目的·比较成人急诊住院患者胸部CT平扫影像中胸骨皮质比例与骨密度之间的关系,评估胸骨皮质比例对骨量低下及骨质疏松的诊断效能。方法·对2020年11月—2022年10月收治于上海交通大学医学院附属新华医院成人急诊病房的住院患者通过双能X射线吸收法(dual energy X-ray absorptiometry,DXA)测定其骨密度。根据骨密度将患者诊断为骨量正常、骨量低下及骨质疏松。对患者根据年龄(>65岁、≤65岁)及骨质疏松情况进行分组。分析各组患者胸部CT平扫影像中气管分叉处平面测量的胸骨皮质比例。用Spearman相关系数分析胸骨皮质比例与骨密度的相关性。采取胸骨皮质比例对骨量低下及骨质疏松进行诊断,绘制受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)并获得最佳截断值,分析胸骨皮质比例在诊断骨量低下及骨质疏松中的诊断效能。结果·研究共纳入198例患者,其中,骨量正常者78例、骨量低下者66例、骨质疏松者54例。在>65岁的患者(n=115)中,骨质疏松组女性占比、患者年龄高于骨量正常组,差异有统计学意义(均P<0.05);而在≤65岁的患者(n=83)中,该差异均无统计学意义(P>0.05)。不论在>65岁患者,还是在≤65岁的患者中,骨量正常组胸骨皮质比例均高于骨量低下组及骨质疏松组,骨量低下组胸骨皮质比例均高于骨质疏松组(均P<0.05);骨量正常组、骨量低下组及骨质疏松组的女性患者胸骨皮质比例均低于男性患者(均P<0.05),男性和女性患者的胸骨皮质比例均与骨密度呈正相关(r=0.704,P=0.000;r=0.785,P=0.000;r=0.735,P=0.000;r=0.479,P=0.000)。在诊断效能方面,在>65岁的患者中,胸骨皮质比例对骨量正常组男性患者的诊断准确率较骨量低下组及骨质疏松组高,对骨质疏松组患者的诊断误诊率较骨量正常组及骨量低下组低;在≤65岁的患者中,胸骨皮质比例对骨质疏松组男性患者的诊断准确率较骨量正常组及骨量低下组高,对骨量正常组患者的诊断误诊率较骨量低下组及骨质疏松组低。结论·男性和女性患者的胸骨皮质比例均与骨密度呈正相关,胸骨皮质比例对骨量低下及骨质疏松有较好的诊断效能。
关键词:骨质疏松
;
骨密度
;
胸骨
;
骨皮质
;
诊断价值。
Abstract
Objective ·To compare the relationship between sternal cortical thickness ratio and bone mineral density in adult emergency inpatients with chest CT plain scan, and evaluate the diagnostic ability of sternal cortical thickness ratio for osteopenia and osteoporosis. Methods ·The bone density was measured by dual energy X-ray absorptiometry (DXA) in hospitalized patients collected in the adult emergency ward of Xinhua Hospital, Shanghai Jiao Tong University School of Medicine from November 2020 to October 2022, and the patients were diagnosed as normal bone mass, osteopenia, or osteoporosis according to the bone density. The patients were grouped based on age (>65 years old, ≤65 years old) and osteoporosis status. The sternal cortical thickness ratio measured at the level of tracheal bifurcation in the chest CT scan image of each group was analyzed. Spearman correlation was used to analyze the correlation between the sternal cortical thickness ratio and bone mineral density. The sternal cortical thickness ratio was used to diagnose the osteopenia and the osteoporosis, and the receiver operator characteristic curve (ROC curve) was drawn to obtain the best cut-off value. The diagnostic efficacy of the sternal cortical thickness ratio in the diagnosis of osteopenia and osteoporosis was analyzed. Results ·A total of 198 patients were included in the study, including 78 patients with normal bone mass, 66 patients with osteopenia, and 54 patients with osteoporosis. Among patients aged >65 years old (n=115), the proportion of female patients and the age of patients in the osteoporosis group were significantly higher than those in the normal bone mass group (all P<0.05). However, in patients ≤65 years old (n=83), the difference was not statistically significant (P>0.05). Whether in patients >65 years old or ≤65 years old, the sternal cortical thickness ratio in the normal bone mass group was higher than that in the osteopenia group and the osteoporosis group, and the sternal cortical thickness ratio in the osteopenia group was higher than that in the osteoporosis group (all P<0.05); The sternal cortical thickness ratio in female patients in the normal bone mass group, osteopenia group and osteoporosis group was lower than that in male patients (all P<0.05). The sternal cortical thickness ratio in both male and female patients was positively correlated with bone mineral density (r=0.704, P=0.000; r=0.785, P=0.000; r=0.735, P=0.000; r=0.479, P=0.000). In terms of diagnostic performance, in patients >65 years old, the diagnostic accuracy rate of male patients in the normal bone mass group was higher than that in the osteopenia group and the osteoporosis group, and the diagnosis misdiagnosis rate in the osteoporosis group was lower than that in the normal bone mass group and the osteopenia group; In patients ≤65 years old, the diagnostic accuracy rate of male patients in the osteoporosis group was higher than that in the normal bone mass group and the osteopenia group, and the diagnosis misdiagnosis rate in the normal bone mass group was lower than that in the osteopenia group and the osteoporosis group. Conclusion ·The sternal cortical thickness ratio in both male and female patients is positively correlated with bone mineral density, and the sternal cortical thickness ratio has good diagnostic efficacy for osteopenia and osteoporosis.
