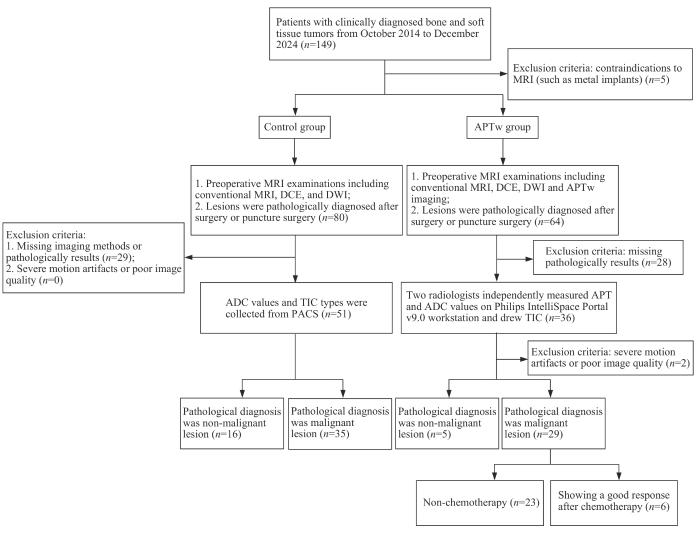
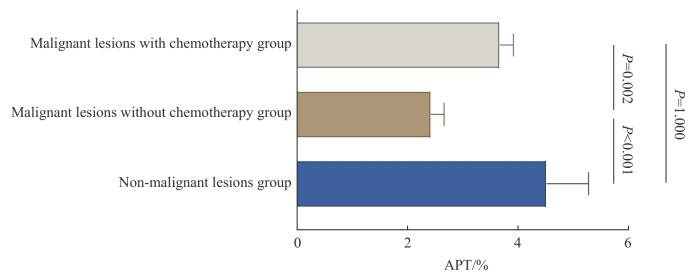
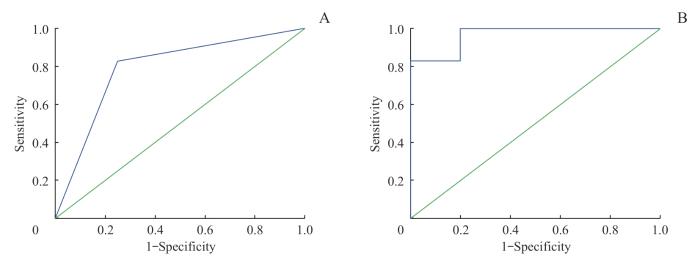
Objective ·To preliminarily investigate the value of high-order functional magnetic resonance imaging in the evaluation of benign and malignant bone and soft tissue tumors and the changes after chemotherapy. Methods ·Patients clinically diagnosed with bone and soft tissue tumors at the Department of Orthopaedics, Shanghai Ninth People 's Hospital, Shanghai Jiao Tong University School of Medicine, from October 2014 to December 2024 were enrolled. The patients were divided into a control group and an amide proton transfer-weighted imaging (APTw) group according to the imaging method. All patients underwent conventional magnetic resonance imaging (MRI), diffusion-weighted imaging (DWI), and dynamic contrast-enhanced imaging (DCE) before surgery. Patients in the APTw group received additional APTw imaging. Both groups were divided into non-malignant and malignant lesion subgroups according to pathological results. According to whether the patients received chemotherapy before enrollment, the patients with malignant lesions in the APTw group were further divided into malignant group without chemotherapy and malignant group with chemotherapy. Clinical and imaging data, including APT values, apparent diffusion coefficient (ADC), and time-intensity curves (TICs) from the largest tumor section, were collected and analyzed to assess the diagnostic performance of APTw, DWI, and DCE, and to evaluate changes after chemotherapy. Results ·Eighty-five patients were enrolled, including 51 males and 34 females, with ages ranging from 10 to 84 years, and a mean age of (43.05±17.62) years. There were 51 patients in the control group (16 with non-malignant lesions and 35 with malignant lesions) and 34 patients in the APTw group (5 with non-malignant lesions and 29 with malignant lesions; 23 malignant lesions without chemotherapy and 6 malignant lesions with chemotherapy). The clinical and imaging data showed that only the tumor margin of the control group and the maximum tumor diameter of the APTw group had statistically significant differences in their malignant and non-malignant lesion groups ( P<0.05). In the APTw group, there was a statistically significant difference in APT values between the