上海交通大学学报(医学版) ›› 2024, Vol. 44 ›› Issue (4): 482-493.doi: 10.3969/j.issn.1674-8115.2024.04.009
傅艺玲( ), 吴茜, 罗晓庆, 吴艾泓, 夏雪兰, 郑敏()
), 吴茜, 罗晓庆, 吴艾泓, 夏雪兰, 郑敏()
收稿日期:2023-11-01
接受日期:2024-02-06
出版日期:2024-04-28
发布日期:2024-04-28
通讯作者:
郑 敏(1979—),电子信箱:1287285766@qq.com。作者简介:傅艺玲(1999—),女,护士,硕士生;电子信箱:1715757154@qq.com。
FU Yiling(), WU Qian, LUO Xiaoqing, WU Aihong, XIA Xuelan, ZHENG Min()
Received:2023-11-01
Accepted:2024-02-06
Online:2024-04-28
Published:2024-04-28
Contact:
ZHENG Min, E-mail: 1287285766@qq.com.摘要:
目的·系统整合晚期癌症患者预立医疗照护计划(advance care planning,ACP)参与行为的相关影响因素。方法·系统检索中国知网、万方、中国生物医学文献数据库(Sinomed)、PubMed、Cochrane Library、Embase、CINAHL、PsycINFO等数据库从建库至2022年12月有关晚期癌症患者ACP参与行为影响因素的中英文文献。由2名研究者对最终纳入的文献进行文献质量评价、内容提取和汇总,将定量研究与定性研究分别提取数据后进行整合,得到晚期癌症患者ACP参与行为的最终影响因素。并借助理论域框架,将其逐级映射至能力、机会、动机-行为(capability, opportunity, motivation-behavior,COM-B)模型。结果·共纳入21项研究,整合归纳出27个影响因素,涉及9个理论域。映射至COM-B模型中的因素包括能力因素9个(ACP知识、文化程度、准确了解预后知识、知晓疾病诊断时间、先前经历、主观预期寿命、年龄、肿瘤部位、疾病症状负担)、机会因素13个(性别、婚姻状况、种族/民族、宗教信仰、未成年子女、家庭经济收入、居住地点、房屋居住类型、家庭支持、社会支持、医患关系、文化适应、是否设立临终关怀服务中心)和动机因素5个(ACP态度、ACP信念、ACP动机、焦虑抑郁、死亡态度)。其中,医患关系、宗教信仰、ACP态度、文化程度、婚姻状况、家庭支持、ACP知识、准确了解预后知识、年龄、居住地点、死亡态度、先前经历、种族/民族是对患者ACP参与行为影响较多的因素。结论·基于COM-B模型可全面归纳总结晚期癌症患者ACP参与行为的影响因素。未来研究可以上述因素为切入点,基于COM-B模型设计连续化、多方面的综合性干预措施,促进晚期癌症患者ACP参与行为实践。
中图分类号:
傅艺玲, 吴茜, 罗晓庆, 吴艾泓, 夏雪兰, 郑敏. 晚期癌症患者预立医疗照护计划参与行为影响因素的系统综述[J]. 上海交通大学学报(医学版), 2024, 44(4): 482-493.
FU Yiling, WU Qian, LUO Xiaoqing, WU Aihong, XIA Xuelan, ZHENG Min. Factors influencing advance care planning engagement behavior in patients with advanced cancer: a systematic review[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(4): 482-493.
| Step | Strategy |
|---|---|
| #1 | "advance care planning" [MeSH Terms] |
| #2 | "advance care planning" [Title/Abstract] OR "advance directives" [Title/Abstract] OR "living wills" [Title/Abstract]) OR "medical power of attorney" [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | "terminal" [Title/Abstract] OR "advanced" [Title/Abstract] OR "end-stage" [Title/Abstract] OR "end-of-life" [Title/Abstract] |
| #5 | "neoplasms" [MeSH Terms] |
| #6 | "neoplasms" [Title/Abstract] OR "cancer"[Title/Abstract] OR "tumor" [Title/Abstract] OR "oncology" [Title/Abstract] OR "malignancy" [Title/Abstract] |
| #7 | #5 OR #6 |
| #8 | #4 AND #7 |
| #9 | #3 AND #8 |
表1 PubMed 检索策略
Tab 1 Searching strategy for searching in PubMed
| Step | Strategy |
|---|---|
| #1 | "advance care planning" [MeSH Terms] |
| #2 | "advance care planning" [Title/Abstract] OR "advance directives" [Title/Abstract] OR "living wills" [Title/Abstract]) OR "medical power of attorney" [Title/Abstract] |
| #3 | #1 OR #2 |
| #4 | "terminal" [Title/Abstract] OR "advanced" [Title/Abstract] OR "end-stage" [Title/Abstract] OR "end-of-life" [Title/Abstract] |
| #5 | "neoplasms" [MeSH Terms] |
| #6 | "neoplasms" [Title/Abstract] OR "cancer"[Title/Abstract] OR "tumor" [Title/Abstract] OR "oncology" [Title/Abstract] OR "malignancy" [Title/Abstract] |
| #7 | #5 OR #6 |
| #8 | #4 AND #7 |
| #9 | #3 AND #8 |
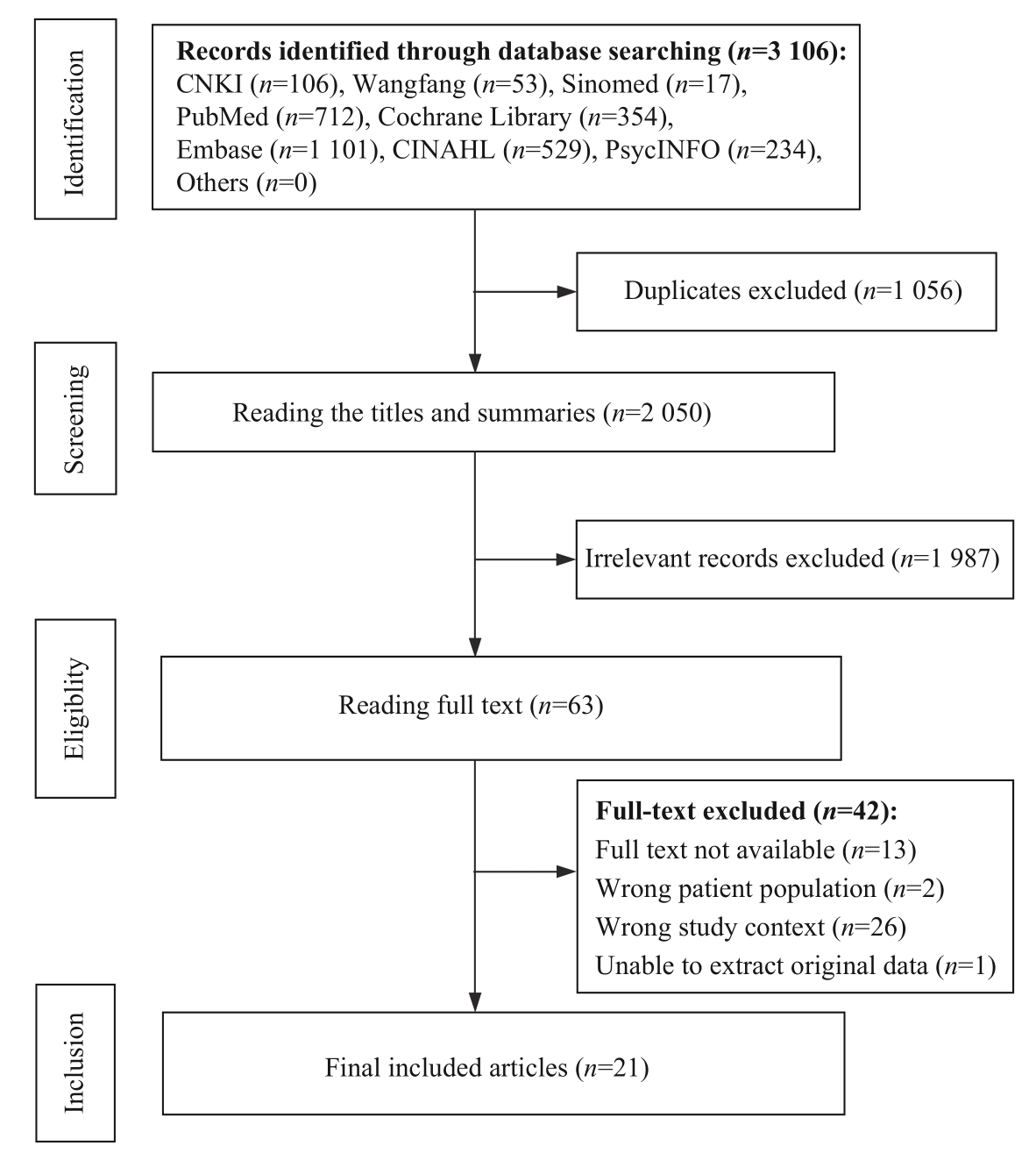
图1 文献筛选流程
Fig 1 Process of study selection
| Author | Year | Area | Design | Research method | Sample size | Influencing factor | Quality rating |
|---|---|---|---|---|---|---|---|
| QU X L, et al | 2020 | Beijing, China | Qualitative study | Phenomenological study | 17 | Ⅰ: ①② | 80% |
| BAR-SELA G, et al | 2021 | Israel | Mixed studies | Phenomenological study Questionnaire investigation | 109 | Ⅰ: ①②⑧⑨⑩⑪ Ⅱ: ⑥⑦ | QN: 73% QL: 80% |
| WANG Y X, et al | 2019 | Hefei, China | Cross-sectional study | Questionnaire investigation | 520 | Ⅰ: ⑧⑨ Ⅱ: ④⑤⑥⑦⑫ ⑭⑮ | 64% |
| WANG L, et al | 2021 | Xi'an, China | Cross-sectional study | Questionnaire investigation | 72 | Ⅱ: ③⑤⑭⑯17 Ⅲ: 18 | 91% |
| YAN C X, et al | 2022 | Tianjin, China | Cross-sectional study | Questionnaire investigation | 206 | Ⅰ: ① Ⅲ: ②④⑭ | 86% |
| CHEN Y Z, et al | 2022 | Guangzhou, China | Cross-sectional study | Questionnaire investigation | 120 | Ⅲ: ③④⑪19 | 86% |
| TANG S T, et al | 2014 | Taiwan, China | Cross-sectional study | Questionnaire investigation | 2 450 | Ⅲ: ⑭2021 | 86% |
| WONG S Y, et al | 2012 | Hong Kong, China | Cohort study | Questionnaire investigation | 191 | Ⅲ: 20 Ⅳ: ⑩ | 77% |
| HOU X T, et al | 2021 | Beijing, China | Cross-sectional study | Questionnaire investigation | 264 | Ⅲ: ⑤⑥⑫⑬ | 73% |
| KIERNER K A, et al | 2010 | Austria | Cohort study | Questionnaire investigation | 108 | Ⅱ: 22 | 64% |
| RODENBACH R A, et al | 2021 | America | Cross-sectional study | Questionnaire investigation | 672 | Ⅲ: 19 | 86% |
| GARRIDO M M, et al | 2014 | America | Cross-sectional study | Questionnaire investigation | 606 | Ⅲ: 23 | 82% |
| NILSSON M E, et al | 2009 | America | Cohort study | Questionnaire investigation | 668 | Ⅲ: 24 | 86% |
| TRUE G, et al | 2005 | America | Longitudinal study | Questionnaire investigation | 68 | Ⅲ: ④23 | 73% |
