[1]
CHAKRAVARTY E F, BUSH T M, MANZI S, et al. Prevalence of adult systemic lupus erythematosus in California and Pennsylvania in 2000: estimates obtained using hospitalization data[J]. Arthritis Rheum, 2007, 56(6): 2092-2094.
[本文引用: 1]
[2]
PONS-ESTEL G J, ALARCÓN G S, SCOFIELD L, et al. Understanding the epidemiology and progression of systemic lupus erythematosus[J]. Semin Arthritis Rheum, 2010, 39(4): 257-268.
[3]
IZMIRLY P M, PARTON H, WANG L, et al. Prevalence of systemic lupus erythematosus in the United States: estimates from a meta-analysis of the centers for disease control and prevention national lupus registries[J]. Arthritis Rheumatol, 2021, 73(6): 991-996.
[4]
STOJAN G, PETRI M. Epidemiology of systemic lupus erythematosus: an update[J]. Curr Opin Rheumatol, 2018, 30(2): 144-150.
[本文引用: 1]
[5]
中华医学会血液学分会红细胞疾病(贫血)学组. 获得性纯红细胞再生障碍诊断与治疗中国专家共识(2020年版)[J]. 中华血液学杂志, 2020, 41(3): 177-184.
[本文引用: 3]
Red Blood Cell Disease (Anemia) Group, Chinese Society of Hematology, Chinese Medical Association. Chinese expert consensus on the diagnosis and treatment of acquired pure red cell aplasia (2020)[J]. Chinese Journal of Hematology, 2020, 41(3): 177-184.
[本文引用: 3]
[6]
张丽, 邹尧, 陈玉梅, 等. 儿童系统性红斑狼疮相关纯红细胞再生障碍性贫血1例报告并文献复习[J]. 中国实用儿科杂志, 2005, 20(7): 436-438.
[本文引用: 2]
ZHANG L, ZOU Y, CHEN Y M, et al. Pure red cell aplasia as presentation of systemic lupus erythematosus in children[J]. Chinese Journal of Practical Pediatrics, 2005, 20(7): 436-438.
[本文引用: 2]
[7]
张国材. 继发于系统性红斑性狼疮的纯红细胞性再生障碍性贫血1例报告[J]. 新医学, 1991, 22(4): 187.
[本文引用: 1]
ZHANG G C. A case report of pure red blood cell aplastic anemia secondary to systemic lupus erythematosus[J]. Journal of New Medicine, 1991, 22(4): 187.
[本文引用: 1]
[8]
谢其冰, 杨南萍, 罗泽玲. 系统性红斑狼疮伴纯红细胞再生障碍性贫血2例[J]. 实用医学杂志, 2002, 18(8): 865.
[本文引用: 1]
XIE Q B, YANG N P, LUO Z L, et al. Two cases of systemic lupus erythematosus with pure red blood cell aplastic anemia[J]. The Journal of Practical Medicine, 2002, 18(8): 865.
[本文引用: 1]
[9]
陈楠楠, 黄世林, 向阳, 等. 系统性红斑狼疮并发纯红细胞再生障碍性贫血[J]. 临床皮肤科杂志, 2006, 35(8): 536.
[本文引用: 1]
CHEN N N, HUANG S L, XIANG Y, et al. Systemic lupus erythematosus complicated with pure red blood cell aplastic anemia[J]. Journal of Clinical Dermatology, 2006, 35(8): 536.
[本文引用: 1]
[10]
刘国强. 系统性红斑狼疮并发纯红细胞再生障碍性贫血2例[J]. 中国实用内科杂志, 2005, 25(10): 958.
[本文引用: 1]
LIU G Q. Two cases of systemic lupus erythematosus complicated with pure red blood cell aplastic anemia[J]. Chinese Journal of Practical Internal Medicine, 2005, 25(10): 958.
[本文引用: 1]
[11]
黄仁魏, 夏忠军, 吴祥元, 等. 以纯红细胞再生障碍性贫血为首发表现的系统性红斑狼疮1例[J]. 中国实用内科杂志, 1998, 18(9): 551.
[本文引用: 1]
HUANG R W, XIA Z J, WU X Y, et al. A case of systemic lupus erythematosus with pure red blood cell aplastic anemia as the initial manifestation[J]. Chinese Journal of Practical Internal Medicine, 1998, 18(9): 551.
[本文引用: 1]
[12]
刘维凤, 吴恩亮. 以纯红细胞再生障碍性贫血为首发症状的系统性红斑狼疮1例[J]. 滨州医学院学报, 1999, 22(6): 620.