malignant lesion group and the non-malignant lesion group ( P<0.001). Further analysis showed that the APT values in the malignant group without chemotherapy were significantly lower than that in the malignant group with chemotherapy ( P<0.001). However, there were no statistically significant differences in APT values between the malignant group with chemotherapy and the non-malignant lesion group ( P>0.05). There were no significant differences in ADC values and TIC types between malignant and non-malignant lesion groups in the control group and the APTw group ( P>0.05). The area under the curve (AUC) of the diagnostic model in the APTw group (MRI+DWI+DCE+APTw) for distinguishing malignant from benign tumors was significantly higher than that of the control group (MRI+DWI+DCE) ( P<0.05). The Youden index and specificity of the diagnostic model in the APTw group were higher than those in the control group. Conclusion ·As a high-order functional MRI technique, APTw imaging is capable of evaluating the nature (benign or malignant) of bone and soft tissue tumors and detecting changes after chemotherapy. It serves as a valuable supplement to conventional MRI, DWI, and DCE imaging, providing a novel noninvasive tool for the diagnosis and treatment evaluation of bone and soft tissue tumors.
Keywords:bone neoplasm
;
soft tissue neoplasm
;
amide proton transfer
;
diffusion magnetic resonance imaging
;
neoadjuvant therapy
ZHANG Zhengjia, LI Xiaomin, ZHOU Xin, MA Hairong, AI Songtao. Preliminary study on the value of high-order functional magnetic resonance imaging in the evaluation of bone and soft tissue tumors. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(5): 585-596 doi:10.3969/j.issn.1674-8115.2025.05.007
Tab 5 APT and ADC values, and TIC classifications in APTw group patients with malignant lesions, comparing those who received chemotherapy with those who did not
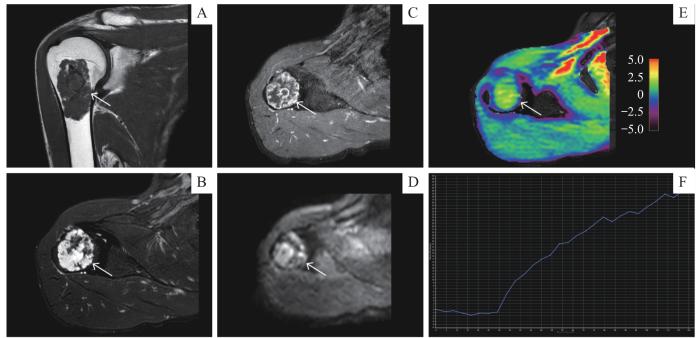
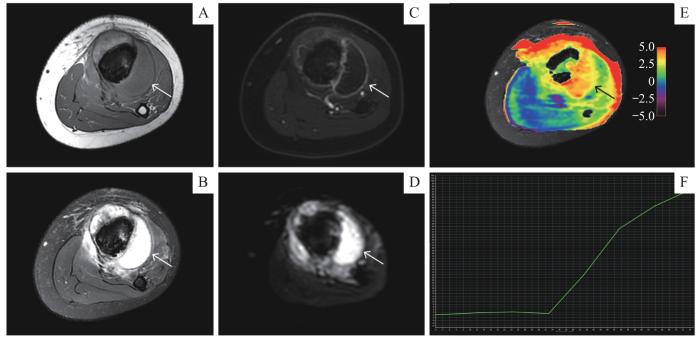
Note: A 52-year-old male with chondrosarcoma of the right humerus. A. Coronal T1-weighted MRI sequence. B. Axial T2-weighted fat-saturated MRI sequence. C. Axial contrast-enhanced T1-weighted MRI sequence. D. Axial DWI ( b=1 000 s·mm -2) sequence. E. Axial APT image fused with axial T2WI (the color bar indicates the APT values). F. TIC classification (type Ⅰ).