| YOO S H, et al | 2020 | South Korea | Cohort study | Questionnaire investigation | 150 | Ⅰ: 25 Ⅳ: 20 | 86% |
| BROWN A J, et al | 2016 | America | Cross-sectional study | Questionnaire investigation | 110 | Ⅲ: ③⑥1926 | 77% |
| ZHU M L, et al | 2019 | Zunyi, China | Cross-sectional study | Questionnaire investigation | 90 | Ⅱ: ③⑯ | 59% |
| WANG Y L | 2021 | Shandong, China | Cross-sectional study | Questionnaire investigation | 145 | Ⅲ: ⑬⑭19 | 91% |
| SHEN M J, et al | 2018 | America | Cohort study | Questionnaire investigation | 279 | Ⅲ: 20 | 77% |
| SHEN M J, et al | 2020 | America | Qualitative study | Phenomenological study | 20 | Ⅰ: ④⑩⑪1823 | 55% |
| JIA Z M, et al | 2022 | America | Qualitative study | Phenomenological study | 21 | Ⅰ: ②⑪27 | 90% |
表2 纳入文献的基本特征
Tab 2 Characteristics of the included literature
| Author | Year | Area | Design | Research method | Sample size | Influencing factor | Quality rating |
|---|---|---|---|---|---|---|---|
| QU X L, et al | 2020 | Beijing, China | Qualitative study | Phenomenological study | 17 | Ⅰ: ①② | 80% |
| BAR-SELA G, et al | 2021 | Israel | Mixed studies | Phenomenological study Questionnaire investigation | 109 | Ⅰ: ①②⑧⑨⑩⑪ Ⅱ: ⑥⑦ | QN: 73% QL: 80% |
| WANG Y X, et al | 2019 | Hefei, China | Cross-sectional study | Questionnaire investigation | 520 | Ⅰ: ⑧⑨ Ⅱ: ④⑤⑥⑦⑫ ⑭⑮ | 64% |
| WANG L, et al | 2021 | Xi'an, China | Cross-sectional study | Questionnaire investigation | 72 | Ⅱ: ③⑤⑭⑯17 Ⅲ: 18 | 91% |
| YAN C X, et al | 2022 | Tianjin, China | Cross-sectional study | Questionnaire investigation | 206 | Ⅰ: ① Ⅲ: ②④⑭ | 86% |
| CHEN Y Z, et al | 2022 | Guangzhou, China | Cross-sectional study | Questionnaire investigation | 120 | Ⅲ: ③④⑪19 | 86% |
| TANG S T, et al | 2014 | Taiwan, China | Cross-sectional study | Questionnaire investigation | 2 450 | Ⅲ: ⑭2021 | 86% |
| WONG S Y, et al | 2012 | Hong Kong, China | Cohort study | Questionnaire investigation | 191 | Ⅲ: 20 Ⅳ: ⑩ | 77% |
| HOU X T, et al | 2021 | Beijing, China | Cross-sectional study | Questionnaire investigation | 264 | Ⅲ: ⑤⑥⑫⑬ | 73% |
| KIERNER K A, et al | 2010 | Austria | Cohort study | Questionnaire investigation | 108 | Ⅱ: 22 | 64% |
| RODENBACH R A, et al | 2021 | America | Cross-sectional study | Questionnaire investigation | 672 | Ⅲ: 19 | 86% |
| GARRIDO M M, et al | 2014 | America | Cross-sectional study | Questionnaire investigation | 606 | Ⅲ: 23 | 82% |
| NILSSON M E, et al | 2009 | America | Cohort study | Questionnaire investigation | 668 | Ⅲ: 24 | 86% |
| TRUE G, et al | 2005 | America | Longitudinal study | Questionnaire investigation | 68 | Ⅲ: ④23 | 73% |
| YOO S H, et al | 2020 | South Korea | Cohort study | Questionnaire investigation | 150 | Ⅰ: 25 Ⅳ: 20 | 86% |
| BROWN A J, et al | 2016 | America | Cross-sectional study | Questionnaire investigation | 110 | Ⅲ: ③⑥1926 | 77% |
| ZHU M L, et al | 2019 | Zunyi, China | Cross-sectional study | Questionnaire investigation | 90 | Ⅱ: ③⑯ | 59% |
| WANG Y L | 2021 | Shandong, China | Cross-sectional study | Questionnaire investigation | 145 | Ⅲ: ⑬⑭19 | 91% |
| SHEN M J, et al | 2018 | America | Cohort study | Questionnaire investigation | 279 | Ⅲ: 20 | 77% |
| SHEN M J, et al | 2020 | America | Qualitative study | Phenomenological study | 20 | Ⅰ: ④⑩⑪1823 | 55% |
| JIA Z M, et al | 2022 | America | Qualitative study | Phenomenological study | 21 | Ⅰ: ②⑪27 | 90% |
COM-B component | TDF | Original definition | Application of TDF to the connotation of ACP engagement behavior in patients with advanced cancer |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | An awareness of the existence of something | Understanding and being familiar with ACP-related knowledge |
| Memory, attention and decision processes | The ability to retain information, selectively focus on aspects of the environment and choose between two or more alternatives | Ability to remember, focus, and select ACP | |
| Behavioural regulation | Anything aiming at managing or changing objectively observed or measured actions | Using healthy behaviors to manage emotions and pursue goals | |
| Physical capability | Skills | An ability or proficiency acquired through practice | Acquiring the ability or skill to engage in ACP through practice, including physiological and cognitive skills |
| Opportunity | |||
| Social opportunity | Social influences | Those interpersonal processes that can cause individuals to change their thoughts, feelings, or behaviors | The process of social activities that enable individuals to change their cognition and behavior about ACP |
| Physical opportunity | Environmental context and resources | Any circumstance of a person's situation or environment that discourages or encourages the development of skills and abilities, independence, social competence, and adaptive behavior | Personal conditions and environments that influence ACP engagement |
