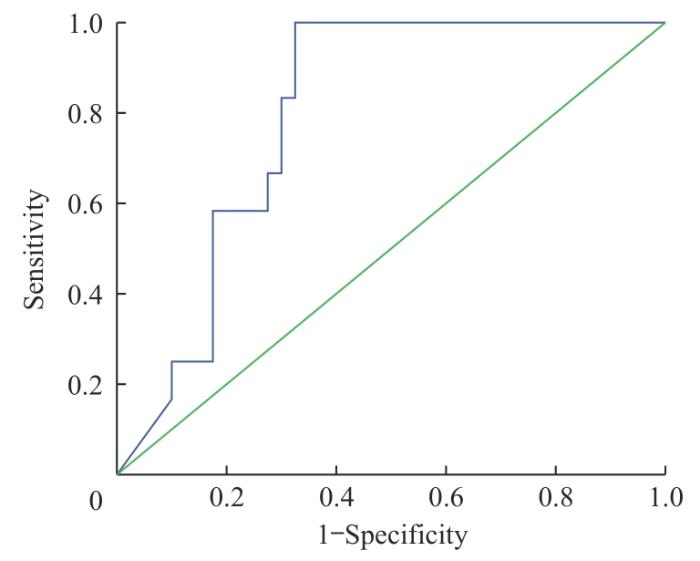
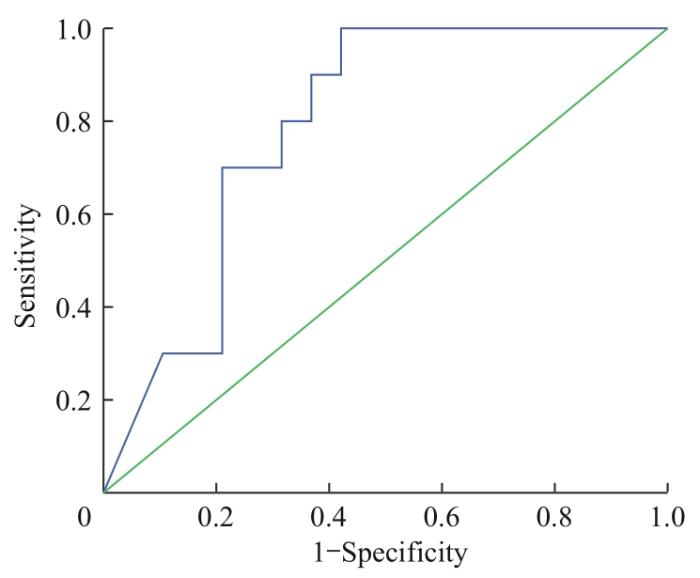
目的·分析重度烧伤患者早期血清肝素结合蛋白(heparin-binding protein,HBP)表达水平,探讨其对患者预后及脓毒症发生的预警价值。方法·回顾性分析上海交通大学医学院附属瑞金医院灼伤整形科2021年1月—2023年5月收治的52例重度烧伤患者的临床资料。收集患者性别、年龄、烧伤总面积、身体质量指数(body mass index,BMI)、是否行气管插管或气管切开等一般资料。收集患者入院48 h内的HBP、血清降钙素原(procalcitonin,PCT)、血清C反应蛋白(C reactive protein,CRP)水平和白细胞计数,以及入院48 h内急性生理与慢性健康评估Ⅱ(acute physiology and chronic health evaluation Ⅱ,APACHE Ⅱ)和序贯性器官衰竭评估(sequential organ failure assessment,SOFA)的评分。根据出院时的状态,将患者分为死亡组和存活组;根据住院期间是否发生脓毒症,将患者分为脓毒症组和非脓毒症组;根据是否发生休克,将脓毒症患者分为脓毒症无休克组和脓毒症休克组。采用Logistic回归分析重度烧伤患者死亡、脓毒症及脓毒症休克的危险因素。绘制受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)评估上述指标对患者死亡、脓毒症,以及脓毒症休克的早期预警作用。结果·与存活组比较,死亡组患者年龄较大,差异有统计学意义(P=0.036);烧伤总面积及行气管插管或切开在是否发生脓毒症患者中差异有统计学意义(P=0.011,P=0.001)。与存活组相比,死亡组患者血清HBP较高,差异具有统计学意义(P=0.002);与非脓毒症组相比,脓毒症组患者血清HBP水平、APACHE Ⅱ评分、SOFA评分较高,差异具有统计学意义(均P<0.05),其余指标差异均无统计学意义。与脓毒症无休克组比较,脓毒症休克组患者HBP水平较高,差异有统计学意义(P=0.008)。Logistic回归分析显示,HBP是住院期间重度烧伤患者死亡的独立危险因素,同时也是重度烧伤后脓毒症患者发生脓毒症休克的独立危险因素。ROC曲线分析显示,HBP水平预测住院期间患者死亡的ROC曲线下面积(area under the curve,AUC)为0.798;当HBP≥147.03 ng/mL时,其敏感度和特异度分别为88.33%和70.00%。HBP水平预测重度烧伤后脓毒症患者出现脓毒症休克的AUC为0.789;当HBP≥147.03 ng/mL时,其敏感度和特异度分别为90.00%和63.20%。结论·入院48 h内的血清HBP水平可作为重度烧伤患者预后以及重度烧伤脓毒症患者是否发生脓毒症休克的预警指标。
关键词:肝素结合蛋白
;
重度烧伤
;
脓毒症
;
预警指标
;
预后
Abstract
Objective ·To study early expression levels of serum heparin-binding protein (HBP) and its potential value in early alarming for prognosis and occurrence of sepsis in patients with severe burns. Methods ·Retrospective analysis was performed on medical records of 52 severely burned patients admitted to the Department of Burn and Plastic, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine during January 2021 to May 2023. General data of patients on gender, age, total burn area, body mass index (BMI), and whether endotracheal intubation or incision was performed were collected. The level of HBP, serum procalcitonin (PCT), serum C-reactive protein (CRP) and the count of white blood cells within 48 h of admission were collected. The scores of acute physiological and chronic health assessment evaluation Ⅱ (APACHE Ⅱ) and sequential organ failure assessment (SOFA) within 48 h of admission were collected. Patients were divided into death group and survival group according to the status at discharge. According to