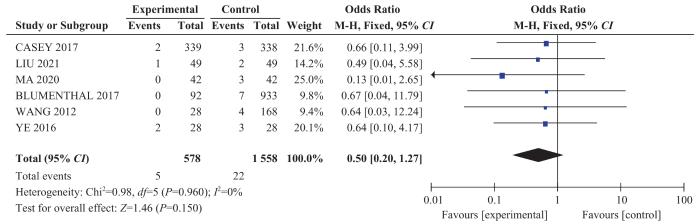
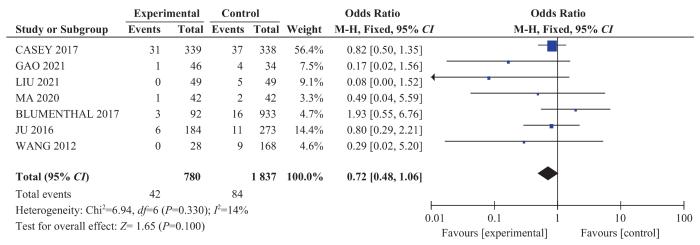
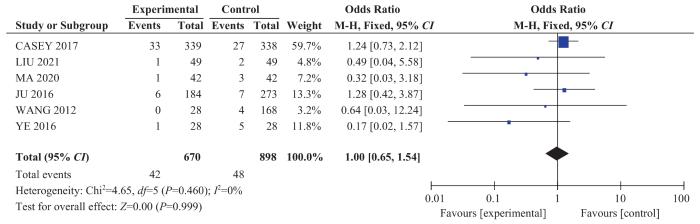
Objective ·To evaluate the effects of levothyroxine (L-T4) dose adjustment according to the level of thyroid stimulating hormone (TSH) on maternal and infant outcomes in the pregnant women with hypothyroidism by meta-analysis. Methods ·China National Knowledge Infrastructure (CNKI), China Science and Technology Journal Database (VIP), Wanfang Data Knowledge Service Platform, PubMed, Cochrane Library and Embase were retrieved to collect all the controlled studies on the treatment of pregnant women with hypothyroidism by adjusting the dose of L-T4 according to TSH level from the establishment of the databases to April 9, 2022. The references were also traced. Literature screening, data extraction, and quality evaluation were performed independently by two researchers. Cochrane evaluation was used to evaluate the quality of the included literature. Outcome indicators included gestational hypertension, gestational diabetes, postpartum hemorrhage, delivery mode, preterm birth, fetal death, neonatal asphyxia, and low birth weight infants. RevMan 5.3 was used for meta-analysis. Result ·A total of 1 268 articles were retrieved from 6 databases, and 8 were included in the study, including 4 Chinese articles and 4 English articles. The overall risk of study bias was at a moderate level. Compared with the control group, the OR of gestational diabetes risk was 0.61 (95%CI 0.44‒0.86, P=0.004) and the OR of fetal death risk was 0.38 (95%CI 0.18‒0.81, P=0.010) in the experimental group with L-T4 dose adjusted according to the TSH level of the pregnant women with hypothyroidism, which were both statistically significant. However, the treatment method of adjusting L-T4 dose did not affect the risks of vaginal delivery [OR=1.82 (95%CI 0.75‒4.40, P=0.180)], gestational hypertension [OR=0.77 (95%CI 0.53‒1.12, P=0.170)], postpartum hemorrhage [OR=1.20 (95%CI 0.50‒2.92, P=0.680)], preterm birth [OR=0.72 (95%CI 0.48‒1.06, P=0.100)], low birth weight infants [OR=1.00 (95%CI 0.65‒1.54, P=0.999)], or neonatal asphyxia [OR=0.50 (95%CI 0.20‒1.27, P=0.150)] significantly. Conclusion ·Adjusting the L-T4 therapeutic dose according to the TSH level may help reduce the risks of gestational diabetes and fetal death in the pregnant women with hypothyroidism.
