Objective ·To evaluate the relationship between body mass index (BMI) and chronic metabolic diseases. Methods ·The elderly (≥60 years old) who were underwent physical examination in the Physical Examination Center of Renji Hospital, Shanghai Jiao Tong University School of Medicine from 2014 to 2021 were studied. Their results of biochemical indicators were collected. Their height, body weight, and blood pressure were measured by trained nurses. The history of chronic metabolic diseases was collected by self-reported questionnaire. Systolic blood pressure ≥140 mmHg (1 mmHg=0.133 kPa), diastolic blood pressure ≥90 mmHg, or self-reported hypertension history was defined as hypertension. Fasting blood glucose ≥7.0 mmol/L or self-reported history of diabetes was defined as diabetes. Total cholesterol≥6.2 mmol/L, triglyceride≥2.3 mmol/L, or self-reported history of dyslipidemia was defined as dyslipidemia. The relationship between BMI and hypertension, diabetes, and dyslipidemia was evaluated by using receiver operator characteristic (ROC) curve analysis and binary logistic regression. Results ·Data of 59 083 subjects were collected [30 807 men and 28 276 women, average age: (67.9±6.3) years old]. The prevalence of hypertension, diabetes and dyslipidemia was 76.5% (45 219/59 083), 24.1% (14 225/59 083) and 50.0% (29 544/59 083), respectively. Compared to the elderly people aged 60‒74 years, those aged 75 years and above had a higher proportion of hypertension and diabetes, and a lower proportion of dyslipidemia and no metabolic abnormalities. With ROC analysis, the BMI cut-off values for hypertension, diabetes, and dyslipidemia were 24.3, 23.9, and 23.9 kg/m2. The BMI cut-off values for hypertension and diabetes in elderly men were similar to those in elderly women (for hypertension: 24.3 kg/m2 in elderly men vs 24.2 kg/m2 in elderly women; for diabetes: 24.0 kg/m2 in elderly men vs 23.7 kg/m2 in elderly women); however, BMI cut-off value for dyslipidemia was obviously higher in elderly men than that in elderly women (24.0 kg/m2 in elderly men vs 22.5 kg/m2 in elderly women). The BMI cut-off value for chronic metabolic diseases was higher in the elderly people aged 60‒74 years than that in the elderly people aged 75 years and above (24.2‒24.7 kg/m2vs 22.9‒23.8 kg/m2). Conclusion ·Elderly people aged 60‒74 years should maintain the BMI below 24.0 kg/m2, while those aged 75 years and above should aim for the BMI below 23.0 kg/m2, so as to reduce the risk of chronic metabolic diseases.
Keywords:body mass index (BMI)
;
chronic metabolic disease
;
elderly
JIANG Ying, LI Qingyao, CHEN Zhiqi, WANG Jialu, LI Yun, XU Renying. Association between body mass index and chronic metabolic diseases in Chinese aged population. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(2): 250-257 doi:10.3969/j.issn.1674-8115.2024.02.011
采用SAS 9.3软件进行分析。符合正态分布的定量资料以x±s表示,组间比较采用方差分析;不符合正态分布的定量资料以M(Q1,Q3)表示,组间比较采用两独立样本非参数检验。定性资料以频数(百分率)表示,组间比较采用卡方检验。采用二元Logistic回归分析BMI与高血压、糖尿病和脂质代谢紊乱之间的关系,通过受试者操作特征(receiver operator characteristic,ROC)曲线的切点值、敏感度、特异度、曲线下面积(area under the curve,AUC)对模型区分结果进行比较。P<0.05表示差异具有统计学意义。
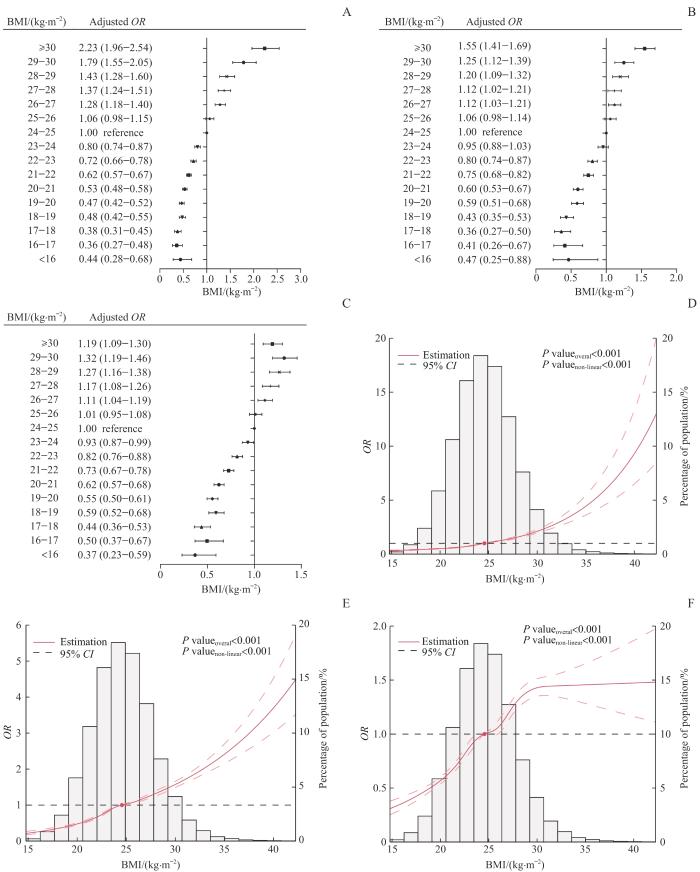
