Efficacy and safety of compound amino acid capsules in the treatment of malnutrition and calcium and phosphorus metabolism disorders in maintenance hemodialysis patients
WU Wangshu,, WANG Minzhou, SONG Ahui, ZHAO Bingru, LU Jiayue, HONG Wenkai, GU Leyi, XIE Kewei, LU Renhua,
Department of Nephrology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200127, China
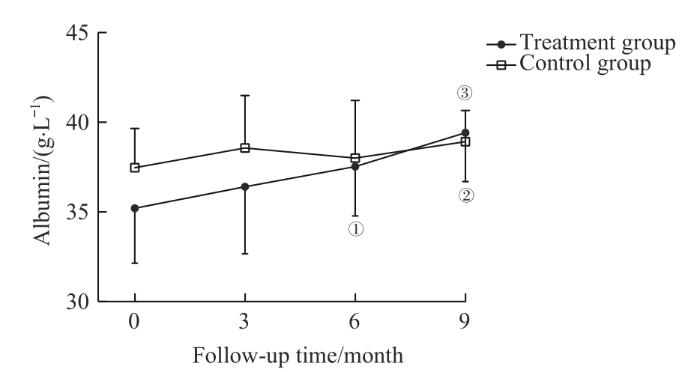
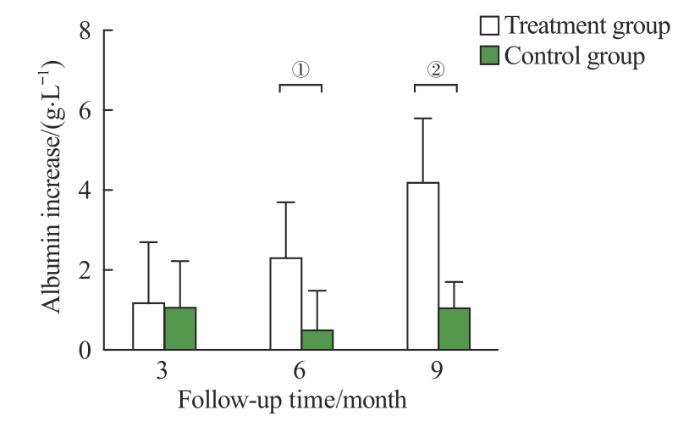
Objective ·To explore the efficacy and safety of compound amino acid capsules in the treatment of malnutrition and calcium and phosphorus metabolism disorders in maintenance hemodialysis patients.Methods ·In this prospective, randomized, controlled, single-center study, forty maintenance hemodialysis patients from Renji Hospital, Shanghai Jiao Tong University School of Medicine were randomly divided into two groups, the treatment group (n=21) and the control group (n=19). The treatment group was given oral compound amino acid capsules on the basis of regular hemodialysis treatment, while the control group received no special nutritional intervention. Serum albumin, prealbumin, hemoglobin, ferritin, calcium, phosphorus, 1,25-(OH)2-D3 and intact parathyroid hormone levels were analyzed every 3 months, and the incidence of adverse events including death, cardio-cerebrovascular accidents and vascular access failure was recorded. The total follow-up period was 9 months. Results ·Serum albumin and prealbumin in the treatment group at 6-month and 9-month were significantly higher than the baseline parameters (albumin, t=3.574, 5.599, both P<0.05; prealbumin, t/Z=-2.485, 2.921, both P<0.05). Albumin in the control group increased at 9-month with a lower amplification compared to the treatment group (t=3.877, P=0.001), while the difference of prealbumin showed no statistical significance during follow-up. Hemoglobin and serum ferritin in the treatment group started to increase at 3-month (hemoglobin, t=2.192; ferritin, t=2.994; both P<0.05). Phosphorus in treatment group decreased at 3-month and 9-month (t/Z=-2.743, -2.103, both P<0.05), while phosphorus in the control group remained relatively stable during the first 6 months and increased at 9-month (Z=-2.178, P=0.029). Calcium and 1,25-(OH)2-D3 in the treatment group at 3-month and 6-month were significantly higher than the baseline parameters (calcium, t=4.581, 4.922, both P=0.000; 1,25-(OH)2-D3t/Z=4.504, -2.374, both P<0.05), while the increase in blood calcium in the control group was significantly smaller than that in the treatment group during the same period. 1,25-(OH)2-D3 in the control group showed no significant improvement. There was no significant difference in intact parathyroid hormone level, incidence of adverse events and other laboratory examination results between the two groups. Conclusion ·Compound amino acid capsules can ameliorate the nutrition status and regulate calcium and phosphorus metabolism effectively and safely in maintenance hemodialysis patients.
