Evaluation of clinical effect of manipulation on masticatory muscle pain guided by MRI
YANG Haixia,1, XU Lili1, WANG Bocheng2, CHEN Minjie,3
1.Department of Physical Medicine & Rehabilitation, Shanghai Ninth People′s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
2.Department of Radiology, Shanghai Ninth People′s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
3.Department of Oral Surgery, Shanghai Ninth People′s Hospital, Shanghai Jiao Tong University School of Medicine; College of Stomatology, Shanghai Jiao Tong University; National Center for Stomatology; National Clinical Research Center for Oral Diseases; Shanghai Key Laboratory of Stomatology, Shanghai 200011, China
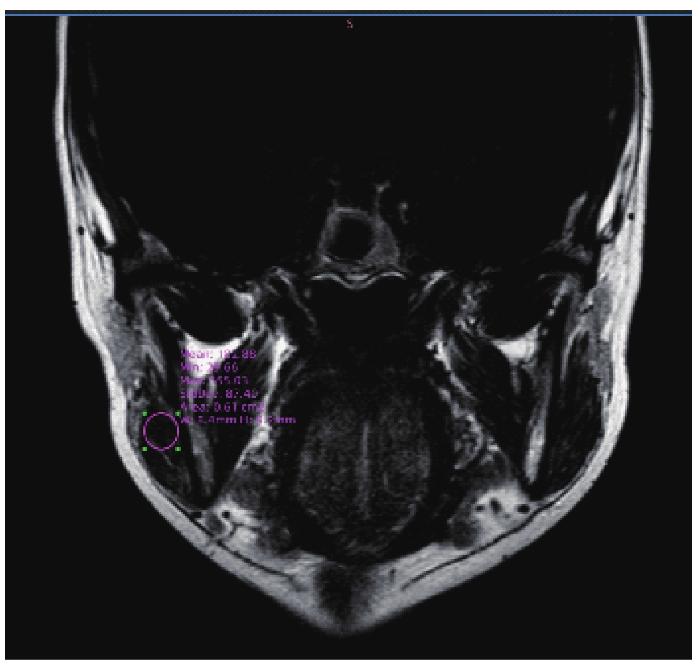
Objective ·To assess muscle changes of patients of temporomandibular joint disorder with nonstructural disorder by using the Dixon technique for MRI of masticatory muscle, and evaluate the clinical effect of manipulation on masticatory muscle pain guided by MRI. Methods ·A total of 29 patients with TMD masticatory muscle pain (without disc displacement) who were diagnosed for the first time in the Department of Oral Surgery, Shanghai Ninth People′s Hospital, Shanghai Jiao Tong University School of Medicine from June 2021 to September 2022 were included. Among them, 9 cases who were assessed with Dixon technique for MRI of masticatory muscle were collected and treated by manipulation. Before treatment, the DICOM Viewer workstation was used to compare the value of masticatory muscle pain area (Z1), the value of ipsilateral non-pain area (Z2) and the value of contralateral corresponding masticatory muscle area (Z3) in Dixon image. Manipulation therapy was performed according to the area of abnormal threshold. Follow-up was performed for 1-4 weeks after treatment, the active maximum mouth opening (MMO) and Visual Analogue Scale (VAS) before and after treatment were compared, and the value of masticatory muscle pain area in Dixon image after treatment was obtained again to evaluate the clinical efficacy. Results ·The mean value of Z2 and Z3 in Dixon was (66.23±32.90) and (66.27±33.87), while Z1 in masticatory muscle pain region was (131.94±83.99), which was significantly higher than Z2 and Z3. Manipulation therapy showed significant improvement in MMO and VAS, and the effective rate was 88.89%. Conclusion ·There is a significant correlation between the imaging findings of Dixon technique for MRI and the pain points of the masticatory muscle reported by the clinical complaints. The manipulation therapy guided by Dixon technique for MRI has a significant effect on improving the degree of mouth opening and pain.