Fig 4
Application of APTw imaging to malignant bone tumor
病例2,患者,男,12岁,左小腿疼痛3周余,以左侧胫骨恶性肿瘤收治入院,已完成4次顺铂和脂质体阿霉素的新辅助化疗方案。术前MRI增强检查结果( 图5)示左侧胫骨干骨质破坏,周围皮质破坏、形成软组织肿块,突破骺板,累及骨骺,肿瘤最大直径约18.92 cm。DCE-TIC曲线Ⅰ型,ADC值1.97×10 -3 mm 2/s,提示对化疗效果的评估有限。APTw成像测得APT值为3.67%,显著高于未化疗的恶性肿瘤参考值,提示肿瘤对化疗有反应。这表明APT值在化疗后有所回升,符合肿瘤细胞对化疗药物的敏感性( 图5E)。术后病理提示骨肉瘤化疗后改变,与APTw成像评估结果相符。
Note: A 12-year-old male with osteosarcoma in the left tibia showed chemotherapy-related changes. A. Axial T1-weighted MRI sequence. B. Axial T2-weighted fat-saturated MRI sequence. C. Axial contrast-enhanced T1-weighted MRI sequence. D. Axial DWI ( b=1 000 s·mm -2) sequence. E. Axial APT image fused with axial T2WI (the color bar indicates the APT values). F. TIC classification (type Ⅰ).
Fig 5
Application of APTw imaging in neoadjuvant chemotherapy for malignant bone tumor
ZHANG Zhengjia contributed to data acquisition, statistical analysis and manuscript preparation. LI Xiaomin and AI Songtao contributed to the overall design of research and the review of the paper. ZHOU Xin and MA Hairong contributed to the data acquisition. All authors have read the final version of paper and consented to its submission.
利益冲突声明
所有作者声明无利益冲突。
COMPETING INTERESTS
All authors declare no relevant conflict of interests.
COLE S, MATTHEW GIANFERANTE D, ZHU B, et al. Osteosarcoma: a surveillance, epidemiology, and end results program-based analysis from 1975 to 2017[J]. Cancer, 2022, 128(11): 2107-2118.
JAFARI F, JAVDANSIRAT S, SANAIE S, et al. Osteosarcoma: a comprehensive review of management and treatment strategies[J]. Ann Diagn Pathol, 2020, 49: 151654.
CHOI J H, RO J Y. The recent advances in molecular diagnosis of soft tissue tumors[J]. Int J Mol Sci, 2023, 24(6): 5934.
TANAKA K, OZAKI T. Adjuvant and neoadjuvant chemotherapy for soft tissue sarcomas: JCOG Bone and Soft Tissue Tumor Study Group[J]. Jpn J Clin Oncol, 2021, 51(2): 180-184.
YUAN W Z, YU Q Y, WANG Z, et al. Efficacy of diffusion-weighted imaging in neoadjuvant chemotherapy for osteosarcoma: a systematic review and meta-analysis[J]. Acad Radiol, 2022, 29(2): 326-334.
HABRE C, DABADIE A, LOUNDOU A D, et al. Diffusion-weighted imaging in differentiating mid-course responders to chemotherapy for long-bone osteosarcoma compared to the histologic response: an update[J]. Pediatr Radiol, 2021, 51(9): 1714-1723.
LI J L, XU Y, XIANG Y S, et al. The value of amide proton transfer MRI in the diagnosis of malignant and benign urinary bladder lesions: comparison with diffusion-weighted imaging[J]. J Magn Reson Imaging, 2024, 60(3): 1124-1133.
SETIAWATI R, NOVARIYANTO B, RAHARDJO P, et al. Characteristic of apparent diffusion coefficient and time intensity curve analysis of dynamic contrast enhanced MRI in osteosarcoma histopathologic subtypes[J]. Int J Med Sci, 2023, 20(2): 163-171.