Keywords:osteoporosis
;
bone mineral density
;
sternum
;
cortical bone
;
diagnostic value
YU Xi, SUN Junnan, ZHANG Jiaojiao, GAO Yue, WANG Hu, YU Yang, WANG Hairong, HONG Wen. Efficacy of sternal cortical thickness ratio in adult chest CT in the diagnosis of osteopenia and osteoporosis. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(10): 1274-1281 doi:10.3969/j.issn.1674-8115.2023.10.008
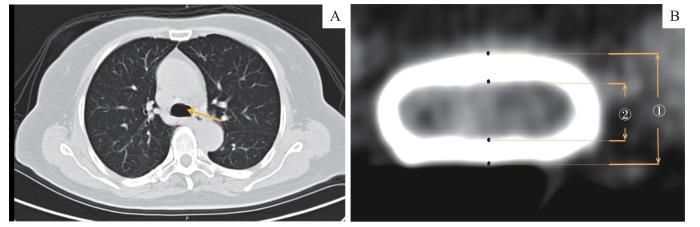
Note: A. The measurement plane at the tracheal bifurcation. The arrow points to the tracheal bifurcation. B. The calculation of the sternal cortical thickness ratio in the measurement plane. ① represents the thickness of the outer edge of the sternal cortex; ② represents the thickness of the inner edge of the sternal cortex; (①‒②)/① is the sternal cortical thickness ratio.
Fig 1
Measurement of cortical thickness in the sternum measurement plane
1.5 统计学方法
采用SPSS 22.0软件进行统计分析。定量资料用x±s表示,2组间数据比较采用独立样本t检验,多组间数据比较采用单因素方差分析。定性资料用n(%)表示,组间比较采用χ2 检验。采用Spearman相关分析胸骨皮质比例与骨密度的相关性;采用受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)计算最佳截断值,并比较曲线下面积(area under the curve,AUC)、特异度、敏感度、误诊率及漏诊率,判断其对骨质疏松的诊断效能。所有检验均为双侧检验,P<0.05表示差异有统计学意义。
The study was designed by WANG Hairong, HONG Wen and YU Yang. The data analysis was enforced by SUN Junnan, ZHANG Jiaojiao, GAO Yue and WANG Hu. The research implementation, and manuscript drafting and revision were enforced by WANG Hairong and YU Xi. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
BIJLSMA A Y, MESKERS C M, WESTENDORP R J, et al. Chronology of age-related disease definitions: osteoporosis and sarcopenia[J]. Ageing Res Rev, 2012, 11(2): 320-324.
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy[J]. JAMA, 2001, 285(6): 785-795.
Osteoporosis and Bone Mineral Disease Branch of Chinese Medical Association. Guidelines for the diagnosis and treatment of primary osteoporosis (2011)[J]. Chinese Journal of Osteoporosis and Bone Mineral Research, 2011, 4(1): 2-17.
Osteoporosis and Bone Mineral Disease Branch of Chinese Medical Association. Guidelines for the diagnosis and treatment of primary osteoporosis (2017)[J]. Chinese Journal of Osteoporosis, 2019, 25(3): 281-309.
MA Y Z, WANG Y P, LIU Q, et al. Guidelines for the diagnosis and treatment of osteoporosis in the elderly in China (2018)[J]. Chinese Journal of Osteoporosis, 2018, 24(12): 1541-1565.