YANG Haixia, XU Lili, WANG Bocheng, CHEN Minjie. Evaluation of clinical effect of manipulation on masticatory muscle pain guided by MRI. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(5): 540-544 doi:10.3969/j.issn.1674-8115.2023.05.004
The study was designed by YANG Haixia and CHEN Minjie; The manuscript was drafted and revised by YANG Haixia; Image data was analyzed by WANG Bocheng; Clinical data was analyzed by XU Lili. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
MAÍSA S G, MARCELE J P, CÉLIA M R. Temporomandibular disorders in fibromyalgia syndrome: a short-communication[J]. Revista Brasileira de Reumatologia, 2015, 55(2): 189-194.
HARKINS S, LINFORD J, COHEN J, et al. Administration of clonazepam in the treatment of TMD and associated myo-fascial pain: a double-blind pilot study[J]. J Craniomandib Disord, 1991, 5(3): 179-186.
VENANCIO R A, ALENCAR F J, ZAMPERINI C. Botulinum toxin, lidocaine, and dry-needling injections in patients with myofascial pain and headaches[J]. Cranio, 2009, 27(1): 46-53.
AL-ANI Z, GRAY R J, DAVIES S J, et al. Stabilization splint therapy for the treatment of temporomandibular myofascial pain: a systematic review[J]. J Dent Educ, 2005, 69(11): 1242-1250.
VENEZIAN G C, DA S M, MAZZETTO R G, et al. Low level laser effects on pain to palpation and electromyographic activity in TMD patients: a double-blind, randomized, placebo-controlled study[J]. Cranio, 2010, 28(2): 84-91.
DE L A, STAPPAERTS K, PAPY S. Consueling and physical therapy as treatment for myofascial pain of the masticatory system[J]. J Orofac Pain, 2003, 17(1): 42-49.
LEE Y H, LEE K M,AUH Q S, et al. Magnetic resonance imaging-based prediction of the relationship between whiplash injury and temporomandibular disorders[J]. Front Neurol, 2017, 8, 725.
VAN D J, PENNATI F, HANSEN H H, et al. Respiratory muscle imaging by ultrasound and MRI in neuromuscular disorders[J]. Eur Respir J, 2021, 58(5): 2100137.
DELGADO E V, ROMERO J C, ESCODA C G. Myofascial pain syndrome associated with trigger points: a literature review. (I): Epidemiology, clinical treatment and etiopathogeny[J]. Med Oral Pathol Oral Cir Bucal, 2009, 14(10):e494-e498.
ARIJI Y, SAKUMA S, IZUMI M, et al. Ultrasonographic features of the masseter muscle in female patients with temporomandibular disorder associated with myofascial pain[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2004, 98: 334-41.
BAKKE M, THOMSEN C E, VILMANN A, et al. Ultrasonographic assessment of the swelling of the human masseter muscle after static and dynamic activity[J]. Arch Oral Biol, 1996, 41: 133-40.
YUTAKA N, HIDEYOSHI N, TAKAHUMI H I. The relationship between masseter muscle pain and T2 values in temporomandibular joint disorders[J]. Oral Surg Oral Med Oral Pathol Oral Radiol, 2018,126(4): 349-354.
MEDLICOTT M S, HARRIS S R. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder[J]. Phys Ther, 2006, 86: 955-973.
GYER G, MICHAEL J, INKLEBARGER J, et al. Spinal manipulation therapy: is it all about the brain? A current review of the neurophysiological effects of manipulation[J]. J Integr Med, 2019, 17(5): 328-337.
URBAŃSKI P, TRYBULEC B, PIHUT M. The Application of Manual Techniques in Masticatory Muscles Relaxation as Adjunctive Therapy in the Treatment of Temporomandibular Joint Disorders[J]. Int J Environ Res Public Health, 2021, 18(24): 12970.



{kind=link}
{kind=link}
{kind=link}
{kind=link}