| Motivation | |||
| Reflective motivation | Beliefs about capabilities | Acceptance of the truth, reality, or validity about an ability, talent, or facility that a person can put to constructive use | Believing that individuals have enough knowledge about ACP and can participate in ACP discussions |
| Goals | Mental representations of outcomes or end states that an individual wants to achieve | The psychological outcomes that individuals want to achieve | |
| Intentions | A conscious decision to perform a behavior or a resolve to act in a certain way | Identifying the skills that are needed to engage in ACP | |
| Beliefs about consequences | Acceptance of the truth, reality, or validity about outcomes of a behavior in a given situation | The degree to which the individuals accept the facts or believe that ACP's involvement in the behavior will lead to specific results | |
| Automatic motivation | Social/professional role and identity | A coherent set of behaviors and displayed personal qualities of an individual in a social or work setting | Self-perception based on social or professional identity |
| Optimism | The confidence that things will happen for the best or that desired goals will be attained | Confidence that the desired goal will be achieved | |
| Reinforcement | Increasing the probability of a response by arranging a dependent relationship, or contingency, between the response and a given stimulus | Promoting and strengthening support for ACP participation | |
| Emotion | A complex reaction pattern, involving experiential, behavioural, and physiological elements, by which the individual attempts to deal with a personally significant matter or event | A mental state or emotional response that is determined by an individual's environment |
表3 COM-B模型应用于晚期癌症患者ACP参与行为的内涵
Tab 3 Connotation of the COM-B model in the ACP engagement behavior of advanced cancer patients
COM-B component | TDF | Original definition | Application of TDF to the connotation of ACP engagement behavior in patients with advanced cancer |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | An awareness of the existence of something | Understanding and being familiar with ACP-related knowledge |
| Memory, attention and decision processes | The ability to retain information, selectively focus on aspects of the environment and choose between two or more alternatives | Ability to remember, focus, and select ACP | |
| Behavioural regulation | Anything aiming at managing or changing objectively observed or measured actions | Using healthy behaviors to manage emotions and pursue goals | |
| Physical capability | Skills | An ability or proficiency acquired through practice | Acquiring the ability or skill to engage in ACP through practice, including physiological and cognitive skills |
| Opportunity | |||
| Social opportunity | Social influences | Those interpersonal processes that can cause individuals to change their thoughts, feelings, or behaviors | The process of social activities that enable individuals to change their cognition and behavior about ACP |
| Physical opportunity | Environmental context and resources | Any circumstance of a person's situation or environment that discourages or encourages the development of skills and abilities, independence, social competence, and adaptive behavior | Personal conditions and environments that influence ACP engagement |
| Motivation | |||
| Reflective motivation | Beliefs about capabilities | Acceptance of the truth, reality, or validity about an ability, talent, or facility that a person can put to constructive use | Believing that individuals have enough knowledge about ACP and can participate in ACP discussions |
| Goals | Mental representations of outcomes or end states that an individual wants to achieve | The psychological outcomes that individuals want to achieve | |
| Intentions | A conscious decision to perform a behavior or a resolve to act in a certain way | Identifying the skills that are needed to engage in ACP | |
| Beliefs about consequences | Acceptance of the truth, reality, or validity about outcomes of a behavior in a given situation | The degree to which the individuals accept the facts or believe that ACP's involvement in the behavior will lead to specific results | |
| Automatic motivation | Social/professional role and identity | A coherent set of behaviors and displayed personal qualities of an individual in a social or work setting | Self-perception based on social or professional identity |
| Optimism | The confidence that things will happen for the best or that desired goals will be attained | Confidence that the desired goal will be achieved | |
