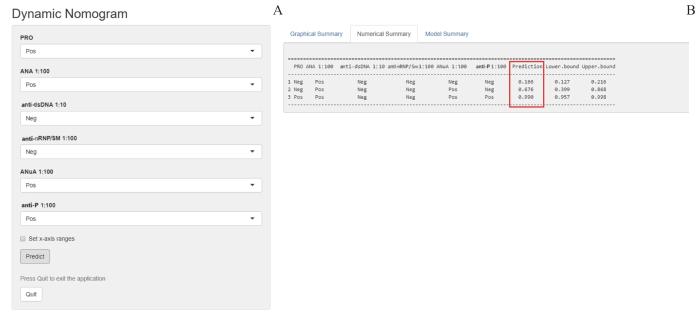
Objective ·To establish a nomogram for the differential diagnosis of early systemic lupus erythematosus (SLE) and other autoimmune diseases based on laboratory indications, and to evaluate its efficacy. Methods ·A total of 535 SLE patients admitted to the First Hospital of Lanzhou University from January 2017 to December 2021 were selected as SLE group, and 535 patients with other autoimmune diseases during the same period were selected as control group. Basic information and laboratory test indicators of the SLE group and control group were collected and compared. The SLE group and control group were randomly assigned to the training set and the validation set at a ratio of 7∶3, respectively. LASSO regression method and multivariate Logistic regression were used to select the main risk factors of SLE. The nomogram for differential diagnosis of early SLE (SLE nomogram) was established according to the selected main risk factors. Bootstrap method was used to conduct internal repeated sampling for 1 000 times to calibrate the nomogram. The receiver operator characteristic curve (ROC curve) and decision curve analysis (DCA) were performed to evaluate the differential diagnosis ability and the value in clinical application of SLE nomogram, respectively. The "DynNom" package of R language was used to convert the nomogram into an electronic calculator, and its consistency with SLE nomogram was verified by data from 3 groups of patients. Results ·LASSO regression and multivariate Logistic regression identified six major risk factors for SLE, including antinuclear antibody (ANA), anti-double-stranded DNA (anti-dsDNA) antibody, anti-ribonucleoprotein antibody/anti-Simth antibody (anti-nRNP/Sm), anti-ribosomal P protein (anti-P) antibody, anti-nucleosome antibody (ANuA) and urinary protein (PRO), which were used to construct the SLE nomogram. The calibration curve of the SLE nomogram had standard errors of 0.009 and 0.015 in the training set and validation set, respectively, and its area under the curve (AUC) was 0.889 and 0.869, respectively. The results of DCA showed that when the risk threshold of SLE nomogram was 0.15‒0.95, the model achieved more net benefit. The prediction results of the electronic calculator showed that when ANA (titer 1∶100) was positive in SLE patient No.1, the prevalence was 0.166; when both ANA (titer 1∶100) and ANuA (titer 1∶100) were positive in patient No.2, the prevalence was 0.676; when all of PRO, ANA (titer 1∶100), ANuA (titer 1∶100) and anti-P antibody (titer 1∶100) were positive in patient No.3, the prevalence was 0.990, which was consistent with the differential diagnosis results of the SLE nomogram. Conclusion ·The established SLE nomogram based on ANA, anti-dsDNA antibody, anti-nRNP/Sm, anti-P antibody, ANuA and PRO and its conversion into an electronic calculator can effectively distinguish early SLE from other autoimmune diseases, and have important clinical application value.
