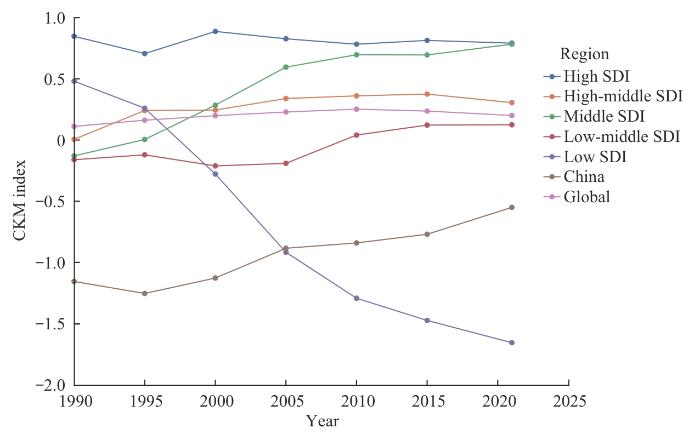
目的·基于2021年全球疾病负担(Global Burden of Disease,GBD)研究(GBD 2021)项目,构建心血管-肾脏-代谢(cardiovascular-kidney-metabolic,CKM)指数,系统评估心血管疾病、慢性肾脏病与代谢性疾病的协同负担特征,揭示其在全球范围内的时空分布规律和相互关联性。方法·数据来源于GBD 2021项目,涵盖1990—2021年204个国家和地区。提取缺血性心脏病、慢性肾脏病与2型糖尿病的伤残调整生命年(disability-adjusted life year,DALY)率,计算年龄标准化DALY率,并采用Z分数标准化后等权重算术平均值作为CKM指数。利用Joinpoint回归模型对CKM指数的时间序列进行趋势分段拟合,识别不同发展阶段的变化拐点及年均变化率。结合社会人口学发展指数(socio-demographic index,SDI)分区,对不同国家和地区进行归类比较。使用Spearman秩相关分析检验3类疾病DALY率之间的相关性。结果·2021年,全球CKM指数为0.201。时间趋势分析显示1990—2021年全球CKM综合征负担总体呈上升趋势,年均增幅为0.002 9。其中,中SDI国家的增长最为显著,CKM指数由-0.130上升至0.783,年均增幅为0.029 4;中高SDI国家与中低SDI国家亦呈现稳定上升趋势,年均增幅分别为0.009 7和0.009 2;而在高SDI国家中,CKM指数自1990年的0.847下降至2010年的0.783,随后略回升至2021年的0.792。全球204个国家和地区的相关性分析显示3类疾病DALY率之间存在不同程度的正相关,其中慢性肾脏病与2型糖尿病相关性最强(r=0.66,P<0.001),缺血性心脏病与慢性肾脏病相关性较弱(r=0.20,P=0.004)。结论·研究构建的CKM指数可为评估多疾病共存负担提供分类量化工具。CKM指数分析结果揭示了心血管疾病、慢性肾脏病与代谢性疾病既存在共同危险因素,也存在协同进展的病理通路,应成为全球慢性疾病防控的重点线索。建议公共卫生政策打破体系分隔,强化对CKM综合征的快速识别与全程管理,提升慢性疾病防治效率。
关键词:心血管-肾脏-代谢综合征
;
全球疾病负担
;
多疾病共存
;
整合性管理
Abstract
Objective ·To construct a cardiovascular-kidney-metabolic (CKM) index based on the Global Burden of Disease (GBD) 2021 study, systematically evaluate the synergistic burden of cardiovascular diseases, chronic kidney diseases, and metabolic disorders, and reveal their spatiotemporal distribution patterns and interrelationships worldwide. Methods ·The data were derived from the GBD 2021 project, encompassing 204 countries and regions over the period from 1990 to 2021. The disability-adjusted life year (DALY) rates for ischemic heart disease, chronic kidney disease, and type 2 diabetes mellitus were extracted, age-standardized DALY rates were calculated, and then the CKM index was computed through equal-weighted averaging of these rates after Z-score standardization. The Joinpoint regression models were applied to the CKM index time series for segmented trend fitting, to identify turning points and annual percentage changes at different developmental stages. Countries and regions were categorized and compared according to their socio-demographic index (SDI) levels. Spearman's rank correlation was used to assess the correlations among DALY rates for the three disease categories. Results ·In 2021, the global CKM index value was 0.201. Temporal trend analysis showed that global CKM syndrome burden generally increased from 1990 to 2021, with an average annual increase of 0.002 9. Among these, middle-SDI countries showed the most significant growth, with CKM index rising from -0.130 to 0.783, representing an average annual increase of 0.029 4. High-middle SDI and low-middle SDI countries also demonstrated steady upward trends, with average annual increases of 0.009 7 and 0.009 2, respectively. In high-SDI countries, the CKM index declined from 0.847 in 1990 to its lowest point of 0.783 in 2010, and then rose slightly to 0.792 in 2021. Correlation analysis across 204 countries and regions globally revealed varying degrees of positive correlation among the three types of diseases in