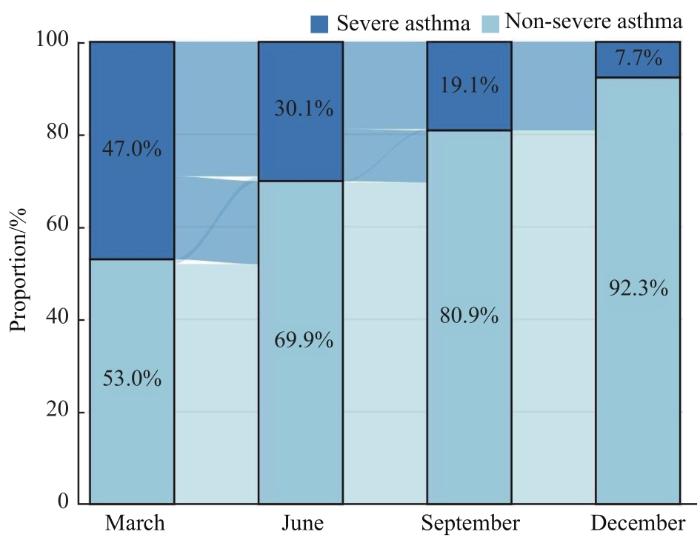
目的·探讨儿童重症支气管哮喘(简称哮喘)的流行病学特征并分析其危险因素。方法·采用单中心前瞻性队列研究,纳入2021年1月1日—12月31日就诊于复旦大学附属儿科医院的难治性哮喘患儿674例,建立动态队列。收集队列成员的基本信息(包括患儿性别、年龄、出生胎龄、出生体质量等)和共存疾病情况,评估其哮喘控制情况、药物吸入技术水平、药物依从性,以及肺功能指标[1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比]、气道炎症指标[呼出气一氧化氮(fraction exhaled nitric oxide,FeNO)检测值]和过敏状态指标[外周血嗜酸性粒细胞(eosinophil,EOS)计数和总血清免疫球蛋白E(immunoglobulin E,IgE)浓度]。所有队列成员分别在其进入队列的第3、6、9和12个月至该院哮喘专病门诊接受再次评估。结果·至队列终点时,有52例(7.7%)患儿被诊断为重症哮喘。处于二手烟暴露环境、家中常年使用空调、共存疾病为鼻炎/鼻窦炎、FEV1%预计值<80%、FEV1/FVC<80%、小气道功能障碍、EOS>300/μL、IgE>200国际单位(international unit,IU)/L、FeNO>20/25 ppb[FeNO>20 ppb(≤12岁),>25 ppb(>12岁),1 ppb=1×10-9 mol/L]在重症哮喘患儿中占比较高,母乳喂养至6月龄及以上、药物依从性好在非重症患儿中占比较高,差异有统计学意义(均P<0.05)。6~11岁重症哮喘患儿中男性占比更多,12~17岁重症哮喘患儿中女性占比更多,差异有统计学意义(均P<0.05)。多因素Logistic回归分析显示,小气道功能障碍是发生重症哮喘的独立危险因素[OR=5.158(95%CI 2.516~10.572)]。结论·难治性哮喘患儿在规范管理1年后,重症哮喘患儿占比有显著下降趋势;小气道功能障碍是其进展为重症哮喘的独立危险因素。
关键词:儿童
;
哮喘
;
重症
;
诊断
;
治疗
Abstract
Objective ·To explore the epidemiological characteristics of severe asthma in children and analyze the risk factors. Methods ·A single-center prospective cohort study was conducted. Six hundred and seventy four children with difficult-to-treat asthma who visited the Children´s Hospital of Fudan University from January 1 to December 31, 2021 were included to establish a dynamic cohort. Basic information (including gender, age, gestational age at birth, birth weight, etc.) and comorbidity of the cohort members were collected. The asthma control status, drug inhalation technique level, medication compliance, pulmonary function parameters [forced expiratory volume in one second (FEV1) as a percent-age of the predicted value (FEV1%pred), FEV1/ forced vital capacity (FVC), and the rate of estimated values of forced expiratory flow at 50% of FVC exhaled (FEF50), FEF75, and FEF25-75 in percent-predicted value, respectively], airway inflammation index [fraction exhaled nitric oxide (FeNO)], and allergy status parameters [eosinophil (EOS) and immunoglobulin E (IgE)] of all cohort members were evaluated. All cohort members underwent re-evaluation respectively at the specialist asthma clinic of the hospital at 3, 6, 9, and 12 months. Results ·At the endpoint of the cohort, 52 children were diagnosed with severe asthma, accounting for 7.7%. A high proportion of severe asthma was found in children who were exposed to secondhand smoke, used air conditioning at home all year round, or had coexisting rhinitis/nasosinusitis, FEV1%pred<80%, FEV1/FVC<80%, small airway dysfunction, EOS>300/μL, IgE>200 IU/L, or FeNO>20/25 ppb [FeNO>20 ppb (≤12 years old) or >25 ppb (>12 years old), 1 ppb=1×10-9 mol/L]. A high proportion of non-severe asthma was found in children who were breastfed for 6 months or longer, or had good medication compliance. The differences were statistically significant (all P<0.05). There were more males in children with severe asthma aged 6‒11 years, and more females in children with severe asthma aged 12‒17 years, with statistical significance (both P<0.05). Multiple-factor Logistic regression analysis showed that only small airway dysfunction was an independent risk factor for severe asthma [OR=5.158 (95%CI 2.516‒10.572)]. Conclusion ·The proportion of children with severe asthma has a significantly decrease after one year of standardized management in children with difficult-to-treat asthma. Small airway dysfunction is an independent risk factor for the progression to severe asthma.