YANG Jingyu, CHEN Liubao, WANG Kangtai, YANG Xingzhi, YU Haitao. Establishment and evaluation of nomogram for differential diagnosis of systemic lupus erythematosus based on laboratory indications. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(2): 204-211 doi:10.3969/j.issn.1674-8115.2024.02.006
检查2组患者基本信息、实验室指标等的完整性,对于缺失率<30%的实验室指标,使用链式方程多重插补(multiple imputation by chained equation,MICE)法对其进行5次计算,取平均值后用于填充缺失指标的信息[16-17],并分析填充前后的数据分布,证实数据结构未发生变化以开展后续分析。同时,将SLE组定义为“1”、对照组定义为“0”,实验室定性指标的阴性结果定义为“0”、阳性结果定义为“1”,用于后续构建列线图。
通过Bootstrap法对训练集、验证集患者的实验室指标进行1 000次的随机重复抽样,并利用校准曲线对列线图进行内部验证。采用受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)及其曲线下面积(area under the curve,AUC)评估该列线图鉴别诊断SLE与其他自身免疫性疾病的价值[21]。使用决策曲线分析(decision curve analysis,DCA)评估该列线图在临床应用中的价值[22]。
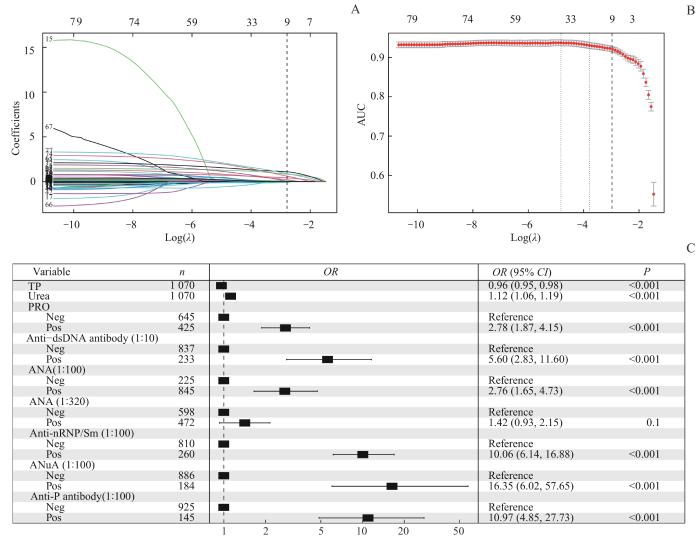
Note: A. LASSO coefficient curves for 79 indicators according to log(λ). The colored lines represent the influence of λ value in the model on the weight coefficients of different indicators. The dashed line represents the best λ value and its number of indicators. B. Selection of the indicators by LASSO at the optimal parameter (λ). C. Multivariate Logistic regression analysis of major risk indicators. TP—total protein; Pos—positive; Neg—negative.
Fig 1
Selection of major risk indicators related to SLE
Tab 1
表1
表1训练集和验证集患者的6项SLE主要危险因子比较
Tab 1 Comparison of six major risk factors for SLE in patients between training set and validation set
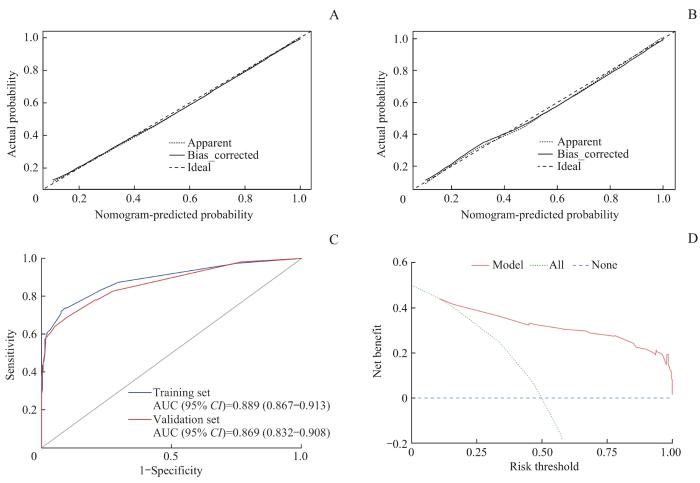
Note: A. Calibration curve of the training set. B. Calibration curve of the validation set. C. ROC curve of the training set and validation set. D. DCA curve of the training set.
