Predictive value of systemic immune inflammation index and somatic symptom scale-China in the occurrence of in-hospital major adverse cardiovascular events after first-episode of acute myocardial infarction undergoing PCI
ZHENG Mengyi,1, MAO Jialiang2, ZOU Zhiguo2, ZHANG Ruilei3, ZHANG Hou1, LI Shiguang,3
1.Graduate School of Bengbu Medical College, Bengbu 233030, China
2.Department of Cardiology, Renji Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200127, China
3.Department of Cardiology, The Second People′s Hospital of Anhui Province, Hefei 230041, China
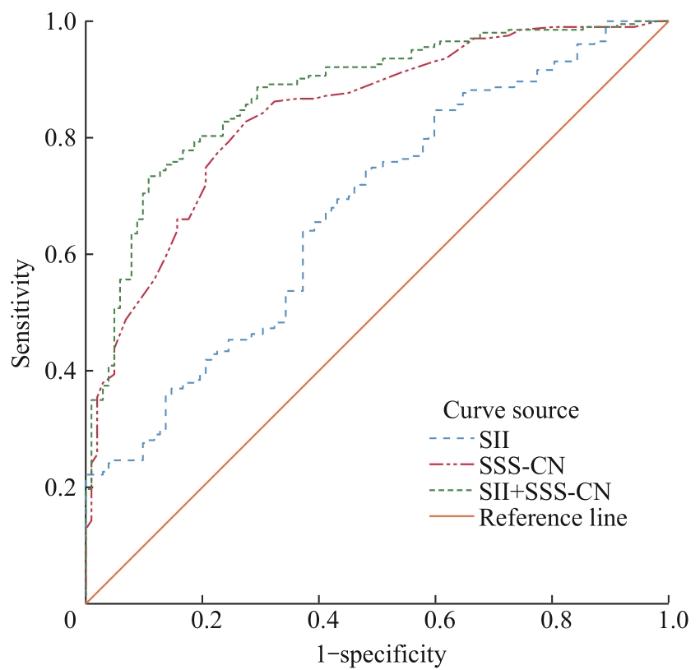
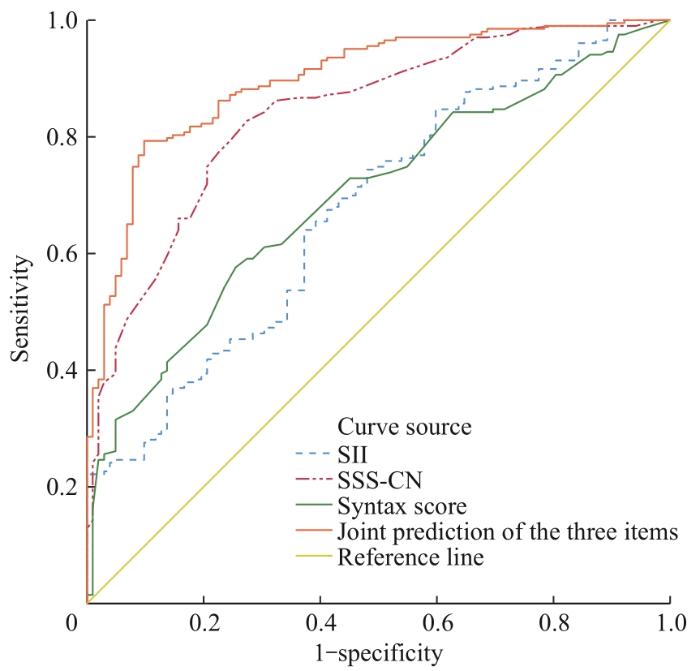
Objective ·To investigate the predictive value of systemic inflammatory index (SII) and somatization symptom score-China (SSS-CN) for major adverse cardiovascular events (MACEs) in patients with first-episode acute myocardial infarction (AMI) undergoing percutaneous coronary intervention (PCI). Methods ·Three hundred and five first-episode AMI patients who received PCI treatment at the Cardiology Department of Anhui Second People's Hospital from September 2021 to September 2023 were included in the study. Enrolled patients were divided into MACEs group (n=203) and non-MACEs group (n=102) based on whether MACEs events occurred during hospitalization. Descriptive statistical analysis was performed on the general data such as gender, age and laboratory test results of the two groups of patients, and binary Logistic regression test was conducted for statistically significant items according to the analysis results. According to the results, receiver operating characteristic (ROC) curves were further drawn to evaluate the value of SII and SSS-CN in predicting the occurrence of MACEs in hospital. On this basis, coronary syntax score (SS) was combined to evaluate the predictive efficacy of the three combinations, and the optimal cut-off value was determined according to the maximum Jordan index. Results ·A total of 203 patients had MACEs events, among whom 179 (88.1%) had heart failure, 16 (7.9%) had severe arrhythmia, 4 (2.0%) had shock, 2 (1.0%) had recurrent myocardial infarction, and 2 (1.0%) died. Compared with the non-MACEs group, the SII and SSS-CN scores in the MACEs group were significantly increased (1 925.86 vs 934.23, 38.57 vs 23.30; both P<0.05). The binary Logistic results suggested that both SII and SSS-CN were independent risk factors for the occurrence of MACEs. The ROC curve results showed that the prediction efficiency was the best when SII ≥ 952, with a sensitivity of 64.0% and a specificity of 62.7% (AUC 0.675, 95% CI 0.612‒0.737). The prediction efficiency was the best when SSS-CN ≥ 28.5, with a sensitivity of 80.7% and a specificity of 77.5% (AUC 0.840, 95% CI 0.794‒0.886). The predictive performance was further improved after combining the syntax score (AUC 0.898, 95% CI 0.862‒0.933). Conclusion ·The admission SII and SSS-CN scores of first-episode AMI patients are independent risk factors for the occurrence of MACEs during hospitalization after PCI. Early monitoring of SII changes in first-episode AMI patients after PCI or SSS-CN scores for patients with obvious Somatization symptoms can help identify high-risk patients for the occurrence of MACEs in the hospital.
