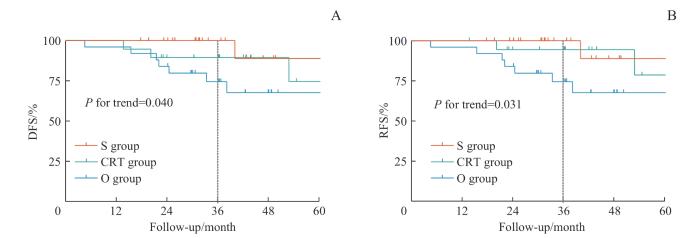
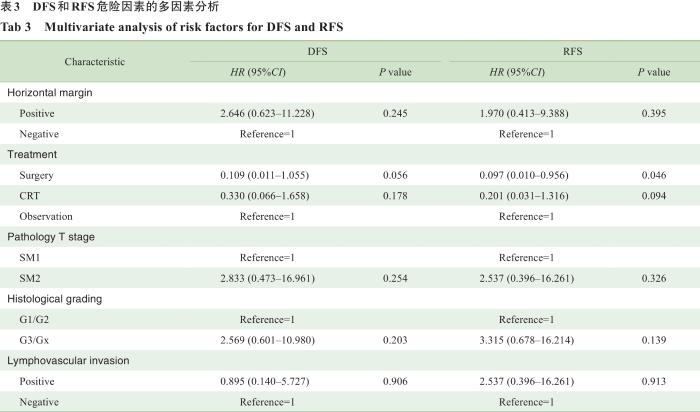
Objective ·To compare the prognostic effects of radical resection of esophageal cancer, concurrent chemoradiotherapy and simple follow-up observation on the prognosis of patients with T1b invasion of superficial esophageal squamous cell carcinoma after endoscopic submucosal dissection (ESD). Methods ·From May 2016 to May 2021, the clinical data of 67 patients with esophageal squamous cell carcinoma who were pathologically confirmed as pT1b after ESD and treated in Shanghai Chest Hospital were retrospectively analyzed. According to the additional treatment after ESD, the patients were divided into additional surgery group (S group), chemoradio-therapy group (CRT group) and observation group (O group). χ2 test was used to compare the clinical baseline data and pathological information of the three groups of patients. The Kaplan-Meier survival curve and log-rank test were used to compare the disease free survival (DFS) and recurrence free survival (RFS) of the three groups of patients, and the Cox proportional hazards regression model was used on DFS and RFS by univariate and multivariate analysis. Results ·Among all 67 patients, there were 23 cases in the S group, 19 cases in the CRT group, and 25 cases in the O group. There was no significant difference in age (P=0.080), gender (P=0.078), tumor length (P=0.485), tumor location (P=0.655), lesion circumferential ratio (P=0.310), histological grading (P=0.084), depth of tumor invasion (P=0.066) and lymphovascular invasion (P=0.279) among the three groups. During (42.6±16.7) months of follow-up, tumor recurrence was observed in 10 cases (14.9%), including 6 patients (60%) with local recurrence, 2 patients (20%) with regional lymph recurrence and 2 patients (20%) with distant metastasis. The median recurrence time of group S, group CRT, and group O was 40.1, 36.6, and 22.1 months, and the 3-year DFSs were 100%, 89.5%, and 74.5% (P-trend=0.040). Multivariate Cox analysis showed that additional esophagectomy was the key to improving independent protective factors of RFS (HR=0.097, 95%CI 0.010‒0.956, P=0.046). Conclusion ·For patients with superficial esophageal squamous cell carcinoma confirmed as pT1b after ESD, additional surgery can significantly reduce the possibility of long-term recurrence.