LI F Z, ECKSTROM E, HARMER P, et al. Exercise and fall prevention: narrowing the research-to-practice gap and enhancing integration of clinical and community practice[J]. J Am Geriatr Soc, 2016, 64(2): 425-431.
LIU L. Clinical discussion of DXA imaging evaluation and bone densitometry in the diagnosis of primary osteoporosis[J]. Journal of Imaging Research and Medical Applications, 2019, 3(17): 50-51.
JANG S, GRAFFY P M, ZIEMLEWICZ T J, et al. Opportunistic osteoporosis screening at routine abdominal and thoracic CT: normative L1 trabecular attenuation values in more than 20 000 adults[J]. Radiology, 2019, 291(2): 360-367.
LESLIE W D, GIANGREGORIO L M, YOGENDRAN M, et al. A population-based analysis of the post-fracture care gap 1996‒2008: the situation is not improving[J]. Osteoporos Int, 2012, 23(5): 1623-1629.
TINGART M J, APRELEVA M, VON STECHOW D, et al. The cortical thickness of the proximal humeral diaphysis predicts bone mineral density of the proximal humerus[J]. J Bone Joint Surg Br, 2003, 85(4): 611-617.
YOSHII I, AKITA K. Cortical thickness relative to the transverse diameter of third metacarpal bone reflects bone mineral density in patients with rheumatoid arthritis[J]. Bone, 2020, 137: 115405.
MATHER J, MACDERMID J C, FABER K J, et al. Proximal humerus cortical bone thickness correlates with bone mineral density and can clinically rule out osteoporosis[J]. J Shoulder Elbow Surg, 2013, 22(6): 732-738.
PISTOIA W, VAN RIETBERGEN B, RÜEGSEGGER P. Mechanical consequences of different scenarios for simulated bone atrophy and recovery in the distal radius[J]. Bone, 2003, 33(6): 937-945.
RAUSCH S, KLOS K, GRAS F, et al. Utility of the cortical thickness of the distal radius as a predictor of distal-radius bone density[J]. Arch Trauma Res, 2013, 2(1): 11-15.
YE C X, GUO Y B, ZHENG Y H, et al. Distal radial cortical bone thickness correlates with bone mineral density and can predict osteoporosis: a cohort study[J]. Injury, 2020, 51(11): 2617-2621.
PICKHARDT P J, POOLER B D, LAUDER T, et al. Opportunistic screening for osteoporosis using abdominal computed tomography scans obtained for other indications[J]. Ann Intern Med, 2013, 158(8): 588-595.
LEE S J, BINKLEY N, LUBNER M G, et al. Opportunistic screening for osteoporosis using the sagittal reconstruction from routine abdominal CT for combined assessment of vertebral fractures and density[J]. Osteoporos Int, 2016, 27(3): 1131-1136.
NAZIA FATHIMA S M, TAMILSELVI R, PARISA BEHAM M, et al. Diagnosis of osteoporosis using modified U-net architecture with attention unit in DEXA and X-ray images[J]. J Xray Sci Technol, 2020, 28(5): 953-973.
YAO Q, LIU J, YUAN K, et al. Comparison of L1 CT-attenuation and cortical thickness in predicting osteoporosis by opportunistic CT[J]. J Xray Sci Technol, 2022, 30(3): 631-640.
MECZEKALSKI B, PODFIGURNA-STOPA A, GENAZZANI A R. Hypoestrogenism in young women and its influence on bone mass density[J]. Gynecol Endocrinol, 2010, 26(9): 652-657.
POSTNOV A A, VINOGRADOV A V, VAN DYCK D, et al. Quantitative analysis of bone mineral content by X-ray microtomography[J]. Physiol Meas, 2003, 24(1): 165-178.
ITOH S, TOMIOKA H, TANAKA J, et al. Relationship between bone mineral density of the distal radius and ulna and fracture characteristics[J]. J Hand Surg Am, 2004, 29(1): 123-130.
LI Y L, WONG K H, LAW M W, et al. Opportunistic screening for osteoporosis in abdominal computed tomography for Chinese population[J]. Arch Osteoporos, 2018, 13(1): 76.
MA D T, WANG J X, LI R G, et al. Observation of sternum variation based on multimodal multi-slice spiral CT[J]. Chinese Journal of Anatomy and Clinics, 2022, 27(2): 87-91.
XU L Z, CHEN M S, SI L. Current status, challenges and suggestions of health economics evaluation research on osteoporosis[J].Chinese Journal of Endocrinology and Metabolism, 2021, 37(9): 859-862.



{kind=link}
{kind=link}
{kind=link}
{kind=link}