| Reinforcement | Increasing the probability of a response by arranging a dependent relationship, or contingency, between the response and a given stimulus | Promoting and strengthening support for ACP participation | |
| Emotion | A complex reaction pattern, involving experiential, behavioural, and physiological elements, by which the individual attempts to deal with a personally significant matter or event | A mental state or emotional response that is determined by an individual's environment |
| COM-B | TDF | Influencing factor | Specific description |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP | →Getting more information about ACP can help patients to understand its significance[ →Patients do not know, do not understand or misunderstand the related concepts of ACP[ |
| Education level | →Cultural education can help patients engage in discussion APC[ | ||
| Behavioural regulation | Prior experience | →Patients with disease experience are more likely to discuss ACP[ | |
| Physical capability | Skills | Cancer site | →Lung cancer patients are more likely to complete advanced directives/Durable Power of Attorney (DPOA) than brain cancer patients[ |
| Opportunity | |||
| Social opportunity | Social influences | Race/ethnicity | →Hispanic patients prefer a family-centered, physician-informed approach to discussing ACP with consideration and incorporation of their religious medical beliefs about end-of-life care[ |
| Religious belief | →Overly optimistic religious beliefs will affect patients' discussion about ACP[ | ||
| Family support | →Patients hope to have open communication with family members[ →Involving family in conversations about end-of-life care can help Latinos to communicate[ →No close relatives agree to take responsibility for preventing patients from engaging in ACP[ →No close relatives can be trusted for preventing patients from engaging in ACP[ | ||
| Doctor-patient relationship | →Patients prefer for the trusted doctors to initiate ACP conversations[ →Patients hope to have open communication with physician[ →Patients' preconceived notions of clinicians' professional responsibility may hinder public discussion of future health care goals and values[ | ||
| Social support | →Providing culturally counseling services and educational materials can help patients learn how to communicate information about ACP[ | ||
| Acculturation | →A key regulator of how patients view ACP is their cultural adaptation to local norms of care, behavior, and communication[ | ||
| Physical opportunity | Environmental context and resources | Place of living | →Living in rural areas has a positive impact on patients' willingness to participate in ACP[ |
| Motivation | |||
| Reflective motivation | Intentions | ACP attitude | →Uncertainty about the timing of patients' engagement in ACP[ →Patients believe that engagement in ACP increases negative emotions[ →Patients question whether ACP itself can be carried out smoothly[ →Patients' belief in an uncertain future may hinder public discussion of future health care goals and values[ |
| Goals | ACP belief | →Patients hope to make the best medical decisions and avoid unnecessary medical measures[ | |
| Beliefs about capabilities | ACP motivation | →Having the opportunity to discuss disease information openly with families and doctors will increase patients' willingness to engage in ACP[ |
表4 定性研究影响因素的整合结果
Tab 4 Integration results of qualitative study of influencing factors
| COM-B | TDF | Influencing factor | Specific description |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP | →Getting more information about ACP can help patients to understand its significance[ →Patients do not know, do not understand or misunderstand the related concepts of ACP[ |
| Education level | →Cultural education can help patients engage in discussion APC[ | ||
| Behavioural regulation | Prior experience | →Patients with disease experience are more likely to discuss ACP[ | |
| Physical capability | Skills | Cancer site | →Lung cancer patients are more likely to complete advanced directives/Durable Power of Attorney (DPOA) than brain cancer patients[ |
| Opportunity | |||
| Social opportunity | Social influences | Race/ethnicity | →Hispanic patients prefer a family-centered, physician-informed approach to discussing ACP with consideration and incorporation of their religious medical beliefs about end-of-life care[ |
| Religious belief | →Overly optimistic religious beliefs will affect patients' discussion about ACP[ | ||
| Family support | →Patients hope to have open communication with family members[ →Involving family in conversations about end-of-life care can help Latinos to communicate[ →No close relatives agree to take responsibility for preventing patients from engaging in ACP[ →No close relatives can be trusted for preventing patients from engaging in ACP[ | ||