COSTA F M, CANELLA C, GASPARETTO E. Advanced magnetic resonance imaging techniques in the evaluation of musculoskeletal tumors[J]. Radiol Clin North Am, 2011, 49(6): 1325-1358, Ⅶ-Ⅷ.
ZHAO A, WU X Y, FU T, et al. Value of DWI, DCE and APT imaging in identifying benign and malignant breast lesions[J]. China Medical Devices, 2024, 39(6): 124-130, 155.
KUANG F, YAN Z P, LI H L, et al. Diagnostic accuracy of diffusion-weighted MRI for differentiation of cervical cancer and benign cervical lesions at 3.0T: comparison with routine MRI and dynamic contrast-enhanced MRI[J]. J Magn Reson Imaging, 2015, 42(4): 1094-1099.
ZHOU J Y, HEO H Y, KNUTSSON L, et al. APT-weighted MRI: techniques, current neuro applications, and challenging issues[J]. J Magn Reson Imaging, 2019, 50(2): 347-364.
WU M H, JIANG T L, GUO M, et al. Amide proton transfer-weighted imaging and derived radiomics in the classification of adult-type diffuse gliomas[J]. Eur Radiol, 2024, 34(5): 2986-2996.
LI Y, LIN C Y, QI Y F, et al. Non-invasive differentiation of endometrial adenocarcinoma from benign lesions in the uterus by utilization of amide proton transfer-weighted MRI[J]. Mol Imaging Biol, 2021, 23(3): 446-455.
LIU Z, WEN J, WANG M, et al. Breast amide proton transfer imaging at 3 T: diagnostic performance and association with pathologic characteristics[J]. J Magn Reson Imaging, 2023, 57(3): 824-833.
DENG H Z, ZHANG H W, HUANG B, et al. Advances in diffuse glioma assessment: preoperative and postoperative applications of chemical exchange saturation transfer[J]. Front Neurosci, 2024, 18: 1424316.
QAMAR S, KING A D, AI Q H, et al. Pre-treatment amide proton transfer imaging predicts treatment outcome in nasopharyngeal carcinoma[J]. Eur Radiol, 2020, 30(11): 6339-6347.
ZHANG N, SONG Q W, LIANG H B, et al. Early prediction of pathological response to neoadjuvant chemotherapy of breast tumors: a comparative study using amide proton transfer-weighted, diffusion weighted and dynamic contrast enhanced MRI[J]. Front Med (Lausanne), 2024, 11: 1295478.
SHI T L, YANG C S, LIU Y Z, et al. The value of APT imaging in evaluating the therapeutic efficacy of concurrent chemoradiotherapy for cervical cancer[J]. Chinese Journal of Magnetic Resonance Imaging, 2024, 15(1): 132-136.
LIU S R, CAI X R, QIU L. Interpretation of the new WHO classification of bone tumors (2020) [J]. Chinese Journal of Magnetic Resonance Imaging, 2020, 11(12): 1086-1091.
FANG S G, WEI J G, CHEN Z W. WHO classification of soft tissue tumors (2020) [J]. Chinese Journal of Clinical and Experimental Pathology, 2020, 36(9): 1132-1134.
CHOI Y J, LEE I S, SONG Y S, et al. Diagnostic performance of diffusion-weighted (DWI) and dynamic contrast-enhanced (DCE) MRI for the differentiation of benign from malignant soft-tissue tumors[J]. J Magn Reson Imaging, 2019, 50(3): 798-809.
HAYAKAWA K, MATSUMOTO S, AE K, et al. Definitive surgery of primary lesion should be prioritized over preoperative chemotherapy to treat high-grade osteosarcoma in patients aged 41‒65 years[J]. J Orthop Traumatol, 2020, 21(1): 13.
CAO Z Y, ZHANG Y L, XU Q, et al. The role of chemotherapy in the survival benefits of patients aged older than 40 years with osteosarcoma[J]. Technol Cancer Res Treat, 2021, 20: 15330338211066195.