CHEN Hui, ZHU Weiyi, YAO Yijin. A meta-analysis of the effects of levothyroxine dose adjustment on maternal and infant outcomes in pregnant women with hypothyroidism. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(7): 906-915 doi:10.3969/j.issn.1674-8115.2023.07.013
检索中国知网(CNKI)、维普中文科技期刊数据库(维普,VIP)、万方数据知识服务平台(万方,Wanfang)、Embase、Cochrane Library、PubMed数据库,检索语种限制为中文和英文,检索时间为建库至2022年4月9日。通过PubMed数据库MeSH词表和Embase数据库Emtree词表检索主题词,根据检索结果调整并确定检索关键词。中文检索策略:① “孕妇”OR“妊娠”OR“怀孕”OR“孕期”OR“产妇”。② “甲状腺功能减退”OR“甲减”。③ “左旋甲状腺素”OR“优甲乐”OR“激素”OR“L-T4”。④ “剂量”。⑤ “①AND②AND③AND④”。英文检索策略:①“pregnant” OR “pregnancy” OR “expectant mother”OR “maternity”OR “maternal” OR “gestation” OR “gravidity” OR “parturient” OR “puerpera” OR “fetation”。②“hypothyroidism” OR “hypothyroid” OR “hypothyrea” OR “thyroid hypofunction”。③“levothyroxine” OR “L-thyroine” OR “L-T4” OR “levoid” OR “euthyrox” OR “hormone”。④“dosage” OR “dose”。⑤ “①AND②AND③AND ④”。
采用Revman 5.3软件进行meta分析。连续性资料采用加权均数差(weighted mean difference,WMD)和95%CI;定性资料采用优势比(OR)和95%CI。采用χ2检验评估各研究间的异质性,检验水准α=0.1。若I2≤50%,P≥0.01,提示各研究间具有同质性,采用固定效应模型;若I2>50%,P<0.01,提示各研究间具有异质性,采用随机效应模型,并进行敏感性分析或亚组分析寻找异质性来源。
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions
The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked once a month and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of
The study was designed by YAO Yijin. The data were collected and processed by CHEN Hui and ZHU Weiyi. The manuscript was drafted by CHEN Hui. The statistics of data and the manuscript revision were completed by ZHU Weiyi. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
DONG A C, STAGNARO-GREEN A. Differences in diagnostic criteria mask the true prevalence of thyroid disease in pregnancy: a systematic review and meta-analysis[J]. Thyroid, 2019, 29(2): 278-289.
The Consortium on Thyroid and Pregnancy-Study Group on Preterm Birth. Association of thyroid function test abnormalities and thyroid autoimmunity with preterm birth: a systematic review and meta-analysis[J]. JAMA, 2019, 322(7): 632-641.
MARAKA S, OSPINA N M S, O′KEEFFE D T, et al. Subclinical hypothyroidism in pregnancy: a systematic review and meta-analysis[J]. Thyroid, 2016, 26(4): 580-590.
SULLIVAN S D, DOWNS E, POPOVENIUC G, et al. Randomized trial comparing two algorithms for levothyroxine dose adjustment in pregnant women with primary hypothyroidism[J]. J Clin Endocrinol Metab, 2017, 102(9): 3499-3507.
GAO J B. Observation of the effect of subclinical hypothyroidism during pregnancy and thyroid hormone intervention on pregnancy outcome[J]. Medicine and Pharmacy of Yunnan, 2021, 42(4):345-347.
YE X M,CHEN Y Y. Dose adjustment of levothyroxine tablets for 28 cases of pregnancy complicated with hypothyroidism[J]. Chinese Journal of Woman and Child Health Research, 2016, 27(S1): 425.
MA Y H. Analysis of therapeutic effect of different doses of levothyroxine sodium tablets on pregnant women with hypothyroidism [J]. The Journal of Medical Theory and Practice, 2020, 33(18): 3060-3062.
LIU L J. Dose adjustment analysis of levothyroxine tablets for pregnant women with hypothyroidism[J]. Strait Pharmaceutical Journal, 2021, 33(7): 181-182.
CASEY B M, THOM E A, PEACEMAN A M, et al. Treatment of subclinical hypothyroidism or hypothyroxinemia in pregnancy[J]. N Engl J Med, 2017, 376(9): 815-825.
BLUMENTHAL N J, EASTMAN C J. Beneficial effects on pregnancy outcomes of thyroid hormone replacement for subclinical hypothyroidism[J]. J Thyroid Res, 2017, 2017: 4601365.
WANG S, TENG W P, LI J X, et al. Effects of maternal subclinical hypothyroidism on obstetrical outcomes during early pregnancy[J]. J Endocrinol Invest, 2012, 35(3): 322-325.
JU R, LIN L, LONG Y, et al. Clinical efficacy of therapeutic intervention for subclinical hypothyroidism during pregnancy[J]. Genet Mol Res, 2016, 15(4). DOI: 10.4238/gmr15049019.