ZHU Kaiyuan, SU Yuchen, LIU Zhichao, ZHANG Hong, LI Chunguang, ZHANG Jie, LI Zhigang. Adjuvant strategies for patients with T1b invasion after endoscopic submucosal dissection for esophageal squamous cell carcinoma. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(1): 116-123 doi:10.3969/j.issn.1674-8115.2024.01.013
The study was designed by ZHU Kaiyuan and LI Zhigang. Clinical and survival data was collected by ZHU Kaiyuan, SU Yuchen, ZHANG Hong, LI Chunguang and ZHANG Jie. Data was analyzed by ZHU Kaiyuan. The manuscript was drafted and revised by ZHU Kaiyuan, SU Yuchen, LIU Zhichao and LI Zhigang. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249.
IGAKI H, KATO H, TACHIMORI Y, et al. Clinicopathologic characteristics and survival of patients with clinical Stage I squamous cell carcinomas of the thoracic esophagus treated with three-field lymph node dissection[J]. Eur J Cardiothorac Surg, 2001, 20(6): 1089-1094.
KITAGAWA Y, ISHIHARA R, ISHIKAWA H, et al. Esophageal cancer practice guidelines 2022 edited by the Japan esophageal society: part 1[J]. Esophagus, 2023, 20(3): 343-372.
TAJIMA Y, NAKANISHI Y, TACHIMORI Y, et al. Significance of involvement by squamous cell carcinoma of the ducts of esophageal submucosal glands. Analysis of 201 surgically resected superficial squamous cell carcinomas[J]. Cancer, 2000, 89(2): 248-254.
BOLLSCHWEILER E, BALDUS S E, SCHRÖDER W, et al. High rate of lymph-node metastasis in submucosal esophageal squamous-cell carcinomas and adenocarcinomas[J]. Endoscopy, 2006, 38(2): 149-156
NEWTON A D, PREDINA J D, XIA L L, et al. Surgical management of early-stage esophageal adenocarcinoma based on lymph node metastasis risk[J]. Ann Surg Oncol, 2018, 25(1): 318-325.
KITAGAWA Y, ISHIHARA R, ISHIKAWA H, et al. Esophageal cancer practice guidelines 2022 edited by the Japan Esophageal Society: part 2[J]. Esophagus, 2023, 20(3): 373-389.
Bureau of Medical Administration, National Health Commission of the People′s Republic of China. Standardization for diagnosis and treatment of esophageal cancer (2022 edition)[J]. Chinese Journal of Digestive Surgery, 2022, 21(10): 1247-1268.
KATO H, SATO A, FUKUDA H, et al. A phase Ⅱ trial of chemoradiotherapy for stage I esophageal squamous cell carcinoma: Japan clinical oncology group study (JCOG9708)[J]. Jpn J Clin Oncol, 2009, 39(10): 638-643.
KATO K, ITO Y, NOZAKI I, et al. Parallel-group controlled trial of surgery versus chemoradiotherapy in patients with stage I esophageal squamous cell carcinoma[J]. Gastroenterology, 2021, 161(6): 1878-1886.e2.
FAN X, WANG J, XIA L, et al. Efficacy of endoscopic therapy for T1b esophageal cancer and construction of prognosis prediction model: a retrospective cohort study[J]. Int J Surg, 2023, 109(6): 1708-1719.
NAKAJO K, ABE S, ODA I, et al. Impact of the Charlson Comorbidity Index on the treatment strategy and survival in elderly patients after non-curative endoscopic submucosal dissection for esophageal squamous cell carcinoma: a multicenter retrospective study[J]. J Gastroenterol, 2019, 54(10): 871-880.
RICE T W, ISHWARAN H, FERGUSON M K, et al. Cancer of the esophagus and esophagogastric junction: an eighth edition staging primer[J]. J Thorac Oncol, 2017, 12(1): 36-42.
JOSEPH A, DRAGANOV P V, MALUF-FILHO F, et al. Outcomes for endoscopic submucosal dissection of pathologically staged T1b esophageal cancer: a multicenter study[J]. Gastrointest Endosc, 2022, 96(3): 445-453.