terms of DALY rates, with the strongest correlation observed between chronic kidney disease and type 2 diabetes mellitus (r=0.66, P<0.001), while the correlation between ischemic heart disease and chronic kidney disease was weaker (r=0.20, P=0.004). Conclusion ·The CKM index developed in this study provides a categorized and quantitative tool for assessing the burden of multimorbidity. The application of CKM index analysis revealed that cardiovascular diseases, chronic kidney diseases, and metabolic diseases not only share common risk factors but also have synergistic pathological pathways, which should be key clues for global chronic disease prevention and control. Public health policies should break down system silos, strengthen rapid identification and comprehensive management of CKM, and improve the efficiency of chronic disease prevention and treatment.
Keywords:cardiovascular-kidney-metabolic (CKM) syndrome
;
Global Burden of Disease (GBD)
;
multimorbidity
;
integrated management
HE Jiaxin, BAI Jianling. Global distribution and temporal trends of cardiovascular-kidney-metabolic syndrome burden: a systematic analysis based on GBD 2021. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(12): 1629-1635 doi:10.3969/j.issn.1674-8115.2025.12.008
本研究数据来自美国华盛顿大学健康指标与评估研究所(Institute for Health Metrics and Evaluation,IHME)发布的GBD 2021项目,数据提取涵盖1990—2021年全球204个国家和地区的疾病负担。通过GBD Results Tool在线平台(http://ghdx.healthdata.org/gbd-results-tool),根据社会人口学发展指数(socio-demographic index,SDI)分区,以及国家和地区,分别进行数据提取。其中,SDI是一项结合各地区的人均收入、平均受教育年限和25岁以下女性生育率的综合指标,分数范围为0~100分,分数越高表示社会经济条件越好。提取的疾病相关数据包括以下3项。①心血管疾病:选取缺血性心脏病(GBD病因编号B.2.2.1)伤残调整生命年(disability-adjusted life year,DALY)率。②慢性肾脏病:选取慢性肾脏病的总体(GBD病因编号B.6.1)DALY率。③代谢性疾病:选取2型糖尿病(type 2 diabetes mellitus,T2DM)(GBD病因编号B.8.2)DALY率。所有DALY率均采用世界卫生组织(WHO)世界标准人口进行年龄标准化,单位为每10万人口。
为识别CKM指数在1990—2021年的变化趋势拐点,本研究采用Joinpoint Regression Program软件(版本4.9)进行时间序列拟合分析。模型参数设定如下:最大允许变化点(Joinpoints)为3个,最小间隔年份为4年,使用贝叶斯信息准则(Bayesian information criterion,BIC)作为模型优度选择依据。采用蒙特卡洛置换检验法评估拐点显著性。该方法能够精确识别趋势变化的关键时间节点,适用于流行病学时间序列的动态变化分析。
对尚处发展转型期的中低收入国家而言,CKM综合征防控既是挑战亦是机遇。由于其尚未建立固化的专科分割体系,反而具备“从零起步构建整合性服务”的制度优势。针对中低收入国家,我们建议:开展社区联合筛查(高血压+糖尿病+蛋白尿);实施以成本效益为核心的资源敏感型CKM综合征防控简化路径;开展卫生与非卫生健康部门(如食物环境、城乡规划等)联动策略[18];通过南南合作平台推动技术共享与本地化管理路径共建,将CKM综合征正式纳入国家慢性病防控战略,增强政策一体性[37]。例如,印度国家非传染性疾病控制计划(National Programme for Prevention & Control of Cancer,Diabetes, Cardiovascular Diseases & Stroke,NPCDCS)已在多个邦推行“三病共筛”(糖尿病、高血压、蛋白尿)策略;该计划通过基层社区卫生工作者使用统一的筛查表单及便携式设备实现慢性病早期识别,并与电子健康平台对接,显著提升慢性病识别率[38]。针对发展转型期国家,我们也建议:建立基于风险评估的社区联合筛查体系,设计涵盖高血压家族史、糖尿病家族史及蛋白尿检测等的多病共筛问卷,依托现有基本公共卫生服务平台实施筛查;构建整合型基层随访模式,以患者为中心整合电子健康档案,在单次随访中同时管理3类慢性病风险,采用简化路径实现标准化随访流程;实施药品统一采购策略,重点配置钠-葡萄糖协同转运蛋白2抑制剂等具有心肾代谢三重保护作用的药物,推行成本分级医保报销制度,确保目标人群获得重点保障和精准干预。
HE Jiaxin participated in the research design, data extraction, data analysis, and manuscript writing and revision. BAI Jianling was responsible for the guidance of the project, and for reviewing and revising the manuscript. Both authors have read the final version of the manuscript and consented to submission.