WU Wangshu, WANG Minzhou, SONG Ahui, ZHAO Bingru, LU Jiayue, HONG Wenkai, GU Leyi, XIE Kewei, LU Renhua. Efficacy and safety of compound amino acid capsules in the treatment of malnutrition and calcium and phosphorus metabolism disorders in maintenance hemodialysis patients. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(8): 1023-1029 doi:10.3969/j.issn.1674-8115.2024.08.011
Note: ①P=0.002, ②P=0.000, compared with the baseline serum albumin of the treatment group; ③P=0.002, compared with the baseline serum albumin of the control group.
Fig 1
Comparison of serum albumin between the two groups
本研究使用的复方氨基酸胶囊除8种必需氨基酸外还含有A、C、D、E、B族等11种维生素,能有效补充红细胞生成所需物质。本研究发现,使用复方氨基酸胶囊治疗3个月可提高MHD患者的血红蛋白及铁蛋白水平,然而这一效应在第6~9个月并未稳定持续。李福红等[18]发现,在使用重组人促红细胞生成素(recombinant human erythropoietin,rhEPO)和口服铁剂的常规治疗基础上,补充复方氨基酸胶囊可使肾性贫血在约3个月时得到纠正,较对照组提前约2个月时间达标,且治疗组患者在贫血治疗期和维持期的rhEPO用量明显少于对照组。
The study was designed and the manuscript was written by WU Wangshu, GU Leyi, XIE Kewei and LU Renhua. The data were collected and analyzed by WU Wangshu, WANG Minzhou, SONG Ahui, ZHAO Bingru, LU Jiayue and HONG Wenkai. The manuscript was reviewed and revised by GU Leyi, XIE Kewei and LU Renhua. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
SABATINO A, REGOLISTI G, KARUPAIAH T, et al. Protein-energy wasting and nutritional supplementation in patients with end-stage renal disease on hemodialysis[J]. Clin Nutr, 2017, 36(3): 663-671.
NAGY E, MAHMOUD M, EL-KANNISHY G, et al. Impact of malnutrition on health-related quality of life in patients on maintenance hemodialysis[J]. Ther Apher Dial, 2021, 25(4): 467-474.
FU P, YUAN W J. Effects of compound amino acids capsules on hypoalbuminemia in patients with chronic renal failure undergoing hemodialysis[J]. China Pharmacy, 2005, 16(10): 764-766.
CARRERO J J, THOMAS F, NAGY K, et al. Global prevalence of protein-energy wasting in kidney disease: a meta-analysis of contemporary observational studies from the international society of renal nutrition and metabolism[J]. J Ren Nutr, 2018, 28(6): 380-392.
HANNA R M, GHOBRY L, WASSEF O, et al. A practical approach to nutrition, protein-energy wasting, sarcopenia, and Cachexia in patients with chronic kidney disease[J]. Blood Purif, 2020, 49(1/2): 202-211.
SHIRAI N, INOUE T, OGAWA M, et al. Relationship between nutrition-related problems and falls in hemodialysis patients: a narrative review[J]. Nutrients, 2022, 14(15): 3225.
BOLASCO P. Hemodialysis-nutritional flaws in diagnosis and prescriptions. could amino acid losses be the sharpest "sword of Damocles"?[J]. Nutrients, 2020, 12(6): 1773.
GRATEROL TORRES F, MOLINA M, SOLER-MAJORAL J, et al. Evolving concepts on inflammatory biomarkers and malnutrition in chronic kidney disease[J]. Nutrients, 2022, 14(20): 4297.