Fig 3
Performance verification of nomogram for differential diagnosis of SLE
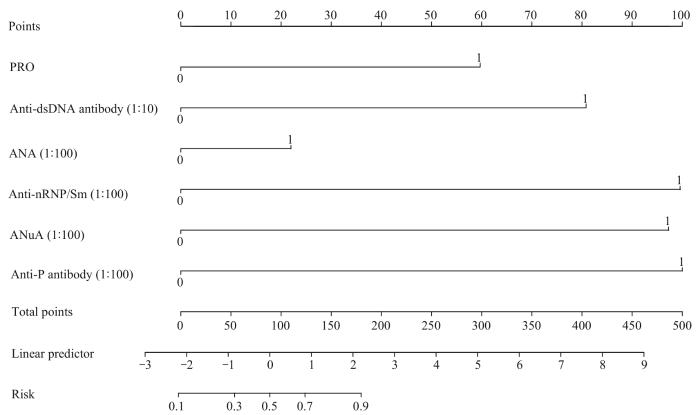
目前,SLE的诊断和鉴别诊断主要根据2019年欧洲抗风湿病联盟联合美国风湿病学会共同发布的系统性红斑狼疮分类标准(2019 European League Against Rheumatism/American College of Rheumatology Systemic Lupus Erythematosus Classification Criteria,2019 EULAR/ACR criteria),并通过其中的症状和实验室指标进行诊断。该标准是由ANA以及21种症状和体征组成的积分表,在ANA滴度≥1∶80、总评分≥10分且排除其他可能的诊断后即可被确诊为SLE。由于该标准涉及的内容较多,临床上使用较为烦琐;而早期SLE症状缺乏特异性,且其与其他自身免疫性疾病间存在相似的体征,这又为早期SLE的鉴别诊断带来了困难。在本研究中,我们根据SLE主要危险因子的作用权重建立了SLE列线图,可通过患者的实验室检查结果直接计算出其患病风险;这不仅为临床工作提供了便利,还可较好地实现早期SLE与其他自身免疫性疾病的鉴别诊断,解决了早期SLE的漏诊和误诊问题。本研究通过LASSO和多因素Logistic回归筛选出SLE的6项主要危险因子,并由该6项建立了早期SLE鉴别诊断的列线图。该列线图在训练集和验证集的AUC分别为0.889和0.869,提示该列线图可较好地鉴别早期SLE和其他自身免疫性疾病,即具有良好的鉴别诊断能力。而后,我们将列线图转换成电子计算器,以更加方便、快捷地评估SLE的患病率,从而为进一步实现临床转化应用奠定了基础。
The study was designed by YU Haitao. The manuscript was drafted and revised by YU Haitao and YANG Jingyu. The data were analyzed by YU Haitao and YANG Jingyu. The data were collected and organized by YANG Jingyu, CHEN Liubao, WANG Kangtai and YANG Xingzhi. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
ROSE J. Autoimmune connective tissue diseases: systemic lupus erythematosus and rheumatoid arthritis[J]. Emerg Med Clin North Am, 2022, 40(1): 179-191.
IQBAL S, SHER M R, GOOD R A, et al. Diversity in presenting manifestations of systemic lupus erythematosus in children[J]. J Pediatr, 1999, 135(4): 500-505.
CHOWDHARY V R, CROWSON C S, POTERUCHA J J, et al. Liver involvement in systemic lupus erythematosus: case review of 40 patients[J]. J Rheumatol, 2008, 35(11): 2159-2164.
YANG Z X, REN Y P, LIU D H, et al. Prevalence of systemic autoimmune rheumatic diseases and clinical significance of ANA profile: data from a tertiary hospital in Shanghai, China[J]. APMIS, 2016, 124(9): 805-811.
MARTORELL-MARUGÁN J, CHIERICI M, JURMAN G, et al. Differential diagnosis of systemic lupus erythematosus and Sjögren's syndrome using machine learning and multi-omics data[J]. Comput Biol Med, 2023, 152: 106373.