利益冲突声明
所有作者声明不存在利益冲突。
Conflict of Interests
All authors declare no relevant conflict of interests.
NDUMELE C E, NEELAND I J, TUTTLE K R, et al. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome:a scientific statement from the American Heart Association[J]. Circulation, 2023, 148(20): 1636-1664.
SEBASTIAN S A, PADDA I, JOHAL G. Cardiovascular-kidney-metabolic (CKM) syndrome: a state-of-the-art review[J]. Curr Probl Cardiol, 2024, 49(2): 102344.
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990—2019: a systematic analysis for the Global Burden of Disease Study 2019[J]. Lancet, 2020, 396(10258): 1204-1222.
ROTH G A, MENSAH G A, JOHNSON C O, et al. Global burden of cardiovascular diseases and risk factors, 1990—2019: update from the GBD 2019 study[J]. J Am Coll Cardiol, 2020, 76(25): 2982-3021.
GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990—2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2020, 395(10225): 709-733.
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease[J]. Kidney Int, 2024, 105(4S): S117-S314.
NDUMELE C E, RANGASWAMI J, CHOW S L, et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association[J]. Circulation, 2023, 148(20): 1606-1635.
VAN DER HAM M, BOLIJN R, DE VRIES A, et al. Gender inequality and the double burden of disease in low-income and middle-income countries: an ecological study[J]. BMJ Open, 2021, 11(4): e047388.
XIA Y, WU Q J, WANG H Y, et al. Global, regional and national burden of gout, 1990—2017: a systematic analysis of the Global Burden of Disease Study[J]. Rheumatology (Oxford), 2020, 59(7): 1529-1538.
NCD Risk Factor Collaboration (NCD-RISC). Worldwide trends in underweight and obesity from 1990 to 2022: a pooled analysis of 3 663 population-representative studies with 222 million children, adolescents, and adults[J]. Lancet, 2024, 403(10431): 1027-1050.
GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990—2021: a systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet, 2024, 403(10440): 2162-2203.
SINDHU D, SHARMA G S, KUMBALA D. Management of diabetic kidney disease: where do we stand?: a narrative review[J]. Medicine (Baltimore), 2023, 102(13): e33366.
LEVIN A, TONELLI M, BONVENTRE J, et al. Global kidney health 2017 and beyond: a roadmap for closing gaps in care, research, and policy[J]. Lancet, 2017, 390(10105): 1888-1917.
OGUNLAYI F, COLEMAN P C, FAT L N, et al. Trends in socioeconomic inequalities in behavioural non-communicable disease risk factors: analysis of repeated cross-sectional health surveys in England between 2003 and 2019[J]. BMC Public Health, 2023, 23(1): 1442.
AN L W, WANG D D, SHI X R, et al. Differences in prevalence and management of chronic kidney disease among T2DM inpatients at the grassroots in Beijing and Taiyuan: a retrospective study[J]. J Health Popul Nutr, 2023, 42(1): 61.
LEINER J, PELLISSIER V, KÖNIG S, et al. Patient characteristics and outcomes of hospitalized chronic kidney disease patients with and without type 2 diabetes mellitus: observations from the German claims data-based cohort of the CaReMe-CKD multinational study[J]. Clin Epidemiol, 2024, 16: 487-500.