whether sepsis occurred during hospitalization, the patients were divided into sepsis group and non-sepsis group. According to whether shock occurred, the septic patients were divided into sepsis without shock group and septic shock group. Risk factors for death, sepsis, and septic shock in severely burned patients were analyzed by using Logistic regression models. Receiver operator characteristic (ROC) curve analysis was established to study risk factors, which may alarm the occurrence of poor prognosis, sepsis, and septic shock. Results ·Compared with the survival group, patients in the death group were older, and the difference was statistically significant (P=0.036). Differences in burn area and whether tracheal intubation or tracheotomy was performed were statistically significant in patients with or without sepsis (P=0.011, P=0.001). Compared with the survival group, the serum HBP levels were higher in the death group, and the difference was statistically significant (P=0.002). Compared with the non-sepsis group, patients in the sepsis group had higher levels of serum HBP, APACHE Ⅱ scores, and SOFA scores, and the differences were statistically significant (all P<0.05). The differences in other indicators were not statistically significant. Compared with the sepsis without shock group, the septic shock group had higher HBP levels, with a statistically significant difference (P=0.008). Logistic regression analysis showed that HBP was an independent risk factor for death in patients with severe burns during hospitalization and also an independent risk factor for the occurrence of septic shock in patients with sepsis after severe burns. ROC curve analysis showed that the area under the curve (AUC) for HBP in predicting patient mortality during hospitalization was 0.798; when HBP ≥147.03 ng/mL, its sensitivity and specificity were 88.33% and 70.00%, respectively. The AUC for HBP in predicting the occurrence of septic shock in patients with sepsis after severe burns was 0.789; when HBP ≥147.03 ng/mL, its sensitivity and specificity were 90.00% and 63.20%, respectively. Conclusion ·The level of serum HBP within 48 h of admission might be used as an early alarming index for prognosis in patients with severe burns and for the occurrence of septic shock in patients with sepsis following severe burns.