| Doctor-patient relationship | →Patients prefer for the trusted doctors to initiate ACP conversations[ →Patients hope to have open communication with physician[ →Patients' preconceived notions of clinicians' professional responsibility may hinder public discussion of future health care goals and values[ | ||
| Social support | →Providing culturally counseling services and educational materials can help patients learn how to communicate information about ACP[ | ||
| Acculturation | →A key regulator of how patients view ACP is their cultural adaptation to local norms of care, behavior, and communication[ | ||
| Physical opportunity | Environmental context and resources | Place of living | →Living in rural areas has a positive impact on patients' willingness to participate in ACP[ |
| Motivation | |||
| Reflective motivation | Intentions | ACP attitude | →Uncertainty about the timing of patients' engagement in ACP[ →Patients believe that engagement in ACP increases negative emotions[ →Patients question whether ACP itself can be carried out smoothly[ →Patients' belief in an uncertain future may hinder public discussion of future health care goals and values[ |
| Goals | ACP belief | →Patients hope to make the best medical decisions and avoid unnecessary medical measures[ | |
| Beliefs about capabilities | ACP motivation | →Having the opportunity to discuss disease information openly with families and doctors will increase patients' willingness to engage in ACP[ |
| COM-B | TDF | Influencing factor | Specific description |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP | →The percentage of patients willing to engage in ACP increased after understanding the concept, process, and importance of advance directive[ |
| Behavioural regulation | Knowledge of the time of disease diagnosis | →Patients who know about the diagnosis of the disease for longer are more likely to engage in ACP[ | |
| Subjective life expectancy | →Patients who are expected to live only a few months are less likely to prefer aggressive treatment[ | ||
| Physical capability | Skills | Disease symptom burden | →The greater the burden of symptoms, the less likely patients are to sign advance directives or health care powers of attorney[ |
| Opportunity | |||
| Social opportunity | Social influences | Family support | →Family members not objecting is an important factor in discussing ACP[ |
| Social support | →Patients with higher social support are more willing to engage in ACP[ | ||
| Doctor-patient relationship | →Poor doctor-patient relationship leads to low acceptance of ACP[ | ||
| Dependent children | →Patients with dependent children are more likely to prefer aggressive treatment and less likely to engage in ACP[ | ||
| Physical opportunity | Environmental context and resources | Housing type | →Patients without private housing are more willing to engage in ACP[ |
| Hospice service center | →Whether or not to establish a hospice service center is a factor influencing whether or not patients choose to participate in ACP[ | ||
| Motivation | |||
| Reflective motivation | Intentions | ACP attitude | →The sense of life meaning is the main factor influencing patients' attitude towards ACP[ |
| Goals | ACP belief | →Patients want to ensure a comfortable end-of-life and avoid pain[ | |
| Beliefs about capabilities | ACP motivation | →The reason that hinders patients from engaging in ACP is that patients think that their relatives can make decisions for them or that their wishes may change in the future[ | |
| Automatic motivation | Emotion | Anxiety and depression | →Patients who participated in ACP had significantly higher anxiety and depression scores than those who did not participate in ACP[ |
表5 定量研究描述性分析结果
Tab 5 Descriptive analysis results of quantitative study
| COM-B | TDF | Influencing factor | Specific description |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP | →The percentage of patients willing to engage in ACP increased after understanding the concept, process, and importance of advance directive[ |
| Behavioural regulation | Knowledge of the time of disease diagnosis | →Patients who know about the diagnosis of the disease for longer are more likely to engage in ACP[ | |
| Subjective life expectancy | →Patients who are expected to live only a few months are less likely to prefer aggressive treatment[ | ||
| Physical capability | Skills | Disease symptom burden | →The greater the burden of symptoms, the less likely patients are to sign advance directives or health care powers of attorney[ |
| Opportunity | |||
| Social opportunity | Social influences | Family support | →Family members not objecting is an important factor in discussing ACP[ |
| Social support | →Patients with higher social support are more willing to engage in ACP[ | ||
| Doctor-patient relationship | →Poor doctor-patient relationship leads to low acceptance of ACP[ | ||