[本文引用: 1]
LIU W F, WU E L. A case of systemic lupus erythematosus with pure red blood cell aplastic anemia as the initial symptom[J]. Journal of Binzhou Medical University, 1999, 22(6): 620.
[本文引用: 1]
[13]
刘艳, 高华, 任虹蓉, 等. 重症系统性红斑狼疮合并纯红细胞再生障碍性贫血1例[J]. 武警后勤学院学报(医学版), 2017, 26(9): 823-824.
[本文引用: 1]
LIU Y, GAO H, REN H R, et al. A case of severe systemic lupus erythematosus complicated with pure red blood cell aplastic anemia[J]. Journal of Logistics University of PAP (Medical Sciences), 2017, 26(9): 823-824.
[本文引用: 1]
[14]
倪勋, 魏锦, 罗文丰. 系统性红斑狼疮继发纯红细胞再生障碍一例[J]. 华西医学, 2011, 26(8): 1211-1212.
[本文引用: 1]
NI X, WEI J, LUO W F. A case of secondary pure red blood cell regeneration disorder in systemic lupus erythematosus[J]. West China Medical Journal, 2011, 26(8): 1211-1212.
[本文引用: 1]
[15]
MITSUNAKA H, TOKUDA M, TAKAHARA J, et al. A case of systemic lupus erythematosus with pure red cell aplasia possibly caused by persistent infection of human parvovirus B19[J]. Nihon Rinsho Meneki Gakkai Kaishi, 1998, 21(5): 220-225.
[本文引用: 1]
[16]
IWADATE H, KOBAYASHI H, SHIO K, et al. A case of systemic lupus erythematosus complicated by pure red cell aplasia and idiopathic portal hypertension after thymectomy[J]. Mod Rheumatol, 2006, 16(2): 109-112.
[本文引用: 1]
[17]
HABIB G S, SALIBA W R, FROOM P. Pure red cell aplasia and lupus[J]. Semin Arthritis Rheum, 2002, 31(4): 279-283.
[本文引用: 1]
[18]
LINARDAKI G D, BOKI K A, FERTAKIS A, et al. Pure red cell aplasia as presentation of systemic lupus erythematosus: antibodies to erythropoietin[J]. Scand J Rheumatol, 1999, 28(3): 189-191.
[本文引用: 1]
[19]
KOYAMA R V, SILVA L F, HENRIQUES V B, et al. Pure red cell aplasia associated with systemic lupus erythematosus[J]. Acta Reumatol Port, 2014, 39(3): 265-268.
[本文引用: 1]
[20]
CHOI B G, YOO W H. Successful treatment of pure red cell aplasia with plasmapheresis in a patient with systemic lupus erythematosus[J]. Yonsei Med J, 2002, 43(2): 274-278.
[本文引用: 1]
[21]
DUCHMANN R, SCHWARTING A, PORALLA T, et al. Thymoma and pure red cell aplasia in a patient with systemic lupus erythematosus[J]. Scand J Rheumatol, 1995, 24(4): 251-254.
[本文引用: 1]
[22]
FRANCIS D A. Pure red-cell aplasia: association with systemic lupus erythematosus and primary autoimmune hypothyroidism[J]. Br Med J (Clin Res Ed), 1982, 284(6309): 85.
[本文引用: 1]
[23]
OKADA H, SUZUKI H, UCHIDA H, et al. Acquired idiopathic pure red cell aplasia in a hemodialyzed patient with inactive systemic lupus erythematosus[J]. Intern Med, 1994, 33(8): 492-495.
[本文引用: 1]
[24]
MAVRAGANI C P, VLACHAKI E, VOULGARELIS M. Pure red cell aplasia in a Sjögren's syndrome/lupus erythematosus overlap patient[J]. Am J Hematol, 2003, 72(4): 259-262.
[本文引用: 1]
[25]
KIELY P D, MCGUCKIN C P, COLLINS D A, et al. Erythrocyte aplasia and systemic lupus erythematosus[J]. Lupus, 1995, 4(5): 407-411.
[本文引用: 1]
[26]
ATZENI F, SARZI-PUTTINI P, CAPSONI F, et al. Successful treatment of pure red cell aplasia in systemic lupus erythematosus with cyclosporin A[J]. Clin Exp Rheumatol, 2003, 21(6): 759-762.
[本文引用: 1]
[27]
DUARTE-SALAZAR C, CAZARÍN-BARRIENTOS J, GOYCOCHEA-ROBLES M V, et al. Successful treatment of pure red cell aplasia associated with systemic lupus erythematosus with cyclosporin A[J]. Rheumatology (Oxford), 2000, 39(10): 1155-1157.