Note:A‒C. Binary Logistic regression results of BMI with hypertension (A), diabetes (B), and hyperlipoidemia (C). The controlled variables included age, gender, ALT, AST, and eGFR. When analyzing the relationship between BMI and hypertension, further control was applied for FBG, TC, and TAG. When analyzing the relationship between BMI and diabetes, further control was applied for SBP, DBP, TC, and TAG. When analyzing the relationship between BMI and hyperlipoidemia, further control was applied for SBP, DBP, and FBG. D‒F. Restricted cubic spline results of BMI with hypertension (D), diabetes (E), and hyperlipoidemia (F). The controlled variables included age and gender, and the reference value for BMI was 24.56 kg/m2.
Fig 1
Relationship between BMI and chronic metabolic diseases
The study was designed by JIANG Ying, LI Qingyao, CHEN Zhiqi, LI Yun and XU Renying. The manuscript was drafted and revised by JIANG Ying, LI Qingyao, WANG Jialu and XU Renying. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
XIONG Y, ZHANG Y C, ZHANG F X, et al. Prevalence and associated factors of metabolic syndrome in Chinese middle-aged and elderly population: a national cross-sectional study[J]. Aging Male, 2021, 24(1): 148-159.
GE H S, YANG Z H, LI X Y, et al. The prevalence and associated factors of metabolic syndrome in Chinese aging population[J]. Sci Rep, 2020, 10(1): 20034.
ZHOU B F, Cooperative Meta-analysis Group of the Working Group on Obesity in China. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults: study on optimal cut-off points of body mass index and waist circumference in Chinese adults[J]. Biomed Environ Sci, 2002, 15(1): 83-96.
YORKE E, TETTEH J, BOIMA V, et al. High BMI: an important health risk factor among older adults in Ghana[J]. Public Health Nutr, 2021, 24(14): 4522-4529.
ZHANG W L, HE K, ZHAO H, et al. Association of body mass index and waist circumference with high blood pressure in older adults[J]. BMC Geriatr, 2021, 21(1): 260.
WANG S K, MA W, WANG S M, et al. Obesity and its relationship with hypertension among adults 50 years and older in Jinan, China[J]. PLoS One, 2014, 9(12): e114424.
WANG J, TAYLOR A W, ZHANG T, et al. Association between body mass index and all-cause mortality among oldest old Chinese[J]. J Nutr Health Aging, 2018, 22(2): 262-268.
BHASKARAN K, DOS-SANTOS-SILVA I, LEON D A, et al. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3.6 million adults in the UK[J]. Lancet Diabetes Endocrinol, 2018, 6(12): 944-953.
JAVED A A, MA J H, ANDERSON L N, et al. Age-appropriate BMI cut-points for cardiometabolic health risk: a cross-sectional analysis of the Canadian Longitudinal Study on Aging[J]. Int J Obes (Lond), 2022, 46(5): 1027-1035.
JAFARINASABIAN P, INGLIS J E, REILLY W, et al. Aging human body: changes in bone, muscle and body fat with consequent changes in nutrient intake[J]. J Endocrinol, 2017, 234(1): R37-R51.
GRAF C E, KARSEGARD V L, SPOERRI A, et al. Body composition and all-cause mortality in subjects older than 65 y[J]. Am J Clin Nutr, 2015, 101(4): 760-767.
ANDERS H J, HUBER T B, ISERMANN B, et al. CKD in diabetes: diabetic kidney disease versus nondiabetic kidney disease[J]. Nat Rev Nephrol, 2018, 14(6): 361-377.
Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition)[J]. Chinese Journal of Diabetes Mellitus, 2021, 13(4): 315-409.