Keywords:child
;
asthma
;
severe
;
diagnosis
;
treatment
WANG Yingwen, LI Xiaoling, DAI Jiajia, LIU Fang, HUANG Jianfeng, WANG Libo, ZHANG Xiaobo, FENG Rui. Epidemiological characteristics and risk factors of severe asthma in children: a single-center prospective cohort study. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(6): 665-672 doi:10.3969/j.issn.1674-8115.2023.06.002
使用我院自主设计的儿童哮喘专病数据库完成队列患儿随访。该专病数据库基于“互联网+医疗照护”服务理念,以“线上+线下”“院内+院外”镶嵌形式为框架,于2020年12月以浏览器/服务器(browser/server,B/S)架构嵌入我院信息系统(hospital information system,HIS),通过医院微信公众号与患儿端进行数据交换。符合纳入标准的患儿于初诊当日由家长通过订阅微信公众号入库,由数据库系统生成个人随访档案。专病数据库每月通过微信公众号向患儿推送哮喘控制测试评分问卷等,收到反馈数据后将之自动导入随访信息模块并通过既定算法进行实时分析,根据评估得分对应推送就诊或重新评估的建议,以及文字、图片或视频形式的哮喘相关教育信息。在各自随访的第3、6、9、12个月,患儿至我院哮喘专病门诊接受临床访视,由专科医护团队进行体格检查,评估患儿哮喘控制情况、药物吸入技术水平、服药依从性,检测其肺功能、气道炎症指标和过敏状态。结合既往病史数据,综合分析结果后,根据患儿对前段哮喘治疗的反应,进行治疗策略的优化调整,与家庭共同制定个体化哮喘管理行动计划。
1.3.2 评估方法
(1)哮喘相关症状和因素评估
通过微信平台推送问卷以及临床访视获取数据:①哮喘控制测试评分。微信平台推送相应问卷,患儿和/或家长填写后,由专病数据库收集结果。患儿≥6岁且<12岁使用儿童版哮喘控制测试问卷(Childhood Asthma Control Test,C-ACT),患儿>12岁使用哮喘控制测试问卷(Asthma Control Test,ACT)[10-11]。其中C-ACT为评价患儿近4周哮喘控制情况,共7题,第1~4题(4级评分,0分代表最差,3分代表最好)由患儿回答或家长协助回答,第5~7题由家长回答(6级评分,0分代表最差,5分代表最好),总分29分;ACT为患儿自我报告问卷,同样评价患儿近4周哮喘控制情况,共5题(5级评分,1分代表最差,5分代表最好),总分25分;C-ACT或ACT评分<20分代表症状未控制[12]。②药物吸入技术水平。临床访视时,由哮喘专科护士根据药物吸入技术操作标准,对患儿给药操作进行观察性评估后作出判定(合格或不合格),结果由专科护士手动录入专病数据库。③药物依从性。由微信平台推送哮喘药物依从性量表(Medication Adherence Report Scale for Asthma,MARS-A)[13],患儿或家长填写后,由专病数据库收集结果。由患儿自我报告或家长协助报告,评价患儿吸入性糖皮质激素的使用情况,共10个条目(5级评分,1分代表该情况总是发生,5分代表从未发生),结果取各条目得分的均值,MARS-A≥4.5为药物依从性好。
(2)肺功能检测
临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测。为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训。检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频。检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比。参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍。
Tab 1 Baseline characteristics of children diagnosed with severe and non-severe asthma at the 12-month follow-up (n=674)
Item
Non-severe asthma (n=622)
Severe asthma (n=52)
Z/χ2 value
P value
Male/n(%)
419 (67.4)
37 (71.2)
0.166
0.684
Age/year
9.0 (6.0, 13.0)
9.0 (6.8, 12.2)
0.228
0.820
Age groups/n(%)
0.003
0.957
6‒11 years old
338 (54.3)
29 (55.8)
12‒17 years old
284 (45.7)
23 (44.2)
Gestational age<37 weeks/n(%)
33 (5.3)
5 (9.6)
0.963
0.326
Birth weight<2 500 g/n(%)
59 (9.5)
6 (11.5)
0.056
0.812
Taking vitamin D supplements regularly until 3-year-old/n(%)
277 (44.5)
27 (51.9)
0.781
0.377
Taking vitamin D supplements regularly during pregnancy/n(%)
298 (47.9)
31 (59.6)
2.184
0.139