Keywords:heparin-binding protein (HBP)
;
severe burn
;
sepsis
;
early alarming index
;
prognosis
SONG Chenlu, XIANG Jun, YANG Huizhong. Early alarming effect of serum heparin-binding protein on prognosis and occurrence of sepsis in severely burned patients. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(4): 474-481 doi:10.3969/j.issn.1674-8115.2024.04.008
收集患者的一般资料,如性别、年龄、身体质量指数(body mass index,BMI)、烧伤总面积、致伤因素、是否行气管插管或气管切开等。记录患者入院48 h内的急性生理与慢性健康评估Ⅱ(acute physiology and chronic health evaluation Ⅱ,APACHE Ⅱ)和序贯性器官衰竭评估(sequential organ failure assessment,SOFA)评分,PCT、CRP、HBP水平,以及白细胞(white blood cell,WBC)计数,微生物培养结果等指标。临床化验标本均送至上海交通大学医学院附属瑞金医院临床检验科检测。
各指标的正常参考值为:PCT<0.5 μg/L、CRP 0~10 mg/L、WBC(4~10)×109/L、HBP<11.4 ng/mL。APACHE Ⅱ评分[8]由急性生理学评分(acute physiology score,APS)、年龄评分、慢性健康状况评分(chronic health score,CPS)3部分组成,最后得分为三者之和。其理论最高分为71分,分值越高,表示病情越重。SOFA评分[9]项目包括呼吸系统、凝血系统、消化系统(肝功能)、循环系统、神经系统和泌尿系统(肾功能)六大器官或系统功能评分组成;得分越高,提示器官/系统功能障碍或衰竭程度越严重。
SONG Chenlu was responsible for data collection and analysis. XIANG Jun was involved in the data analysis. YANG Huizhong was responsible for manuscript drafting and revising. All authors have given final approval of the version to be published.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
YAO Y M, ZHANG H, TONG Y L. Deepening the understanding of the diagnostic system and therapeutic strategy for burn sepsis[J]. Chinese Journal of Burns and Wounds, 2021, 37(5): 404-409.
WILLIAMS F N, HERNDON D N, HAWKINS H K, et al. The leading causes of death after burn injury in a single pediatric burn center[J]. Crit Care, 2009, 13(6): R183.
FISHER J, LINDER A. Heparin-binding protein: a key player in the pathophysiology of organ dysfunction in sepsis[J]. J Intern Med, 2017, 281(6): 562-574.
Editorial Committee of Guidelines for Diagnosis and Treatment of Burn Infection, Burn Physician Branch, Chinese Medical Doctor Association. Diagnostic criteria and treatment guidelines for burn infection (2012 edition)[J]. Chinese Journal of Burn, 2012, 28(6): 401-403.
SINGER M, DEUTSCHMAN C S, SEYMOUR C W, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3)[J]. JAMA, 2016, 315(8): 801-810.
JESCHKE M G, FINNERTY C C, KULP G A, et al. Can we use C-reactive protein levels to predict severe infection or sepsis in severely burned patients?[J]. Int J Burns Trauma, 2013, 3(3): 137-143.
LU Z Q, LI X, YANG P, et al. Heparin-binding protein enhances NF-κB pathway-mediated inflammatory gene transcription in M1 macrophages via lactate[J]. Inflammation, 2021, 44(1): 48-56.
LINDER A, AKESSON P, BRINK M, et al. Heparin-binding protein: a diagnostic marker of acute bacterial meningitis[J]. Crit Care Med, 2011, 39(4): 812-817.
LERTDUMRONGLUK K, THONGMEE T, KERR S J, et al. Diagnostic accuracy of urine heparin binding protein for pediatric acute pyelonephritis[J]. Eur J Pediatr, 2015, 174(1): 43-48.
MELLHAMMAR L, THELAUS L, ELÉN S, et al. Heparin binding protein in severe COVID-19: a prospective observational cohort study[J]. PLoS One, 2021, 16(4): e0249570.
SHU W Q, WAN J H, YANG X Y, et al. Heparin-binding protein levels at admission and within 24 h are associated with persistent organ failure in acute pancreatitis[J]. Dig Dis Sci, 2021, 66(10): 3597-3603.
WU Y L, YO C H, HSU W T, et al. Accuracy of heparin-binding protein in diagnosing sepsis: a systematic review and meta-analysis[J]. Crit Care Med, 2021, 49(1): e80-e90.
LINDER A, ARNOLD R, BOYD J H, et al. Heparin-binding protein measurement improves the prediction of severe infection with organ dysfunction in the emergency department[J]. Crit Care Med, 2015, 43(11): 2378-2386.
KAHN F, TVERRING J, MELLHAMMAR L, et al. Heparin-binding protein as a prognostic biomarker of sepsis and disease severity at the emergency department[J]. Shock, 2019, 52(6): e135-e145.



{kind=link}
{kind=link}
{kind=link}
{kind=link}