[本文引用: 1]
[28]
CHAN A Y K, LI E K, TAM L S, et al. Successful treatment of pure red cell aplasia associated with systemic lupus erythematosus with oral danazol and steroid[J]. Rheumatol Int, 2005, 25(5): 388-390.
[本文引用: 1]
[29]
IDEGUCHI H, OHNO S, ISHIGATSUBO Y. A case of pure red cell aplasia and systemic lupus erythematosus caused by human parvovirus B19 infection[J]. Rheumatol Int, 2007, 27(4): 411-414.
[本文引用: 1]
[30]
SUZUKI T, SAITO S, HIRABAYASHI Y, et al. Human parvovirus B19 infection during the inactive stage of systemic lupus erythematosus[J]. Intern Med, 2003, 42(6): 538-540.
[本文引用: 1]
[31]
GUPTA R K, EZEONYEJI A N, THOMAS A S, et al. A case of pure red cell aplasia and immune thrombocytopenia complicating systemic lupus erythematosus: response to rituximab and cyclophosphamide[J]. Lupus, 2011, 20(14): 1547-1550.
[本文引用: 1]
[32]
FRANZÉN P, FRIMAN C, PETTERSSON T, et al. Combined pure red cell aplasia and primary autoimmune hypothyroidism in systemic lupus erythematosus[J]. Arthritis Rheum, 1987, 30(7): 839-840.
[本文引用: 1]
[33]
HECK L W, ALARCÓN G S, BALL G V, et al. Pure red cell aplasia and protein-losing enteropathy in a patient with systemic lupus erythematosus[J]. Arthritis Rheum, 1985, 28(9): 1059-1061.
[本文引用: 1]
[34]
HARA A, WADA T, KITAJIMA S, et al. Combined pure red cell aplasia and autoimmune hemolytic anemia in systemic lupus erythematosus with anti-erythropoietin autoantibodies[J]. Am J Hematol, 2008, 83(9): 750-752.
[本文引用: 1]
[35]
MARMONT A M, BACIGALUPO A, GUALANDI F, et al. Systemic lupus erythematosus complicated with thymoma and pure red cell aplasia (PCRA). CR of both complications following thymectomy and allogeneic haematopoietic SCT (HSCT), but persistence of antinuclear antibodies (ANA)[J]. Bone Marrow Transplant, 2014, 49(7): 982-983.
[本文引用: 1]
[36]
MEYER R J, HOFFMAN R, ZANJANI E D. Autoimmune hemolytic anemia and periodic pure red cell aplasia in systemic lupus erythematosus[J]. Am J Med, 1978, 65(2): 342-345.
[本文引用: 1]
[37]
FALLAHI S, AKBARIAN M, DABIRI S. Pure red cell aplasia as a presenting feature in systemic lupus erythematosus and association with thymoma, hypothyroidism and hypoparathyroidism: a case report and literature review[J]. Iran J Allergy Asthma Immunol, 2014, 13(2): 138-143.
[本文引用: 1]
[38]
ARCASOY M O, CHAO N J. T-cell-mediated pure red-cell aplasia in systemic lupus erythematosus: response to cyclosporin A and mycophenolate mofetil[J]. Am J Hematol, 2005, 78(2): 161-163.
[本文引用: 1]
[39]
MOLLAEIAN A, HAAS C. A tale of autoimmunity: thymoma, thymectomy, and systemic lupus erythematosus[J]. Clin Rheumatol, 2020, 39(7): 2227-2234.
[本文引用: 1]
[40]
BISWAL N, NARAYANAN P, CHETAN G. Cyclosporine A responsive pure red cell aplasia in a child with systemic lupus erythematosus[J]. Indian J Hematol Blood Transfus, 2007, 23(3/4): 107-108.
[本文引用: 1]
[41]
NAKAMURA H, OKADA A, KAWAKAMI A, et al. Isoniazid-triggered pure red cell aplasia in systemic lupus erythematosus complicated with myasthenia gravis[J]. Rheumatol Int, 2010, 30(12): 1643-1645.
[本文引用: 1]
[42]
ILAN Y, NAPARSTEK Y. Pure red cell aplasia associated with systemic lupus erythematosus: remission after a single course of intravenous immunoglobulin[J]. Acta Haematol, 1993, 89(3): 152-154.
[本文引用: 1]
[43]
TAKIGAWA M, HAYAKAWA M. Thymoma with systemic lupus erythematosus, red blood cell aplasia, and herpesvirus infection[J]. Arch Dermatol, 1974, 110(1): 99-102.