Mother′s age at delivery/year
29.0 (26.0, 32.0)
29.0 (27.0, 31.2)
-0.242
0.809
Breastfeeding≥6 months/n(%)
333 (53.5)
10 (19.2)
21.247
0.000
Reside in city/n(%)
539 (86.7)
46 (88.5)
0.024
0.876
Expose to second-hand smoking at home/n(%)
95 (15.3)
15 (28.8)
5.518
0.019
Long-term use of air conditioning/n(%)
501 (80.5)
52 (100.0)
11.044
0.001
Annual household income/n(%)
0.349
0.840
<100 000 CNY
101 (16.2)
8 (15.4)
≥100 000 and <200 000 CNY
307 (49.4)
24 (46.2)
≥200 000 CNY
214 (34.4)
20 (38.5)
Educational level of the main household/n(%)
0.067
0.796
Senior high school or lower
116 (18.6)
11 (21.2)
College and above
506 (81.4)
41 (78.8)
Comorbidity/n(%)
Obesity
137 (22.0)
17 (32.7)
2.522
0.112
Obstructive sleep apnea
59 (9.5)
8 (15.4)
1.265
0.261
Rhinitis/sinusitis
317 (51.0)
38 (73.1)
8.546
0.003
MARS-A≥4.5/n(%)
301 (48.4)
17 (32.7)
4.137
0.042
Correct inhaler technique/n(%)
140 (22.5)
17 (32.7)
2.245
0.134
Pulmonary function/n(%)
FEV1%pred<80%
2 (0.3)
17 (32.7)
171.928
0.000
FEV1/FVC<80%
0 (0)
7 (13.5)
72.019
0.000
Small airway dysfunction①
32 (5.1)
40 (76.9)
251.658
0.000
EOS>300 μL-1/n(%)
329 (52.9)
46 (88.5)
23.176
0.000
IgE>200 (IU·L-1)/n(%)
260 (41.8)
47 (90.4)
43.733
0.000
FeNO>20 or 25 ppb②/n(%)
390 (62.7)
52 (100.0)
27.947
0.000
C-AST or ACT<20/n(%)
51 (8.2)
52 (100.0)
305.321
0.000
Note: CNY—Chinese yuan; FEV1%pred—FEV1 as a percentage of the predicted value. ①Small airway dysfunction is defined as FEF50, FEF75 and FEF25-75 as a percentage of the predicted value with any two items less than 65%. ②FeNO>20 ppb (≤12 years old) or >25 ppb (>12 years old).
The study was designed by WANG Yingwen, LI Xiaoling, ZHANG Xiaobo and Feng Rui. The manuscript was drafted and revised by WANG Yingwen, LI Xiaoling, ZHANG Xiaobo, Feng Rui and HUANG Jianfeng. The data analysis was conducted by WANG Yingwen and LI Xiaoling. DAI Jiajia, LIU Fang and WANG Libo participated in the data collection. All the authors have read the last version of paper and consented for submission.
HUANG K, YANG T, XU J, et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study[J]. Lancet, 2019, 394(10196): 407-418.
The Editorial Board, Chinese Journal of Pediatrics, the Subspecialty Group of Respiratory Diseases, the Society of Pediatrics, Chinese Medical Association, the Children′s Respiratory Professional Committee, the Society of Pediatrics of Chinese Medical Doctor Association. Recommendations for diagnosis and management of bronchial asthma in children (2020)[J].Chinese Journal of Pediatrics, 2020, 58(9): 708-717.