| Dependent children | →Patients with dependent children are more likely to prefer aggressive treatment and less likely to engage in ACP[ | ||
| Physical opportunity | Environmental context and resources | Housing type | →Patients without private housing are more willing to engage in ACP[ |
| Hospice service center | →Whether or not to establish a hospice service center is a factor influencing whether or not patients choose to participate in ACP[ | ||
| Motivation | |||
| Reflective motivation | Intentions | ACP attitude | →The sense of life meaning is the main factor influencing patients' attitude towards ACP[ |
| Goals | ACP belief | →Patients want to ensure a comfortable end-of-life and avoid pain[ | |
| Beliefs about capabilities | ACP motivation | →The reason that hinders patients from engaging in ACP is that patients think that their relatives can make decisions for them or that their wishes may change in the future[ | |
| Automatic motivation | Emotion | Anxiety and depression | →Patients who participated in ACP had significantly higher anxiety and depression scores than those who did not participate in ACP[ |
| COM-B | TDF | Facilitator | Barrier |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP[ Education level[ Accurate knowledge of prognosis[ | Knowledge of ACP[ |
| Behavioural regulation | Knowledge of the time of disease diagnosis[ Prior experience[ | Subjective life expectancy[ | |
| Physical capability | Skills | Age[ Cancer site[ | Disease symptom burden[ |
| Opportunity | |||
| Social opportunity | Social influences | Marital status[ Race/ethnicity[ Family support[ Doctor-patient relationship[ Religious belief[ Gender[ Social support[ Dependent children[ Acculturation[ | Marital status[ Race/ethnicity[ Family support[ Doctor-patient relationship[ Religious belief[ |
| Physical opportunity | Environmental context and resources | Family economic condition[ Place of living[ Housing type[ | Hospice service center[ Place of living[ |
| Motivation | |||
| Reflective motivation | Intentions | ‒ | ACP attitude[ |
| Goals | ACP belief[ | ‒ | |
| Beliefs about capabilities | ACP motivation[ | ACP motivation[ | |
| Automatic motivation | Emotion | Anxiety and depression[ | Death attitude[ |
表6 晚期癌症患者ACP参与行为影响因素COM-B模型编码结果汇总
Tab 6 Factors influencing ACP engagement behavior of advanced cancer patients coded according to COM-B model
| COM-B | TDF | Facilitator | Barrier |
|---|---|---|---|
| Capability | |||
| Psychological capability | Knowledge | Knowledge of ACP[ Education level[ Accurate knowledge of prognosis[ | Knowledge of ACP[ |
| Behavioural regulation | Knowledge of the time of disease diagnosis[ Prior experience[ | Subjective life expectancy[ | |
| Physical capability | Skills | Age[ Cancer site[ | Disease symptom burden[ |
| Opportunity | |||
| Social opportunity | Social influences | Marital status[ Race/ethnicity[ Family support[ Doctor-patient relationship[ Religious belief[ Gender[ Social support[ Dependent children[ Acculturation[ | Marital status[ Race/ethnicity[ Family support[ Doctor-patient relationship[ Religious belief[ |
| Physical opportunity | Environmental context and resources | Family economic condition[ Place of living[ Housing type[ | Hospice service center[ Place of living[ |
| Motivation | |||
| Reflective motivation | Intentions | ‒ | ACP attitude[ |
| Goals | ACP belief[ | ‒ | |
| Beliefs about capabilities | ACP motivation[ | ACP motivation[ | |
| Automatic motivation | Emotion | Anxiety and depression[ | Death attitude[ |
| 1 | SUNG H, FERLAY J, SIEGEL R L, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. |
| 2 | COSTA A R, LUNET N, MARTINS-BRANCO D, et al. Hospitalizations at the end of life among chronic obstructive pulmonary disease and lung cancer patients: a nationwide study[J]. J Pain Symptom Manage, 2021, 62(1): 48-57. |
| 3 | 龚婷. 基于预立医疗照护计划癌症患者决策辅助工具的原型设计研究[D]. 成都: 成都医学院, 2023. |
| GONG T. Prototyping study of decision aid tools for cancer patients based on advance care planning[D]. Chengdu: Chengdu Medical College, 2023. | |
| 4 | LIN C P, EVANS C J, KOFFMAN J, et al. The conceptual models and mechanisms of action that underpin advance care planning for cancer patients: a systematic review of randomised controlled trials[J]. Palliat Med, 2019, 33(1): 5-23. |
| 5 | 李嘉音. 预立医疗照护计划参与问卷汉化及在社区老年慢病患者中的应用研究[D]. 郑州: 郑州大学, 2021. |
| LI J Y. The Chinese localization of Advance Care Planning Engagement Survey and the application in community elderly chronic patients[D]. Zhengzhou: Zhengzhou University, 2021. | |
| 6 | DUNCAN E, O'CATHAIN A, ROUSSEAU N, et al. Guidance for reporting intervention development studies in health research (GUIDED): an evidence-based consensus study[J]. BMJ Open, 2020, 10(4): e033516. |
| 7 | MICHIE S, van STRALEN M M, WEST R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions[J]. Implement Sci, 2011, 6: 42. |