[本文引用: 1]
[44]
HARADA N, NAGASAWA K, OKAMURA T, et al. A case of systemic lypus erythematosus with autoimmune hemolytic anemia amd with a history of pure red cell aplasia[J]. Jpn J Clin Immunol, 1990, 13(3): 286-291.
[本文引用: 1]
[45]
ATSUMI T, SAGAWA A, KATSUMATA K, et al. A case of systemic lupus erythematosus with pure red cell aplasia responded to steroid pulse therapy[J]. Jpn J Clin Immunol, 1991, 14(6): 639-645.
[本文引用: 1]
[46]
JAREK M J, ENZENAUER R J, JUDSON P H. Pure red cell aplasia in systemic lupus erythematosus[J]. J Clin Rheumatol, 1996, 2(1): 44-49.
[本文引用: 1]
[47]
MINAMI R, IZUTSU K, MIYAMURA T, et al. A case of systemic lupus erythematosus accompanied with pure red cell aplasia[J]. Nihon Rinsho Meneki Gakkai Kaishi, 2006, 29(3): 148-153.
[本文引用: 1]
[48]
MURAYAMA J, ASANUMA Y, TSUDA T, et al. Appearance of central nervous system lupus during corticosteroid therapy and warfarinization in a patient with pure red cell aplasia and antiphospholipid syndrome[J]. Nihon Rinsho Meneki Gakkai Kaishi, 2006, 29(1): 43-47.
[本文引用: 1]
[49]
SAEED M, SHARIF F, IJAZ M, et al. A case of systemic lupus erythematosus presenting as pure red cell aplasia[J]. Int J Hematol Oncol Stem Cell Res, 2021, 15(2): 135-138.
[本文引用: 1]
[50]
TOMAC-STOJMENOVIĆ M, HADŽISEJDIĆ I, VALKOVIĆ T, et al. Pure red blood cell aplasia in systemic lupus erythematosus: a case report[J]. Reumatizam, 2017, 64(1): 26-29.
[本文引用: 1]
[51]
杜安琇, 叶凤英, 高雅慧. Azathioprine引起的单纯红血球再生不良[J]. 台湾医学, 2006, 10(1): 42-48.
[本文引用: 1]
DU A X, YE F Y, GAO Y H. Azathioprine-induced pure red blood cell aplasia[J]. Formosan Journal of Medicine, 2006, 10(1): 42-48.
[本文引用: 1]
[52]
JIMENO SAINZ A, BLÁZQUEZ ENCINAR J C, CONESA V. Pure red aplasia as the first manifestation of systemic lupus erythematosus[J]. Am J Med, 2001, 111(1): 78-79.
[本文引用: 2]
[53]
CHOI Y, JO J C, JEON H J, et al. Trend and treatment patterns of aplastic anemia in Korea, pure red cell aplasia and myelodysplastic syndrome in Korea: a nation-wide analysis[J]. Int J Hematol, 2017, 106(4): 500-507.
[本文引用: 1]
1
... 系统性红斑狼疮(systemic lupus erythematosus,SLE)是一种系统性自身免疫病,以全身多系统多脏器受累、反复的复发与缓解、体内存在大量自身抗体为主要临床特点,如不及时治疗,会造成受累脏器不可逆损害.很多SLE患者的整个病程中都贯穿血液系统异常,三系[白细胞(white blood cell,WBC)、血红蛋白(hemoglobin,Hb)和血小板(blood platelet,PLT)]均可受到影响.贫血是SLE最常见的血液学异常,累及超过半数患者[1 -4 ] .但是,SLE合并纯红细胞再生障碍性贫血(pure red cell aplasia,PRCA)却较罕见,尤其是以PRCA作为首发症状的SLE则更为少见.PRCA是以正细胞正色素性贫血、网织红细胞(reticulocyte,Ret)减少和骨髓中红系前体细胞显著减少或缺如为特征的一种罕见的骨髓单纯红系造血障碍综合征,其粒细胞系和巨核细胞系均未明显累及.PRCA患者通常表现为严重的贫血和非常低的Ret计数[5 ] .为了增强临床医师对SLE合并PRCA这类疾病的系统认识,现对上海交通大学医学院附属第一人民医院收治的1例SLE合并PRCA的病例进行报道,并检索1974—2021年文献报道的SLE合并PRCA患者的病例资料,对其进行汇总(共1+51例)和特征分析. ...