XIANG L, ZHAO J, ZHENG Y J, et al. Uncontrolled asthma and its risk factors in Chinese children: a cross-sectional observational study[J]. J Asthma, 2016, 53(7): 699-706.
HONG J G. Pay attention to the diagnosis and treatment of difficult-to-treat asthma / severe asthma in children[J]. Chinese Journal of Allergy & Clinical Immunology, 2019, 13(4): 267-270.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2022[EB/OL]. [2022-12-09]. https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022- FINAL-22-07-01-WMS.pdf.
LIU F, ZHANG Y R, Li X L, et al. Construction and application of an asthma: specific database for children[J]. Journal of Nursing Science, 2022, 37(19): 25-28.
LIU A H, ZEIGER R, SORKNESS C, et al. Development and cross-sectional validation of the Childhood Asthma Control Test[J]. J Allergy Clin Immunol, 2007, 119(4): 817-825.
NATHAN R A, SORKNESS C A, KOSINSKI M, et al. Development of the asthma control test: a survey for assessing asthma control[J]. J Allergy Clin Immunol, 2004, 113(1): 59-65.
THOMAS M, KAY S, PIKE J, et al. The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: analysis of a multinational cross-sectional survey[J]. Prim Care Respir J, 2009, 18(1): 41-49.
COHEN J L, MANN D M, WISNIVESKY J P, et al. Assessing the validity of self-reported medication adherence among inner-city asthmatic adults: the Medication Adherence Report Scale for Asthma[J]. Ann Allergy Asthma Immunol, 2009, 103(4): 325-331.
FU W J, TANG L F, YE C J, et al. Implementation of an artificial intelligence based clinical decision support system on historical pulmonary function reports[J]. China Medical Device Information, 2022, 28(14): 147-150.
Pulmonary Function Group, Respiratory Branch of Chinese Pediatric Society of Chinese Medical Association, Editorial Board of Chinese Journal of Applied Clinical Pediatrics. Series guidelines for pediatric pulmonary function (part Ⅱ): lung volume and spirometry[J]. Chinese Journal of Applied Clinical Pediatrics, 2016, 31(10): 744-750.
CULVER B H, GRAHAM B L, COATES A L, et al. Recommendations for a standardized pulmonary function report. An official American thoracic society technical statement[J]. Am J Respir Crit Care Med, 2017, 196(11): 1463-1472.
Collaboration Group of Asthma, the Subspecialty Group of Respiratory Diseases, the Society of Pediatrics, Chinese Medical Association. Expert consensus on detection and clinical application of exhaled nitric oxide in children (2021 edition) [J]. Chinese Journal of Applied Clinical Pediatrics, 2021, 36(6): 417-423.
ROSS K R, GUPTA R, DEBOER M D, et al. Severe asthma during childhood and adolescence: a longitudinal study[J]. J Allergy Clin Immunol, 2020, 145(1): 140-146.e9.
LEYNAERT B, SUNYER J, GARCIA-ESTEBAN R, et al. Gender differences in prevalence, diagnosis and incidence of allergic and non-allergic asthma: a population-based cohort[J]. Thorax, 2012, 67(7): 625-631.
CHIPPS B E, HASELKORN T, PAKNIS B, et al. More than a decade follow-up in patients with severe or difficult-to-treat asthma: The Epidemiology and Natural History of Asthma: Outcomes and Treatment Regimens (TENOR) Ⅱ[J]. J Allergy Clin Immunol, 2018, 141(5): 1590-1597.e9.
DEBOER M D, PHILLIPS B R, MAUGER D T, et al. Effects of endogenous sex hormones on lung function and symptom control in adolescents with asthma[J]. BMC Pulm Med, 2018, 18(1): 58.
TAI A, TRAN H, ROBERTS M, et al. The association between childhood asthma and adult chronic obstructive pulmonary disease[J]. Thorax, 2014, 69(9): 805-810.
MUKHERJEE M, STODDART A, GUPTA R P, et al. The epidemiology, healthcare and societal burden and costs of asthma in the UK and its member nations: analyses of standalone and linked national databases[J]. BMC Med, 2016, 14(1): 113.
HEDLIN G, BUSH A, LØDRUP CARLSEN K, et al. Problematic severe asthma in children, not one problem but many: a GA2LEN initiative[J]. Eur Respir J, 2010, 36(1): 196-201.