GUO Z X, QIN X Y, MU R H, et al. Amide proton transfer could provide more accurate lesion characterization in the transition zone of the prostate[J]. J Magn Reson Imaging, 2022, 56(5): 1311-1319.
TOGAO O, YOSHIURA T, KEUPP J, et al. Amide proton transfer imaging of adult diffuse gliomas: correlation with histopathological grades[J]. Neuro Oncol, 2014, 16(3): 441-448.
MENG N, WANG X J, SUN J, et al. Comparative study of amide proton transfer-weighted imaging and intravoxel incoherent motion imaging in breast cancer diagnosis and evaluation[J]. J Magn Reson Imaging, 2020, 52(4): 1175-1186.
KOIKE H, MORIKAWA M, ISHIMARU H, et al. Amide proton transfer-chemical exchange saturation transfer imaging of intracranial brain tumors and tumor-like lesions: our experience and a review[J]. Diagnostics (Basel), 2023, 13(5): 914.
YANG L, WANG L, TAN Y C, et al. Amide Proton Transfer-weighted MRI combined with serum prostate-specific antigen levels for differentiating malignant prostate lesions from benign prostate lesions: a retrospective cohort study[J]. Cancer Imaging, 2023, 23(1): 3.
JIA G, ABAZA R, WILLIAMS J D, et al. Amide proton transfer MR imaging of prostate cancer: a preliminary study[J]. J Magn Reson Imaging, 2011, 33(3): 647-654.
ZHANG H W, LIU X L, ZHANG H B, et al. Differentiation of meningiomas and gliomas by amide proton transfer imaging: a preliminary study of brain tumour infiltration[J]. Front Oncol, 2022, 12: 886968.
LI Y,CHENG J L, REN C P, et al. 3D amide proton transfer weighted imaging combined with diffusion weighted imaging for differentiating benign and malignant bone and soft tissue tumors[J]. Chinese Journal of Medical Imaging Technology, 2024, 40(10): 1572-1576.
LI Y, LIN L J, ZHANG Y, et al. Preliminary exploration of amide proton transfer weighted imaging in differentiation between benign and malignant bone tumors[J]. Front Oncol, 2024, 14: 1402628.
LIU J C, CUI J L, LI S L, et al. The role of apparent diffusion coefficient in the differentiation between benign and malignant bone tumors[J]. Chinese Journal of Radiology, 2009, 43(6): 567-570.
HAYASHIDA Y, HIRAI T, YAKUSHIJI T, et al. Evaluation of diffusion-weighted imaging for the differential diagnosis of poorly contrast-enhanced and T2-prolonged bone masses: initial experience[J]. J Magn Reson Imaging, 2006, 23(3): 377-382.
WANG T T, WU X R, CUI Y F, et al. Role of apparent diffusion coefficients with diffusion-weighted magnetic resonance imaging in differentiating between benign and malignant bone tumors[J]. World J Surg Oncol, 2014, 12: 365.
WANG S W, SUN M Y, ZHANG L N, et al. MR perfusion and diffusion imaging in diagnosing benign and malignant bone tumors[J]. International Journal of Medical Radiology, 2008, 31(1): 6-10.
HISATOMI M, ASAUMI J I, YANAGI Y, et al. Diagnostic value of dynamic contrast-enhanced MRI in the salivary gland tumors[J]. Oral Oncol, 2007, 43(9): 940-947.
ZHOU J Y, ZAISS M, KNUTSSON L, et al. Review and consensus recommendations on clinical APT-weighted imaging approaches at 3T: application to brain tumors[J]. Magn Reson Med, 2022, 88(2): 546-574.
GUO H, LIU J, HU J J, et al. Diagnostic performance of gliomas grading and IDH status decoding A comparison between 3D amide proton transfer APT and four diffusion-weighted MRI models[J]. J Magn Reson Imaging, 2022, 56(6): 1834-1844.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}