1
... 系统性红斑狼疮(systemic lupus erythematosus,SLE)是一种系统性自身免疫病,以全身多系统多脏器受累、反复的复发与缓解、体内存在大量自身抗体为主要临床特点,如不及时治疗,会造成受累脏器不可逆损害.很多SLE患者的整个病程中都贯穿血液系统异常,三系[白细胞(white blood cell,WBC)、血红蛋白(hemoglobin,Hb)和血小板(blood platelet,PLT)]均可受到影响.贫血是SLE最常见的血液学异常,累及超过半数患者[1 -4 ] .但是,SLE合并纯红细胞再生障碍性贫血(pure red cell aplasia,PRCA)却较罕见,尤其是以PRCA作为首发症状的SLE则更为少见.PRCA是以正细胞正色素性贫血、网织红细胞(reticulocyte,Ret)减少和骨髓中红系前体细胞显著减少或缺如为特征的一种罕见的骨髓单纯红系造血障碍综合征,其粒细胞系和巨核细胞系均未明显累及.PRCA患者通常表现为严重的贫血和非常低的Ret计数[5 ] .为了增强临床医师对SLE合并PRCA这类疾病的系统认识,现对上海交通大学医学院附属第一人民医院收治的1例SLE合并PRCA的病例进行报道,并检索1974—2021年文献报道的SLE合并PRCA患者的病例资料,对其进行汇总(共1+51例)和特征分析. ...
3
... 系统性红斑狼疮(systemic lupus erythematosus,SLE)是一种系统性自身免疫病,以全身多系统多脏器受累、反复的复发与缓解、体内存在大量自身抗体为主要临床特点,如不及时治疗,会造成受累脏器不可逆损害.很多SLE患者的整个病程中都贯穿血液系统异常,三系[白细胞(white blood cell,WBC)、血红蛋白(hemoglobin,Hb)和血小板(blood platelet,PLT)]均可受到影响.贫血是SLE最常见的血液学异常,累及超过半数患者[1 -4 ] .但是,SLE合并纯红细胞再生障碍性贫血(pure red cell aplasia,PRCA)却较罕见,尤其是以PRCA作为首发症状的SLE则更为少见.PRCA是以正细胞正色素性贫血、网织红细胞(reticulocyte,Ret)减少和骨髓中红系前体细胞显著减少或缺如为特征的一种罕见的骨髓单纯红系造血障碍综合征,其粒细胞系和巨核细胞系均未明显累及.PRCA患者通常表现为严重的贫血和非常低的Ret计数[5 ] .为了增强临床医师对SLE合并PRCA这类疾病的系统认识,现对上海交通大学医学院附属第一人民医院收治的1例SLE合并PRCA的病例进行报道,并检索1974—2021年文献报道的SLE合并PRCA患者的病例资料,对其进行汇总(共1+51例)和特征分析. ...
... 获得性PRCA主要是由于药物、病毒、抗体或者免疫细胞等攻击红系祖细胞、红细胞生成素或其受体等,抑制红系细胞增殖和分化成熟,从而导致发病;该病多为免疫性,可继发于不同疾病,如SLE、类风湿关节炎、炎症性肠病等[5 ] .获得性PRCA具有多病因性和异质性的特点,患者常无特异性体征,合并SLE者的临床表现多以乏力、关节痛、皮疹为首发表现.实验室检查结果中均以免疫指标异常为主:ANA阳性、抗dsDNA抗体阳性、尿蛋白阳性和低补体水平的人数比例均较高,平均Hb浓度处于重度贫血水平,Ret百分比明显减少.这可能由于外周血液循环中红细胞寿命一般为120 d,每日红细胞丢失速率仅约为1/120,足以让机体有时间代偿以适应慢性缺氧环境,故对于SLE合并PRCA患者易忽视其贫血的治疗.只有处于重度贫血导致严重缺氧时,机体失去代偿,出现明显贫血表现,才会触发患者的就医需求.根据本研究文献统计,52例报道的病例中有6例合并AIHA,8例合并胸腺瘤,5例合并甲状腺功能减退,3例合并重症肌无力.如本文中PRCA、AIHA、甲状腺功能减退相关的SLE的病例鲜有报道. ...