| 8 | ATKINS L, FRANCIS J, ISLAM R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems[J]. Implement Sci, 2017, 12: 77. |
| 9 | 郭慧琦, 沈蕴之, 施海明, 等. 医护人员心脏康复推荐决策行为的障碍因素分析: 基于能力、机会、动机-行动模型和理论域框架的质性研究[J]. 军事护理, 2023, 40(12): 60-63. |
| GUO H Q, SHEN Y Z, SHI H M, et al. Analysis of obstacles to decision-making behavior cardiac rehabilitation recommendation among medical staff: a qualitative study based on COM-B Model and Theoretical Domain Framework[J]. Military Nursing, 2023, 40(12): 60-63. | |
| 10 | 董安红. 基于COM-B模型的类风湿关节炎患者服药依从性阻碍与促进因素研究[D]. 武汉: 华中科技大学, 2021. |
| DONG A H. Barriers and enablers to medication adherence of patients with rheumatoid arthritis based on COM-B model[D]. Wuhan: Huazhong University of Science and Technology, 2021. | |
| 11 | 仇如霞, 顾艳荭. 范围综述报告规范(PRISMA-ScR)的解读[J]. 中国循证医学杂志, 2022, 22(6): 722-730. |
| QIU R X, GU Y H. Interpretation of the PRISMA extension for scoping review (PRISMA-ScR)[J]. Chinese Journal of Evidence-Based Medicine, 2022, 22(6): 722-730. | |
| 12 | KISHINO M, ELLIS-SMITH C, AFOLABI O, et al. Family involvement in advance care planning for people living with advanced cancer: a systematic mixed-methods review[J]. Palliat Med, 2022, 36(3): 462-477. |
| 13 | MICHIE S, JOHNSTON M, ABRAHAM C, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach[J]. Qual Saf Health Care, 2005, 14(1): 26-33. |
| 14 | 邱均平, 邹菲. 关于内容分析法的研究[J]. 中国图书馆学报, 2004, 30(2): 12-17. |
| QIU J P, ZOU F. A study of content analysis methods[J]. Journal of Library Science in China, 2004, 30(2): 12-17. | |
| 15 | 陈颖珍, 邬丽满, 李红霞, 等. 晚期癌症患者预立医疗照护计划接受现状及影响因素分析[J]. 护理实践与研究, 2022, 19(21): 3192-3197. |
| CHEN Y Z, WU L M, LI H X, et al. Statue quo and influencing factors of advance care plan acceptance in advanced cancer patients[J]. Nursing Practice and Research, 2022, 19(21): 3192-3197. | |
| 16 | 闫春旭, 张倩, 武文婧, 等. 老年晚期肿瘤患者预先指示态度的调查研究[J]. 军事护理, 2022, 39(8): 69-72. |
| YAN C X, ZHANG Q, WU W J, et al. Survey on the attitudes to advance directives in elderly patients with advanced cancer[J]. Military Nursing, 2022, 39(8): 69-72. | |
| 17 | 王雅莉. 肺癌患者及照护者对“预立医疗照护计划”认知影响因素的二元关系模型构建[D]. 济南: 山东大学, 2021. |
| WANG Y L. Construction of the dyadic relationship model for influencing factors of perception to "advance care planning" among lung cancer patients and caregivers[D]. Jinan: Shandong University, 2021. | |
| 18 | 王力, 赵芳, 李小宁, 等. 晚期乳腺肿瘤患者对预立医疗照护计划的接受程度及影响因素分析[J]. 中华现代护理杂志, 2021, 27(34): 4694-4699. |
| WANG L, ZHAO F, LI X N, et al. Acceptance of advanced breast cancer patients to the advance care planning and its influencing factors[J]. Chinese Journal of Modern Nursing, 2021, 27(34): 4694-4699. | |
| 19 | 屈小伶, 张炜, 张晓颖, 等. 终末期肺癌患者预立医疗照护计划的认知和态度的质性研究[J]. 中华现代护理杂志, 2020, 26(35): 4944-4948. |
| QU X L, ZHANG W, ZHANG X Y, et al. Qualitative research on cognition and attitude of patients with end-stage lung cancer towards advance care planning[J]. Chinese Journal of Modern Nursing, 2020, 26(35): 4944-4948. | |
| 20 | 王毅欣, 王秀敏, 焦丽, 等. 晚期肿瘤患者对生前预嘱及临终关怀的认知及影响因素研究[J]. 医学与哲学, 2019, 40(5): 30-34. |
| WANG Y X, WANG X M, JIAO L, et al. Cognition and the influencing factors of advance directives and end-of-life care of patients with advanced tumors[J]. Medicine & Philosophy, 2019, 40(5): 30-34. | |
| 21 | 朱明兰, 蒋本利, 崔伟, 等. 终末期恶性肿瘤患者及家属对预先指示认知的现况调查[J]. 长治医学院学报, 2019, 33(1): 19-22. |
| ZHU M L, JIANG B L, CUI W, et al. Investigation and analysis of pre-indicated cognition status of patients with end-stage maglignant tumor and their families[J]. Journal of Changzhi Medical College, 2019, 33(1): 19-22. | |
| 22 | JIA Z M, YEH I M, LEE C H, et al. Barriers and facilitators to advance care planning among Chinese patients with advanced cancer and their caregivers[J]. J Palliat Med, 2022, 25(5): 774-782. |
| 23 | BAR-SELA G, BAGON S, MITNIK I, et al. The perception and attitudes of Israeli cancer patients regarding advance care planning[J]. J Geriatr Oncol, 2021, 12(8): 1181-1185. |
| 24 | HOU X T, LU Y H, YANG H, et al. The knowledge and attitude towards advance care planning among Chinese patients with advanced cancer[J]. J Cancer Educ, 2021, 36(3): 603-610. |
| 25 | RODENBACH R A, ALTHOUSE A D, SCHENKER Y, et al. Relationships between advanced cancer patients' worry about dying and illness understanding, treatment preferences, and advance care planning[J]. J Pain Symptom Manage, 2021, 61(4): 723-731.e1. |
| 26 | SHEN M J, GONZALEZ C, LEACH B, et al. An examination of Latino advanced cancer patients' and their informal caregivers' preferences for communication about advance care planning: a qualitative study[J]. Palliat Support Care, 2020, 18(3): 277-284. |
| 27 | YOO S H, LEE J, KANG J H, et al. Association of illness understanding with advance care planning and end-of-life care preferences for advanced cancer patients and their family members[J]. Support Care Cancer, 2020, 28(6): 2959-2967. |