THEODORAKIS N, NIKOLAOU M. From cardiovascular-kidney-metabolic syndrome to cardiovascular-renal-hepatic-metabolic syndrome: proposing an expanded framework[J]. Biomolecules, 2025, 15(2): 213.
CHOI Y, JACOBS D R Jr, SHROFF G R, et al. Progression of chronic kidney disease risk categories and risk of cardiovascular disease and total mortality: coronary artery risk development in young adults cohort[J]. J Am Heart Assoc, 2022, 11(21): e026685.
CHERNEY D Z I, REPETTO E, WHEELER D C, et al. Impact of cardio-renal-metabolic comorbidities on cardiovascular outcomes and mortality in type 2 diabetes mellitus[J]. Am J Nephrol, 2020, 51(1): 74-82.
PERKOVIC V, TUTTLE K R, ROSSING P, et al. Effects of semaglutide on chronic kidney disease in patients with type 2 diabetes[J]. N Engl J Med, 2024, 391(2): 109-121.
YANG J S, MAMUDU H M, MACKEY T K. Governing noncommunicable diseases through political rationality and technologies of government: a discourse analysis[J]. Int J Environ Res Public Health, 2020, 17(12): 4413.
TONELLI M, WIEBE N, RICHARD J F, et al. Characteristics of adults with type 2 diabetes mellitus by category of chronic kidney disease and presence of cardiovascular disease in Alberta Canada: a cross-sectional study[J]. Can J Kidney Health Dis, 2019, 6: 2054358119854113.
COLLISTER D, PYNE L, CUNNINGHAM J, et al. Multidisciplinary chronic kidney disease clinic practices: a scoping review[J]. Can J Kidney Health Dis, 2019, 6: 2054358119882667.
GIORGINO F, VORA J, FENICI P, et al. Renoprotection with SGLT2 inhibitors in type 2 diabetes over a spectrum of cardiovascular and renal risk[J]. Cardiovasc Diabetol, 2020, 19(1): 196.
PERKOVIC V, JARDINE M J, NEAL B, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy[J]. N Engl J Med, 2019, 380(24): 2295-2306.
LAM C S P, CHANDRAMOULI C, AHOOJA V, et al. SGLT-2 inhibitors in heart failure: current management, unmet needs, and therapeutic prospects[J]. J Am Heart Assoc, 2019, 8(20): e013389.
WHEELER D C, STEFÁNSSON B V, JONGS N, et al. Effects of dapagliflozin on major adverse kidney and cardiovascular events in patients with diabetic and non-diabetic chronic kidney disease: a prespecified analysis from the DAPA-CKD trial[J]. Lancet Diabetes Endocrinol, 2021, 9(1): 22-31.
BHATT D L, SZAREK M, PITT B, et al. Sotagliflozin in patients with diabetes and chronic kidney disease[J]. N Engl J Med, 2021, 384(2): 129-139.
KYRIAZAKOS S, PNEVMATIKAKIS A, KOSTOPOULOU K, et al. Benchmarking the clinical outcomes of Healthentia SaMD in chronic disease management: a systematic literature review comparison[J]. Front Public Health, 2024, 12: 1488687.
Ministry of Health & Family Welfare Government of India. National programme for prevention & control of cancer, diabetes, cardiovascular diseases & stroke (NPCDCS)[EB/OL]. [2025-06-17]. https://nhm.gov.in/index1.php?lang=1&level=2&sublinkid=1048&lid=604.