... PRCA的主要治疗目标是恢复红细胞生成,从而减少输血,避免输血相关的问题.免疫源性SLE合并PRCA的发病机制为免疫抑制治疗提供了理论依据,其临床治疗策略和预后分别与基础疾病和病程相关.因此,除了必要的输血支持治疗之外,应尽早对此类患者开始免疫抑制治疗.文献报道中的治疗方案通常侧重于序贯使用各种免疫抑制治疗,直至病情缓解后逐渐减少用药.52例患者中,98.08%均接受糖皮质激素治疗,最大剂量为甲强龙500 mg/d,其次依次为输血治疗、环孢素A、环磷酰胺、高剂量静脉注射免疫球蛋白等.其中环孢素A目前被认为是获得性PRCA的一线治疗用药,有效率为65%~87%,推荐剂量为3~5 mg/(kg·d)[5 ] .但是由于环孢素A具有肾毒性,用药过程中应注意监测血药浓度和肾功能.本例患者应用环孢素A联合糖皮质激素治疗3周后疗效明显,Hb较前增加30 g/L以上,Ret明显升高,后期随访中亦维持正常水平,但尚缺乏完全停药后复查骨髓象的评估反馈.汇总的文献报道中,仅2例应用利妥昔单克隆抗体治疗,其中1例疗效满意;1例治疗无反应后改糖皮质激素联合环孢素A和吗替麦考酚酯治疗,遂病情好转.随着更多SLE发病机制的关键通路被揭示,多种靶向治疗(如生物制剂、小分子制剂、T细胞免疫疗法等)被开发和应用.这些靶向治疗是否能成为SLE合并PRCA患者的选择,其诱导缓解持续时间和维持治疗时间该如何确定,有赖于进一步的临床研究. ...
3
... 系统性红斑狼疮(systemic lupus erythematosus,SLE)是一种系统性自身免疫病,以全身多系统多脏器受累、反复的复发与缓解、体内存在大量自身抗体为主要临床特点,如不及时治疗,会造成受累脏器不可逆损害.很多SLE患者的整个病程中都贯穿血液系统异常,三系[白细胞(white blood cell,WBC)、血红蛋白(hemoglobin,Hb)和血小板(blood platelet,PLT)]均可受到影响.贫血是SLE最常见的血液学异常,累及超过半数患者[1 -4 ] .但是,SLE合并纯红细胞再生障碍性贫血(pure red cell aplasia,PRCA)却较罕见,尤其是以PRCA作为首发症状的SLE则更为少见.PRCA是以正细胞正色素性贫血、网织红细胞(reticulocyte,Ret)减少和骨髓中红系前体细胞显著减少或缺如为特征的一种罕见的骨髓单纯红系造血障碍综合征,其粒细胞系和巨核细胞系均未明显累及.PRCA患者通常表现为严重的贫血和非常低的Ret计数[5 ] .为了增强临床医师对SLE合并PRCA这类疾病的系统认识,现对上海交通大学医学院附属第一人民医院收治的1例SLE合并PRCA的病例进行报道,并检索1974—2021年文献报道的SLE合并PRCA患者的病例资料,对其进行汇总(共1+51例)和特征分析. ...
... 获得性PRCA主要是由于药物、病毒、抗体或者免疫细胞等攻击红系祖细胞、红细胞生成素或其受体等,抑制红系细胞增殖和分化成熟,从而导致发病;该病多为免疫性,可继发于不同疾病,如SLE、类风湿关节炎、炎症性肠病等[5 ] .获得性PRCA具有多病因性和异质性的特点,患者常无特异性体征,合并SLE者的临床表现多以乏力、关节痛、皮疹为首发表现.实验室检查结果中均以免疫指标异常为主:ANA阳性、抗dsDNA抗体阳性、尿蛋白阳性和低补体水平的人数比例均较高,平均Hb浓度处于重度贫血水平,Ret百分比明显减少.这可能由于外周血液循环中红细胞寿命一般为120 d,每日红细胞丢失速率仅约为1/120,足以让机体有时间代偿以适应慢性缺氧环境,故对于SLE合并PRCA患者易忽视其贫血的治疗.只有处于重度贫血导致严重缺氧时,机体失去代偿,出现明显贫血表现,才会触发患者的就医需求.根据本研究文献统计,52例报道的病例中有6例合并AIHA,8例合并胸腺瘤,5例合并甲状腺功能减退,3例合并重症肌无力.如本文中PRCA、AIHA、甲状腺功能减退相关的SLE的病例鲜有报道. ...