| 28 | SHEN M J, TREVINO K M, PRIGERSON H G. The interactive effect of advanced cancer patient and caregiver prognostic understanding on patients' completion of Do Not Resuscitate orders[J]. Psycho-oncology, 2018, 27(7): 1765-1771. |
| 29 | BROWN A J, SHEN M J, URBAUER D, et al. Room for improvement: an examination of advance care planning documentation among gynecologic oncology patients[J]. Gynecol Oncol, 2016, 142(3): 525-530. |
| 30 | TANG S T, LIU T W, LIU L N, et al. Physician-patient end-of-life care discussions: correlates and associations with end-of-life care preferences of cancer patients: a cross-sectional survey study[J]. Palliat Med, 2014, 28(10): 1222-1230. |
| 31 | GARRIDO M M, HARRINGTON S T, PRIGERSON H G. End-of-life treatment preferences: a key to reducing ethnic/racial disparities in advance care planning?[J]. Cancer, 2014, 120(24): 3981-3986. |
| 32 | WONG S Y, LO S H, CHAN C H, et al. Is it feasible to discuss an advance directive with a Chinese patient with advanced malignancy? A prospective cohort study[J]. Hong Kong Med J, 2012, 18(3): 178-185. |
| 33 | KIERNER K A, HLADSCHIK-KERMER B, GARTNER V, et al. Attitudes of patients with malignancies towards completion of advance directives[J]. Support Care Cancer, 2010, 18(3): 367-372. |
| 34 | NILSSON M E, MACIEJEWSKI P K, ZHANG B H, et al. Mental health, treatment preferences, advance care planning, location, and quality of death in advanced cancer patients with dependent children[J]. Cancer, 2009, 115(2): 399-409. |
| 35 | TRUE G, PHIPPS E J, BRAITMAN L E, et al. Treatment preferences and advance care planning at end of life: the role of ethnicity and spiritual coping in cancer patients[J]. Ann Behav Med, 2005, 30(2): 174-179. |
| 36 | 邢淑君, 陈鹤方, 胡梦蝶, 等. 肿瘤患者参与药物临床试验现状及影响因素研究[J]. 中国新药杂志, 2022, 31(12): 1201-1208. |
| XING S J, CHEN H F, HU M D, et al. Study on the current situation and influencing factors of tumor patients participating in drug clincal trials[J]. Chinese Journal of New Drugs, 2022, 31(12): 1201-1208. | |
| 37 | 尹晓彤, 朱蓝玉, 王幽, 等. 中青年癌症患者预立医疗照护计划接受度现状及影响因素研究[J]. 中华护理杂志, 2022, 57(7): 834-840. |
| YIN X T, ZHU L Y, WANG Y, et al. Status quo and influencing factors of acceptance of advance care planning for young and middle-aged cancer patients[J]. Chinese Journal of Nursing, 2022, 57(7): 834-840. | |
| 38 | 缪佳芮, 陈柳柳, 张江辉, 等. 晚期癌症患者预立医疗照护计划质性研究进展[J]. 医学与哲学(B), 2018, 39(1): 61-64. |
| MIAO J R, CHEN L L, ZHANG J H, et al. Advances on qualitative research about advance care planning in patients with advanced cancer[J]. Medicine & Philosophy(B), 2018, 39(1): 61-64. | |
| 39 | 宫伟利, 赵涓旭, 韩玉香, 等. 基于跨理论模型的预立医疗照护计划干预在晚期癌症患者中的应用效果研究[J]. 军事护理, 2023, 40(8): 14-17. |
| GONG W L, ZHAO J X, HAN Y X, et al. Application effect of advanced care planning intervention on patients with advanced cancer based on cross-thoretical model[J]. Military Nursing, 2023, 40(8): 14-17. | |
| 40 | FESTINGER L. A theory of cognitive dissonance[M]. Stanford: Stanford University Press, 1962. |
| 41 | 周佳. 癌症患者死亡威胁及其防御机制研究[D]. 重庆: 西南大学, 2019. |
| ZHOU J. Research on death threat and defense mechanisms of cancer patients[D]. Chongqing: Southwest University, 2019. |
| [1] | 陆晔峰, 高磊青, 倪晓筱, 富晶晶. 儿童肝移植术后早期血糖及血脂的多时间点监测与影响因素分析[J]. 上海交通大学学报(医学版), 2025, 45(4): 443-451. |
| [2] | 陈佳莹, 褚以忞, 彭海霞. 结直肠癌无进展生存时间预测模型及影响因素研究[J]. 上海交通大学学报(医学版), 2025, 45(3): 324-334. |
| [3] | 陈丽红, 王妍, 周翔天, 郑俊克, 闫小响. 国家自然科学基金青年科学基金项目立项的影响因素分析——以上海交通大学医学院为例[J]. 上海交通大学学报(医学版), 2024, 44(9): 1205-1212. |
| [4] | 张勇, 李伟宏, 程志鹏, 王斌, 王思珩, 王毓斌. 受体相互作用蛋白激酶1调节癌症进展和免疫反应的研究现状[J]. 上海交通大学学报(医学版), 2024, 44(6): 788-794. |
| [5] | 孙晨寅, 吴百川, 张慧凤, 方贻儒, 彭代辉. 体动记录仪评估抑郁症昼夜节律:一项系统综述和meta分析[J]. 上海交通大学学报(医学版), 2024, 44(5): 606-616. |
| [6] | 高怡青, 彭裕, 许华俊, 易红良, 关建, 殷善开. 全球阻塞性睡眠呼吸暂停指南质量评价[J]. 上海交通大学学报(医学版), 2024, 44(2): 237-249. |
| [7] | 克德尔亚·艾山江, 傅怡, 赖冬林, 邬海龙, 龚伟. 肝细胞癌相关的核编码线粒体基因及临床信息的综合预后模型[J]. 上海交通大学学报(医学版), 2024, 44(1): 1-12. |
| [8] | 罗晨, 沈玲, 王传伟, 顾佳妮, 王瑾, 赵黎, 黄帅. 腹腔镜结直肠癌根治术后患者早期下床活动现状及影响因素[J]. 上海交通大学学报(医学版), 2023, 43(9): 1201-1210. |
| [9] | 王晓玉, 彭银辉, 马文琳, 姚博爽, 李一凡, 赵莉, 杨春霞. 新冠疫情大流行期间儿童及青少年新发焦虑症状的纵向研究[J]. 上海交通大学学报(医学版), 2023, 43(8): 963-970. |
| [10] | 张媛媛, 吴安琪, 吴捷, 朱雅琪, 李梦瑶, 闫德修, 章雅青, 侯黎莉. 中青年癌症生存者重返工作干预方案的系统评价[J]. 上海交通大学学报(医学版), 2023, 43(3): 333-341. |
| [11] | 唐雷, 徐迎春, 张凤春. 胶原蛋白在肿瘤发生和发展中的作用综述[J]. 上海交通大学学报(医学版), 2023, 43(12): 1577-1584. |
| [12] | 刘砚燕, 杨田田, 沈南平, 何梦雪, 张洪燕. 儿童青少年癌症患者多症状困扰潜在剖面分析及其对体力活动的影响[J]. 上海交通大学学报(医学版), 2023, 43(11): 1408-1416. |
| [13] | 台瑞, 方芳, 毛晶珏, 周霞. 永久性肠造口患者造口适应水平影响因素分析[J]. 上海交通大学学报(医学版), 2023, 43(11): 1423-1429. |
| [14] | 崔培荣, 倪雪萍, 宗明灿, 忻笑, 江雨露, 李贤华. 老年慢性病患者健康信息寻求行为现状及影响因素路径分析[J]. 上海交通大学学报(医学版), 2022, 42(6): 805-812. |
| [15] | 许莉, 杨艳, 陈菡芬, 姜萌, 卜军. 急性心肌梗死患者于心脏康复中心就诊的影响因素及效果评价[J]. 上海交通大学学报(医学版), 2022, 42(5): 646-652. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||