... 对尚处发展转型期的中低收入国家而言,CKM综合征防控既是挑战亦是机遇.由于其尚未建立固化的专科分割体系,反而具备“从零起步构建整合性服务”的制度优势.针对中低收入国家,我们建议:开展社区联合筛查(高血压+糖尿病+蛋白尿);实施以成本效益为核心的资源敏感型CKM综合征防控简化路径;开展卫生与非卫生健康部门(如食物环境、城乡规划等)联动策略[18];通过南南合作平台推动技术共享与本地化管理路径共建,将CKM综合征正式纳入国家慢性病防控战略,增强政策一体性[37].例如,印度国家非传染性疾病控制计划(National Programme for Prevention & Control of Cancer,Diabetes, Cardiovascular Diseases & Stroke,NPCDCS)已在多个邦推行“三病共筛”(糖尿病、高血压、蛋白尿)策略;该计划通过基层社区卫生工作者使用统一的筛查表单及便携式设备实现慢性病早期识别,并与电子健康平台对接,显著提升慢性病识别率[38].针对发展转型期国家,我们也建议:建立基于风险评估的社区联合筛查体系,设计涵盖高血压家族史、糖尿病家族史及蛋白尿检测等的多病共筛问卷,依托现有基本公共卫生服务平台实施筛查;构建整合型基层随访模式,以患者为中心整合电子健康档案,在单次随访中同时管理3类慢性病风险,采用简化路径实现标准化随访流程;实施药品统一采购策略,重点配置钠-葡萄糖协同转运蛋白2抑制剂等具有心肾代谢三重保护作用的药物,推行成本分级医保报销制度,确保目标人群获得重点保障和精准干预. ...
... 对尚处发展转型期的中低收入国家而言,CKM综合征防控既是挑战亦是机遇.由于其尚未建立固化的专科分割体系,反而具备“从零起步构建整合性服务”的制度优势.针对中低收入国家,我们建议:开展社区联合筛查(高血压+糖尿病+蛋白尿);实施以成本效益为核心的资源敏感型CKM综合征防控简化路径;开展卫生与非卫生健康部门(如食物环境、城乡规划等)联动策略[18];通过南南合作平台推动技术共享与本地化管理路径共建,将CKM综合征正式纳入国家慢性病防控战略,增强政策一体性[37].例如,印度国家非传染性疾病控制计划(National Programme for Prevention & Control of Cancer,Diabetes, Cardiovascular Diseases & Stroke,NPCDCS)已在多个邦推行“三病共筛”(糖尿病、高血压、蛋白尿)策略;该计划通过基层社区卫生工作者使用统一的筛查表单及便携式设备实现慢性病早期识别,并与电子健康平台对接,显著提升慢性病识别率[38].针对发展转型期国家,我们也建议:建立基于风险评估的社区联合筛查体系,设计涵盖高血压家族史、糖尿病家族史及蛋白尿检测等的多病共筛问卷,依托现有基本公共卫生服务平台实施筛查;构建整合型基层随访模式,以患者为中心整合电子健康档案,在单次随访中同时管理3类慢性病风险,采用简化路径实现标准化随访流程;实施药品统一采购策略,重点配置钠-葡萄糖协同转运蛋白2抑制剂等具有心肾代谢三重保护作用的药物,推行成本分级医保报销制度,确保目标人群获得重点保障和精准干预. ...
1
... 对尚处发展转型期的中低收入国家而言,CKM综合征防控既是挑战亦是机遇.由于其尚未建立固化的专科分割体系,反而具备“从零起步构建整合性服务”的制度优势.针对中低收入国家,我们建议:开展社区联合筛查(高血压+糖尿病+蛋白尿);实施以成本效益为核心的资源敏感型CKM综合征防控简化路径;开展卫生与非卫生健康部门(如食物环境、城乡规划等)联动策略[18];通过南南合作平台推动技术共享与本地化管理路径共建,将CKM综合征正式纳入国家慢性病防控战略,增强政策一体性[37].例如,印度国家非传染性疾病控制计划(National Programme for Prevention & Control of Cancer,Diabetes, Cardiovascular Diseases & Stroke,NPCDCS)已在多个邦推行“三病共筛”(糖尿病、高血压、蛋白尿)策略;该计划通过基层社区卫生工作者使用统一的筛查表单及便携式设备实现慢性病早期识别,并与电子健康平台对接,显著提升慢性病识别率[38].针对发展转型期国家,我们也建议:建立基于风险评估的社区联合筛查体系,设计涵盖高血压家族史、糖尿病家族史及蛋白尿检测等的多病共筛问卷,依托现有基本公共卫生服务平台实施筛查;构建整合型基层随访模式,以患者为中心整合电子健康档案,在单次随访中同时管理3类慢性病风险,采用简化路径实现标准化随访流程;实施药品统一采购策略,重点配置钠-葡萄糖协同转运蛋白2抑制剂等具有心肾代谢三重保护作用的药物,推行成本分级医保报销制度,确保目标人群获得重点保障和精准干预. ...



{kind=link}
{kind=link}