... PRCA的主要治疗目标是恢复红细胞生成,从而减少输血,避免输血相关的问题.免疫源性SLE合并PRCA的发病机制为免疫抑制治疗提供了理论依据,其临床治疗策略和预后分别与基础疾病和病程相关.因此,除了必要的输血支持治疗之外,应尽早对此类患者开始免疫抑制治疗.文献报道中的治疗方案通常侧重于序贯使用各种免疫抑制治疗,直至病情缓解后逐渐减少用药.52例患者中,98.08%均接受糖皮质激素治疗,最大剂量为甲强龙500 mg/d,其次依次为输血治疗、环孢素A、环磷酰胺、高剂量静脉注射免疫球蛋白等.其中环孢素A目前被认为是获得性PRCA的一线治疗用药,有效率为65%~87%,推荐剂量为3~5 mg/(kg·d)[5 ] .但是由于环孢素A具有肾毒性,用药过程中应注意监测血药浓度和肾功能.本例患者应用环孢素A联合糖皮质激素治疗3周后疗效明显,Hb较前增加30 g/L以上,Ret明显升高,后期随访中亦维持正常水平,但尚缺乏完全停药后复查骨髓象的评估反馈.汇总的文献报道中,仅2例应用利妥昔单克隆抗体治疗,其中1例疗效满意;1例治疗无反应后改糖皮质激素联合环孢素A和吗替麦考酚酯治疗,遂病情好转.随着更多SLE发病机制的关键通路被揭示,多种靶向治疗(如生物制剂、小分子制剂、T细胞免疫疗法等)被开发和应用.这些靶向治疗是否能成为SLE合并PRCA患者的选择,其诱导缓解持续时间和维持治疗时间该如何确定,有赖于进一步的临床研究. ...
2
... 以“系统性红斑狼疮”“纯红细胞再生障碍性贫血”“病例”为检索词,检索万方数据、中国知网、维普数据库从建库至2021年报道的相关文献.以“systemic lupus erythematosus”“SLE”“pure red cell aplastic anemia”“PRCA”“case report”为检索词,检索PubMed数据库从建库至2021年报道的相关文献.通过阅读文题、摘要及全文,排除资料报道不完整的病例,最终纳入文献47篇,包含51例(国内13例,国外38例)病例(表1 )[6 -52 ] 以及本报道国内1例,一共52例SLE合并PRCA患者的资料,均无重复病例. ...
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
2
... 以“系统性红斑狼疮”“纯红细胞再生障碍性贫血”“病例”为检索词,检索万方数据、中国知网、维普数据库从建库至2021年报道的相关文献.以“systemic lupus erythematosus”“SLE”“pure red cell aplastic anemia”“PRCA”“case report”为检索词,检索PubMed数据库从建库至2021年报道的相关文献.通过阅读文题、摘要及全文,排除资料报道不完整的病例,最终纳入文献47篇,包含51例(国内13例,国外38例)病例(表1 )[6 -52 ] 以及本报道国内1例,一共52例SLE合并PRCA患者的资料,均无重复病例. ...
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
2
... 以“系统性红斑狼疮”“纯红细胞再生障碍性贫血”“病例”为检索词,检索万方数据、中国知网、维普数据库从建库至2021年报道的相关文献.以“systemic lupus erythematosus”“SLE”“pure red cell aplastic anemia”“PRCA”“case report”为检索词,检索PubMed数据库从建库至2021年报道的相关文献.通过阅读文题、摘要及全文,排除资料报道不完整的病例,最终纳入文献47篇,包含51例(国内13例,国外38例)病例(表1 )[6 -52 ] 以及本报道国内1例,一共52例SLE合并PRCA患者的资料,均无重复病例. ...
... Data of the 51 cases
Tab 1 First author Published year Origin of the case Case sample/n Gender Age/year Reference ZHANG L 2005 China 1 F 6 [6 ] ZHANG G C 1991 China 1 M 44 [7 ] XIE Q B 2002 China 2 M/F 54/56 [8 ] CHEN N N 2006 China 1 F 26 [9 ] LIU G Q 2005 China 2 F/F 41/31 [10 ] HUANG R W 1998 China 1 F 43 [11 ] LIU W F 1999 China 1 