Joint Committee Issued Chinese Guideline for the Management of Dyslipidemia in Adults. 2016 Chinese guideline for the management of dyslipidemia in adults[J]. Chinese Journal of Cardiology, 2016, 44(10): 833-853.
Hypertension Branch of Chinese Geriatrics Society, National Clinical Research Center for Geriatric Diseases-Chinese Alliance of Geriatric Cardiovascular Disease. 2019 Chinese guidelines for the management of hypertension in the elderly[J]. Chinese Journal of Cardiovascular Medicine, 2019, 24(1):1-23.
CHEN Y J, LIANG X, ZHENG S S, et al. Association of body fat mass and fat distribution with the incidence of hypertension in a population-based Chinese cohort: a 22-year follow-up[J]. J Am Heart Assoc, 2018, 7(6): e007153.
BADR H E, SHAH N M, SHAH M A. Obesity among Kuwaitis aged 50 years or older: prevalence, correlates, and comorbidities[J]. Gerontologist, 2013, 53(4): 555-566.
RAHMAN M, ZAMAN M M, ISLAM J Y, et al. Prevalence, treatment patterns, and risk factors of hypertension and pre-hypertension among Bangladeshi adults[J]. J Hum Hypertens, 2018, 32(5): 334-348.
HSU C H, LIN J D, HSIEH C H, et al. Adiposity measurements in association with metabolic syndrome in older men have different clinical implications[J]. Nutr Res, 2014, 34(3): 219-225.
SEOK LEE H, PARK Y M, HAN K, et al. Obesity-related hypertension: findings from the Korea national health and nutrition examination survey 2008‒2010[J]. PLoS One, 2020, 15(4): e0230616.
DAS S, DEBNATH M, DAS S, et al. Association of overweight and obesity with hypertension, diabetes and comorbidity among adults in Bangladesh: evidence from nationwide Demographic and Health Survey 2017‒2018 data[J]. BMJ Open, 2022, 12(7): e052822.
SASAI H, SAIRENCHI T, ISO H, et al. Relationship between obesity and incident diabetes in middle-aged and older Japanese adults: the Ibaraki Prefectural Health Study[J]. Mayo Clin Proc, 2010, 85(1): 36-40.
EBRAHIMI H, EMAMIAN M H, HASHEMI H, et al. Dyslipidemia and its risk factors among urban middle-aged Iranians: a population-based study[J]. Diabetes Metab Syndr, 2016, 10(3): 149-156.
LIN H Q, WU J Y, CHEN M L, et al. Prevalence of dyslipidemia and prediction of 10-year CVD risk among older adults living in southeast coastal regions in China: a cross-sectional study[J]. Clin Interv Aging, 2019, 14: 1119-1129.
XI Y F, NIU L W, CAO N, et al. Prevalence of dyslipidemia and associated risk factors among adults aged ≥35 years in Northern China: a cross-sectional study[J]. BMC Public Health, 2020, 20(1): 1068.
VAN HEMELRIJCK M, ULMER H, NAGEL G, et al. Longitudinal study of body mass index, dyslipidemia, hyperglycemia, and hypertension in 60, 000 men and women in Sweden and Austria[J]. PLoS One, 2018, 13(6): e0197830.
PIKILIDOU M I, SCUTERI A, MORRELL C, et al. The burden of obesity on blood pressure is reduced in older persons: the SardiNIA study[J]. Obesity, 2013, 21(1): E10-E13.
CANNING K L, BROWN R E, JAMNIK V K, et al. Relationship between obesity and obesity-related morbidities weakens with aging[J]. J Gerontol A Biol Sci Med Sci, 2014, 69(1): 87-92.
CHENG F W, GAO X, MITCHELL D C, et al. Metabolic health status and the obesity paradox in older adults[J]. J Nutr Gerontol Geriatr, 2016, 35(3): 161-176.
BOWMAN K, DELGADO J, HENLEY W E, et al. Obesity in older people with and without conditions associated with weight loss: follow-up of 955, 000 primary care patients[J]. J Gerontol A Biol Sci Med Sci, 2017, 72(2): 203-209.
DI RENZO L, ITANI L, GUALTIERI P, et al. New BMI cut-off points for obesity in middle-aged and older adults in clinical nutrition settings in Italy: a cross-sectional study[J]. Nutrients, 2022, 14(22): 4848.
KUWABARA M, KUWABARA R, NIWA K, et al. Different risk for hypertension, diabetes, dyslipidemia, and hyperuricemia according to level of body mass index in Japanese and American subjects[J]. Nutrients, 2018, 10(8): 1011.



{kind=link}
{kind=link}