DE ANDRADE W C, LASMAR L M, RICCI C D E A, et al. Phenotypes of severe asthma among children and adolescents in Brazil: a prospective study[J]. BMC Pulm Med, 2015, 15: 36.
JARJOUR N N, ERZURUM S C, BLEECKER E R, et al. Severe asthma: lessons learned from the National Heart, Lung, and Blood Institute Severe Asthma Research Program[J]. Am J Respir Crit Care Med, 2012, 185(4): 356-362.
LI R, DONG X Y, JIANG K, et al. Application of fractional exhaled nitric oxide and nasal nitric oxide in control evaluation of bronchial asthma and diagnosis of allergic rhinitis in children[J]. Chinese Journal of Contemporary Pediatrics, 2022, 24(1) :90-95.
KOULOUMENTA V, HATZIEFTHIMIOU A, PARASKEVA E, et al. Non-genomic effect of testosterone on airway smooth muscle[J]. Br J Pharmacol, 2006, 149(8): 1083-1091.
FUSEINI H, YUNG J A, CEPHUS J Y, et al. Testosterone decreases house dust mite-induced type 2 and IL-17A-mediated airway inflammation[J]. J Immunol, 2018, 201(7): 1843-1854.
... 通过微信平台推送问卷以及临床访视获取数据:①哮喘控制测试评分.微信平台推送相应问卷,患儿和/或家长填写后,由专病数据库收集结果.患儿≥6岁且<12岁使用儿童版哮喘控制测试问卷(Childhood Asthma Control Test,C-ACT),患儿>12岁使用哮喘控制测试问卷(Asthma Control Test,ACT)[10-11].其中C-ACT为评价患儿近4周哮喘控制情况,共7题,第1~4题(4级评分,0分代表最差,3分代表最好)由患儿回答或家长协助回答,第5~7题由家长回答(6级评分,0分代表最差,5分代表最好),总分29分;ACT为患儿自我报告问卷,同样评价患儿近4周哮喘控制情况,共5题(5级评分,1分代表最差,5分代表最好),总分25分;C-ACT或ACT评分<20分代表症状未控制[12].②药物吸入技术水平.临床访视时,由哮喘专科护士根据药物吸入技术操作标准,对患儿给药操作进行观察性评估后作出判定(合格或不合格),结果由专科护士手动录入专病数据库.③药物依从性.由微信平台推送哮喘药物依从性量表(Medication Adherence Report Scale for Asthma,MARS-A)[13],患儿或家长填写后,由专病数据库收集结果.由患儿自我报告或家长协助报告,评价患儿吸入性糖皮质激素的使用情况,共10个条目(5级评分,1分代表该情况总是发生,5分代表从未发生),结果取各条目得分的均值,MARS-A≥4.5为药物依从性好. ...
1
... 通过微信平台推送问卷以及临床访视获取数据:①哮喘控制测试评分.微信平台推送相应问卷,患儿和/或家长填写后,由专病数据库收集结果.患儿≥6岁且<12岁使用儿童版哮喘控制测试问卷(Childhood Asthma Control Test,C-ACT),患儿>12岁使用哮喘控制测试问卷(Asthma Control Test,ACT)[10-11].其中C-ACT为评价患儿近4周哮喘控制情况,共7题,第1~4题(4级评分,0分代表最差,3分代表最好)由患儿回答或家长协助回答,第5~7题由家长回答(6级评分,0分代表最差,5分代表最好),总分29分;ACT为患儿自我报告问卷,同样评价患儿近4周哮喘控制情况,共5题(5级评分,1分代表最差,5分代表最好),总分25分;C-ACT或ACT评分<20分代表症状未控制[12].②药物吸入技术水平.临床访视时,由哮喘专科护士根据药物吸入技术操作标准,对患儿给药操作进行观察性评估后作出判定(合格或不合格),结果由专科护士手动录入专病数据库.③药物依从性.由微信平台推送哮喘药物依从性量表(Medication Adherence Report Scale for Asthma,MARS-A)[13],患儿或家长填写后,由专病数据库收集结果.由患儿自我报告或家长协助报告,评价患儿吸入性糖皮质激素的使用情况,共10个条目(5级评分,1分代表该情况总是发生,5分代表从未发生),结果取各条目得分的均值,MARS-A≥4.5为药物依从性好. ...