F 21 [12 ] LIU Y 2017 China 1 M 19 [13 ] NI X 2011 China 1 F 37 [14 ] MITSUNAKA H 1998 Japan 1 F 68 [15 ] IWADATE H 2006 Japan 1 F 43 [16 ] HABIB G S 2002 Iseral 1 F 31 [17 ] LINARDAKI G D 1999 Greece 2 F/F 21/28 [18 ] KOYAMA R V 2014 Brazil 1 F 52 [19 ] CHOI B G 2002 Korea 1 F 31 [20 ] DUCHMANN R 1995 Germany 1 F 63 [21 ] FRANCIS D A 1982 UK 1 F 64 [22 ] OKADA H 1994 Japan 1 M 43 [23 ] MAVRAGANI C P 2003 Greece 1 F 38 [24 ] KIELY P D 1995 India 2 F/F 22/33 [25 ] ATZENI F 2003 Italy 1 F 50 [26 ] DUARTE-SALAZAR C 2000 Mexico 1 F 21 [27 ] CHAN A Y K 2005 Hongkong, China 1 F 59 [28 ] IDEGUCHI H 2007 Japan 1 F 82 [29 ] SUZUKI T 2003 Japan 1 F 54 [30 ] GUPTA R K 2011 Vietnam 1 F 23 [31 ] FRANZÉN P 1987 Finland 1 F 24 [32 ] HECK L W 1985 USA 1 F 17 [33 ] HARA A 2008 Japan 1 F 42 [34 ] MARMONT A M 2014 Italy 1 F 45 [35 ] MEYER R J 1978 China 1 F 56 [36 ] FALLAHI S 2014 Iran 1 F 54 [37 ] ARCASOY M O 2005 USA 1 F 34 [38 ] MOLLAEIAN A 2020 African 1 M 65 [39 ] BISWAL N 2007 India 1 F 9 [40 ] NAKAMURA H 2010 Japan 1 F 47 [41 ] ILAN Y 1993 Iseral 1 F 22 [42 ] TAKIGAWA M 1974 Japan 1 F 44 [43 ] HARADA N 1990 Japan 1 F 27 [44 ] ATSUMI T 1991 Japan 1 M 21 [45 ] JAREK M J 1996 USA 1 F 69 [46 ] MINAMI R 2006 Japan 1 F 33 [47 ] MURAYAMA J 2006 Japan 1 F 48 [48 ] SAEED M 2021 Pakistan 1 F 27 [49 ] TOMAC-STOJMENOVIĆ M 2017 Croatia 1 F 35 [50 ] DU A X 2006 Taiwan, China 1 F 24 [51 ] JIMENO S A 2001 Spain 1 F 19 [52 ]
Note:
1
... 获得性PRCA极为少见,其患病率尚不明确.韩国一项研究[53 ] 发现PRCA的粗患病率为5.28例/100万人,然而目前缺乏跨人群的流行病学数据.本文汇总的52例患者中,亚洲人居多,以女性为主,其中育龄期女性占比最大,这与SLE的流行病学特点相类似.患者诊断为SLE时的中位年龄(31.5岁)早于诊断为PRCA时的中位年龄(36.0岁),先诊断为SLE的人数比例最高.并且先诊断为SLE后诊断为PRCA的诊断间隔时间(约6年)明显长于先诊断为PRCA的间隔时间(约3年).这可能是由于现代临床疾病检出技术的进步,可以早期诊断出SLE.此外,贫血是SLE最常见的血液学异常,可贯穿整个病程.若未与临床信息全面结合分析,忽视必要的血液学鉴别手段,极易漏诊PRCA或者误诊为单纯的血液系统疾病.同理,对于初诊在血液科就诊的年轻女性PRCA患者,若伴有皮肤、关节表现时,也应积极完善相关免疫抗体检查,避免漏诊SLE. ...


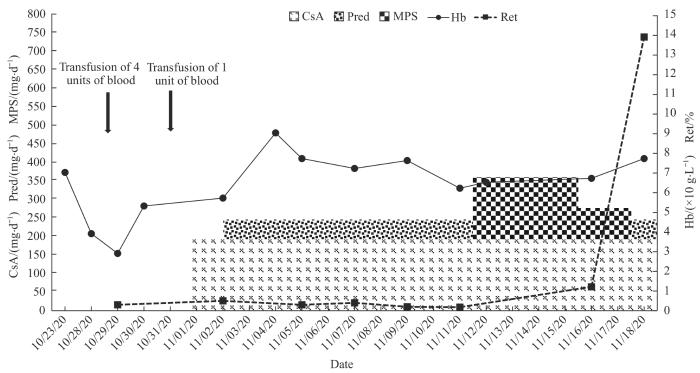
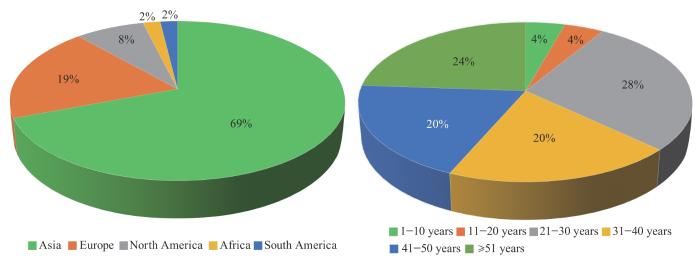

{kind=link}
{kind=link}
{kind=link}
{kind=link}