REZA J A, RAMAN V, VEKSTEIN A, et al. Implementation of staging guidelines in early esophageal cancer: a study of the society of thoracic surgeons general thoracic surgery database[J]. Ann Surg, 2023, 278(4): e754-e759.
KRILL T, BALISS M, ROARK R, et al. Accuracy of endoscopic ultrasound in esophageal cancer staging[J]. J Thorac Dis, 2019, 11(suppl 12): S1602-S1609.
MOTOYAMA S, JIN M, MATSUHASHI T, et al. Outcomes of patients receiving additional esophagectomy after endoscopic resection for clinically mucosal, but pathologically submucosal, squamous cell carcinoma of the esophagus[J]. Surg Today, 2013, 43(6): 638-642.
IKEDA A, HOSHI N, YOSHIZAKI T, et al. Endoscopic submucosal dissection (ESD) with additional therapy for superficial esophageal cancer with submucosal invasion[J]. Intern Med, 2015, 54(22): 2803-2813.
SAEKI H, WATANABE M, MINE S, et al. Esophagectomy for superficial esophageal cancer after non-curative endoscopic resection[J]. J Gastroenterol, 2015, 50(4): 406-413.
MÖNIG S, CHEVALLAY M, NICLAUSS N, et al. Early esophageal cancer: the significance of surgery, endoscopy, and chemoradiation[J]. Ann N Y Acad Sci, 2018, 1434(1): 115-123.
KADOTA T, MINASHI K, WAKABAYASHI M, et al. Diagnostic yield of conventional endoscopy with endoscopic ultrasonography for submucosal invasion of superficial esophageal squamous cell carcinoma: a post hoc analysis of multicenter prospective confirmatory study (JCOG0508)[J]. Esophagus, 2021, 18(3): 604-611.
NIHEI K, MINASHI K, YANO T, et al. Final analysis of diagnostic endoscopic resection followed by selective chemoradiotherapy for stage I esophageal cancer: jcog0508[J]. Gastroenterology, 2023, 164(2): 296-299.e2.
MIYAZAKI T, MYOJIN M, HOSOKAWA M, et al. Endoscopic resection as an independent predictive factor of local control in patients with T1bN0M0 esophageal squamous cell carcinoma treated with chemoradiotherapy: a retrospective study[J]. Radiat Oncol, 2022, 17(1): 11.
SONG B G, KIM G H, CHO C J, et al. Close observation versus additional surgery after noncurative endoscopic resection of esophageal squamous cell carcinoma[J]. Dig Surg, 2021, 38(3): 247-254.
TANAKA T, UENO M, IIZUKA T, et al. Comparison of long-term outcomes between esophagectomy and chemoradiotherapy after endoscopic resection of submucosal esophageal squamous cell carcinoma[J]. Dis Esophagus, 2019, 32(12): doz023.
NAITO S, YOSHIO T, ISHIYAMA A, et al. Long-term outcomes of esophageal squamous cell carcinoma with invasion depth of pathological T1a-muscularis mucosae and T1b-submucosa by endoscopic resection followed by appropriate additional treatment[J]. Dig Endosc, 2022, 34(4): 793-804.
AKUTSU Y, KATO K, IGAKI H, et al. The prevalence of overall and initial lymph node metastases in clinical T1N0 thoracic esophageal cancer: from the results of JCOG0502, a prospective multicenter study[J]. Ann Surg, 2016, 264(6): 1009-1015.
HOLYOAKE D L P, SMYTH E C. Chemoradiotherapy or surgery for very early esophageal squamous cancer: can a nonrandomized trial give us the answer?[J]. Gastroenterology, 2021, 161(6): 1793-1795.
YANG Y, SU Y, ZHANG X, et al. Esophagectomy versus definitive chemoradiotherapy for patients with clinical stage N0 and pathological stage T1b esophageal squamous cell carcinoma after endoscopic submucosal dissection: study protocol for a multicenter randomized controlled trial (Ad-ESD Trial)[J]. Trials, 2020, 21(1): 603.



{kind=link}
{kind=link}