1
... 通过微信平台推送问卷以及临床访视获取数据:①哮喘控制测试评分.微信平台推送相应问卷,患儿和/或家长填写后,由专病数据库收集结果.患儿≥6岁且<12岁使用儿童版哮喘控制测试问卷(Childhood Asthma Control Test,C-ACT),患儿>12岁使用哮喘控制测试问卷(Asthma Control Test,ACT)[10-11].其中C-ACT为评价患儿近4周哮喘控制情况,共7题,第1~4题(4级评分,0分代表最差,3分代表最好)由患儿回答或家长协助回答,第5~7题由家长回答(6级评分,0分代表最差,5分代表最好),总分29分;ACT为患儿自我报告问卷,同样评价患儿近4周哮喘控制情况,共5题(5级评分,1分代表最差,5分代表最好),总分25分;C-ACT或ACT评分<20分代表症状未控制[12].②药物吸入技术水平.临床访视时,由哮喘专科护士根据药物吸入技术操作标准,对患儿给药操作进行观察性评估后作出判定(合格或不合格),结果由专科护士手动录入专病数据库.③药物依从性.由微信平台推送哮喘药物依从性量表(Medication Adherence Report Scale for Asthma,MARS-A)[13],患儿或家长填写后,由专病数据库收集结果.由患儿自我报告或家长协助报告,评价患儿吸入性糖皮质激素的使用情况,共10个条目(5级评分,1分代表该情况总是发生,5分代表从未发生),结果取各条目得分的均值,MARS-A≥4.5为药物依从性好. ...
1
... 通过微信平台推送问卷以及临床访视获取数据:①哮喘控制测试评分.微信平台推送相应问卷,患儿和/或家长填写后,由专病数据库收集结果.患儿≥6岁且<12岁使用儿童版哮喘控制测试问卷(Childhood Asthma Control Test,C-ACT),患儿>12岁使用哮喘控制测试问卷(Asthma Control Test,ACT)[10-11].其中C-ACT为评价患儿近4周哮喘控制情况,共7题,第1~4题(4级评分,0分代表最差,3分代表最好)由患儿回答或家长协助回答,第5~7题由家长回答(6级评分,0分代表最差,5分代表最好),总分29分;ACT为患儿自我报告问卷,同样评价患儿近4周哮喘控制情况,共5题(5级评分,1分代表最差,5分代表最好),总分25分;C-ACT或ACT评分<20分代表症状未控制[12].②药物吸入技术水平.临床访视时,由哮喘专科护士根据药物吸入技术操作标准,对患儿给药操作进行观察性评估后作出判定(合格或不合格),结果由专科护士手动录入专病数据库.③药物依从性.由微信平台推送哮喘药物依从性量表(Medication Adherence Report Scale for Asthma,MARS-A)[13],患儿或家长填写后,由专病数据库收集结果.由患儿自我报告或家长协助报告,评价患儿吸入性糖皮质激素的使用情况,共10个条目(5级评分,1分代表该情况总是发生,5分代表从未发生),结果取各条目得分的均值,MARS-A≥4.5为药物依从性好. ...
1
... 临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测.为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训.检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频.检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比.参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍. ...
1
... 临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测.为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训.检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频.检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比.参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍. ...
1
... 临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测.为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训.检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频.检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比.参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍. ...
1
... 临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测.为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训.检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频.检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比.参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍. ...
1
... 临床访视时,由2位经验丰富的肺功能技师使用德国耶格公司肺功能仪(型号Master Screen)在复旦大学附属儿科医院肺功能实验室对研究对象进行检测.为确保检测过程的同质性,研究开始前建立标准操作手册,根据手册内容对2位技师再次培训.检测前一日通过微信公众号平台向患儿推送检测须知和宣教视频.检测结果由前期构建的肺功能诊断辅助系统自动导入专病数据库[14],包括1秒用力呼气容积(forced expiratory volume in one second,FEV1)占预计值百分比(FEV1%预计值),FEV1/用力肺活量(forced vital capacity,FVC)和用力呼出50%肺活量的呼气流量(forced expiratory flow at 50% of FVC exhaled,FEF50)、FEF75、FEF25-75占预计值百分比.参考美国胸科学会指南和中华医学会儿科学分会呼吸学组肺功能协作组儿童肺功能指南[15-16],以FEV1%预计值<80%且FEV1/FVC<80%诊断为阻塞性肺通气功能障碍,FEF50、FEF75和FEF25-75占预计值百分比中任意2项小于65%诊断为小气道功能障碍. ...



{kind=link}
{kind=link}