WALLACE D J, GAVIN I M, KARPENKO O, et al. Cytokine and chemokine profiles in fibromyalgia, rheumatoid arthritis and systemic lupus erythematosus: a potentially useful tool in differential diagnosis[J]. Rheumatol Int, 2015, 35(6): 991-996.
LIU H H, PAN F M, CHEN L W. Value of antinucleosome antibody and anti-Sm antibody in the differential diagnosis of systemic lupus erythematosus: a meta-analysis[J]. Journal of Modern Laboratory Medicine, 2021, 36(3): 1-6, 31.
LEE J H, YOON Y C, JIN W, et al. Development and validation of nomograms for malignancy prediction in soft tissue tumors using magnetic resonance imaging measurements[J]. Sci Rep, 2019, 9(1): 4897.
CHEN W, WANG B, ZENG R, et al. Development and validation of a nomogram for the estimation of response to platinum-based neoadjuvant chemotherapy in patients with locally advanced cervical cancer[J]. Cancer Manag Res, 2021, 13: 1279-1289.
BALACHANDRAN V P, GONEN M, SMITH J J, et al. Nomograms in oncology: more than meets the eye[J]. Lancet Oncol, 2015, 16(4): e173-e180.
HOCHBERG M C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus[J]. Arthritis Rheum, 1997, 40(9): 1725.
PETRI M, ORBAI A M, ALARCÓN G S, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus[J]. Arthritis Rheum, 2012, 64(8): 2677-2686.
LAQUEUR H S, SHEV A B, KAGAWA R M C. SuperMICE: an ensemble machine learning approach to multiple imputation by chained equations[J]. Am J Epidemiol, 2022, 191(3): 516-525.
WANG Y Q, WANG L X, SUN Y L, et al. Prediction model for the risk of osteoporosis incorporating factors of disease history and living habits in physical examination of population in Chongqing, Southwest China: based on artificial neural network[J]. BMC Public Health, 2021, 21(1): 991.
SAUERBREI W, ROYSTON P, BINDER H. Selection of important variables and determination of functional form for continuous predictors in multivariable model building[J]. Stat Med, 2007, 26(30): 5512-5528.
MEHER P K, RAI A, RAO A R. mLoc-mRNA: predicting multiple sub-cellular localization of mRNAs using random forest algorithm coupled with feature selection via elastic net[J]. BMC Bioinformatics, 2021, 22(1): 342.
SHANG X Y, REN L S, SUN G R, et al. Anti-dsDNA, anti-nucleosome, anti-C1q, and anti-histone antibodies as markers of active lupus nephritis and systemic lupus erythematosus disease activity[J]. Immun Inflamm Dis, 2021, 9(2): 407-418.
JIANG B, XU Z Z, JIANG Z Z, et al. Diagnostic significance of three autoantibodies and complement C3 levels in patients with lupus nephritis[J]. West China Medical Journal, 2016, 31(2): 309-311.
CHEN Q L, LI J, QIU F, et al. Olfactory function and related factors in systemic lupus erythematosus[J]. Chinese Journal of Rheumatology, 2014, 18(6): 408-410.
REN Y M. The clinical diagnostic value of antinuclear antibody combined with antinuclear antibody spectrum in systemic lupus erythematosus[J]. Chinese Journal of Modern Drug Application, 2021, 15(4): 70-72.
WANG Y P, ZOU L, GUO T, et al. The clinical value of anti-ribosomal P protein, anti-Smith, anti-dsDNA, anti-nucleosome and anti-histone antibodies for systemic lupus erythematosus[J]. Current Immunology, 2021, 41(5): 353-360, 379.
ESTÉVEZ DEL TORO M, VARELA CEBALLOS I, CHICO CAPOTE A, et al. Predictive factors for the development of lupus nephritis after diagnosis of systemic lupus erythematosus[J]. Reumatol Clin (Engl Ed), 2022, 18(9): 513-517.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}