LI C L, HUANG H, LI Q H. Relationship of subclinical hypothyroidism with gestational diabetes mellitus during early pregnancy[J]. Chinese Journal of Endocrinology and Metabolism, 2014, 30(9): 747-748.
DERAKHSHAN A, KOREVAAR T I M, TAYLOR P N, et al. The association of maternal thyroid autoimmunity during pregnancy with child IQ[J]. J Clin Endocrinol Metab, 2018, 103(10): 3729-3736.
LIU J D, WANG R, HE J X. Relationship between hypothyroidism and spontaneous abortion in early pregnancy[J]. Journal of Clinical Research, 2022, 39(2): 232-235.
ALEXANDER E K, PEARCE E N, BRENT G A, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum[J]. Thyroid, 2017, 27(3): 315-389.
DING Z, LIU Y D, MARAKA S, et al. Pregnancy and neonatal outcomes with levothyroxine treatment in women with subclinical hypothyroidism based on new diagnostic criteria: a systematic review and meta-analysis[J]. Front Endocrinol (Lausanne), 2021, 12: 797423.
JIAO X F, ZHANG M, CHEN J J, et al. The impact of levothyroxine therapy on the pregnancy, neonatal and childhood outcomes of subclinical hypothyroidism during pregnancy: an updated systematic review, meta-analysis and trial sequential analysis[J]. Front Endocrinol (Lausanne), 2022, 13: 964084.
SHAN Z Y, TENG W P. Guideline on diagnosis and management of thyroid diseases during pregnancy and postpartum (2nd edition): an essential introduction[J]. Chinese Journal of Endocrinology and Metabolism, 2019, 35(8): 632-635.
Writing Committee for Guidelines for Prevention and Management of Thyroid Diseases During Pregnancy and Perinatal Period, Chinese Society of Endocrinology, Chinese Medical Association, Women′s Health Care Branch of Chinese Preventive Medicine Association. Guidelines for prevention and management of thyroid diseases during pregnancy and perinatal period[J]. Chinese Journal of Endocrinology and Metabolism, 2022, 38(7): 539-551.
HUBALEWSKA-DYDEJCZYK A, TROFIMIUK-MÜLDNER M, RUCHALA M, et al. Thyroid diseases in pregnancy: guidelines of the Polish Society of Endocrinology[J]. Endokrynol Pol, 2021, 72(5): 425-488.
WANG W J. Effects of levothyroxine sodium tablets on thyroid function, adverse reactions and pregnancy outcomes in patients with hypothyroidism during pregnancy[J]. Electronic Journal of Practical Gynecological Endocrinology, 2022, 9(12): 27-30.
HAN Y, WANG J, WANG X Y, et al. Relationship between subclinical hypothyroidism in pregnancy and hypertensive disorder of pregnancy: a systematic review and meta-analysis[J]. Front Endocrinol (Lausanne), 2022, 13: 823710.
SONG Q Q, LI Z H, GUO S Q, et al. Effect of disease of pregnant women with gestational diabetes mellitus and subclinical hypothyroidism on their bone mineral density, and levels of osteocalcin and 25-hydroxyvitamin D[J]. Chinese Journal of Family Planning, 2020, 28(1): 56-59.
VELASCO I, VILA L, GOYA M, et al. Executive summary of the SEEN (Sociedad Española de Endocrinología y Nutrición [Spanish Society of Endocrinology and Nutrition])-SEGO (Sociedad Española deGinecología y Obstetricia [Spanish Society of Gynaecology and Obstetrics]) consensus document on the management of thyroid dysfunction during pregnancy[J]. Endocrinol Diabetes Nutr (Engl Ed), 2023, 70(Suppl 1): 38-50.
Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted
Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet
GH, PH, GDM, PD
YE[9]
2016
China
28
28
22-34
22-34
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions ...
Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted
Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet
GH, PH, GDM, PD
YE[9]
2016
China
28
28
22-34
22-34
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions ...
Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted
Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet
GH, PH, GDM, PD
YE[9]
2016
China
28
28
22-34
22-34
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions ...
Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted
Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet
GH, PH, GDM, PD
YE[9]
2016
China
28
28
22-34
22-34
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions ...
The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked once a month and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of ...
The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked once a month and the L-T4 dose was adjusted
The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of ...




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}