KLOPPENBURG W D, STEGEMAN C A, HOVINGA T K, et al. Effect of prescribing a high protein diet and increasing the dose of dialysis on nutrition in stable chronic haemodialysis patients: a randomized, controlled trial[J]. Nephrol Dial Transplant, 2004, 19(5): 1212-1223.
SAHATHEVAN S, KHOR B H, NG H M, et al. Understanding development of malnutrition in hemodialysis patients: a narrative review[J]. Nutrients, 2020, 12(10): 3147.
HENDRIKS F K, KOOMAN J P, VAN LOON L J C. Dietary protein interventions to improve nutritional status in end-stage renal disease patients undergoing hemodialysis[J]. Curr Opin Clin Nutr Metab Care, 2021, 24(1): 79-87.
IKIZLER T A, BURROWES J D, BYHAM-GRAY L D, et al. KDOQI clinical practice guideline for nutrition in CKD: 2020 update[J]. Am J Kidney Dis, 2020, 76(3 Suppl 1): S1-S107.
MA L J, ZHAO S M. Risk factors for mortality in patients undergoing hemodialysis: a systematic review and meta-analysis[J]. Int J Cardiol, 2017, 238: 151-158.
JIANG N, QIAN J Q, LIN A W, et al. Low-protein diet supplemented with keto acids is associated with suppression of small-solute peritoneal transport rate in peritoneal dialysis patients[J]. Int J Nephrol, 2011, 2011: 542704.
LI F H, SUN B, TIAN Y M. Clinical observation of compound amino acid capsules in the supplementary treatment of renal anemia in hemodialysis patients[J]. Journal of Clinical Nephrology, 2017, 17(10): 618-620.
HU L, NAPOLETANO A, PROVENZANO M, et al. Mineral bone disorders in kidney disease patients: the ever-current topic[J]. Int J Mol Sci, 2022, 23(20): 12223.
LI H M, LONG Q, SHAO C H, et al. Effect of short-term low-protein diet supplemented with keto acids on hyperphosphatemia in maintenance hemodialysis patients[J]. Blood Purif, 2011, 31(1/2/3): 33-40.
CASES A, CIGARRÁN-GULDRÍS S, MAS S, et al. Vegetable-based diets for chronic kidney disease? it is time to reconsider[J]. Nutrients, 2019, 11(6): 1263.
CARRERO J J, GONZÁLEZ-ORTIZ A, AVESANI C M, et al. Plant-based diets to manage the risks and complications of chronic kidney disease[J]. Nat Rev Nephrol, 2020, 16(9): 525-542.
... 本研究使用的复方氨基酸胶囊除8种必需氨基酸外还含有A、C、D、E、B族等11种维生素,能有效补充红细胞生成所需物质.本研究发现,使用复方氨基酸胶囊治疗3个月可提高MHD患者的血红蛋白及铁蛋白水平,然而这一效应在第6~9个月并未稳定持续.李福红等[18]发现,在使用重组人促红细胞生成素(recombinant human erythropoietin,rhEPO)和口服铁剂的常规治疗基础上,补充复方氨基酸胶囊可使肾性贫血在约3个月时得到纠正,较对照组提前约2个月时间达标,且治疗组患者在贫血治疗期和维持期的rhEPO用量明显少于对照组. ...
1
... 本研究使用的复方氨基酸胶囊除8种必需氨基酸外还含有A、C、D、E、B族等11种维生素,能有效补充红细胞生成所需物质.本研究发现,使用复方氨基酸胶囊治疗3个月可提高MHD患者的血红蛋白及铁蛋白水平,然而这一效应在第6~9个月并未稳定持续.李福红等[18]发现,在使用重组人促红细胞生成素(recombinant human erythropoietin,rhEPO)和口服铁剂的常规治疗基础上,补充复方氨基酸胶囊可使肾性贫血在约3个月时得到纠正,较对照组提前约2个月时间达标,且治疗组患者在贫血治疗期和维持期的rhEPO用量明显少于对照组. ...



{kind=link}
{kind=link}
{kind=link}
{kind=link}