Keywords:systemic immune inflammation index (SII)
;
somatization symptom score-China (SSS-CN)
;
first episode of acute myocardial infarction
;
major adverse cardiovascular event (MACE)
;
percutaneous coronary intervention (PCI)
ZHENG Mengyi, MAO Jialiang, ZOU Zhiguo, ZHANG Ruilei, ZHANG Hou, LI Shiguang. Predictive value of systemic immune inflammation index and somatic symptom scale-China in the occurrence of in-hospital major adverse cardiovascular events after first-episode of acute myocardial infarction undergoing PCI. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(3): 334-341 doi:10.3969/j.issn.1674-8115.2024.03.005
ZHENG Mengyi designed the study and wrote the manuscript. ZHANG Ruilei and ZHANG Hou collected data and performed the statistical analysis. MAO Jialiang, ZOU Zhiguo, and LI Shiguang participated in the revision of the paper. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
The Joint Task Force for Guideline on the Assessment and Management of Cardiovascular Risk in China. Guideline on the assessment and management of cardiovascular risk in china[J]. Chinese Circulation Journal, 2019, 34(1): 4-28
HAO M H, GUO M, TANG Y, et al. Serum REG level after PCI and its relationship with prognosis in patients with acute ST-segment elevation myocardial infarction[J]. Advances in Cardiovascular Diseases, 2020, 41(1): 102-106.
ESENBOĞA K, KURTUL A, YAMANTÜRK Y Y, et al. Systemic immune-inflammation index predicts no-reflow phenomenon after primary percutaneous coronary intervention[J]. Acta Cardiol, 2022, 77(1): 59-65.
HU B, YANG X R, XU Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma[J]. Clin Cancer Res, 2014, 20(23): 6212-6222.
SAYLIK F, AKBULUT T. Systemic immune-inflammation index predicts major cardiovascular adverse events in patients with ST-segment elevated myocardial infarction[J]. Arq Bras Cardiol, 2022, 119(1):14-22.
WANG Z, QIN Z, YUAN R, et al. Systemic immune-inflammation index as a prognostic marker for advanced chronic heart failure with renal dysfunction[J]. ESC Heart Fail, 2023, 10(1): 478-491.
HE X H, JIA Y D, ZHAI H J, et al. Relationship between novel inflammatory markers and prognosis in patients with acute myocardial infarction after coronary intervention[J]. Journal of Cardiovascular and Pulmonary Diseases, 2023, 42(7): 656-661.
ROSENGREN A, HAWKEN S, OUNPUU S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study[J]. Lancet, 2004, 364(9438): 953-962.
CHEN B X, HAN Y, FENG M T, et al. Investigation and analysis of somatic symptoms disorder, anxiety and depression in patients with acute myocardial infarction and patients with negative coronary angiography[J]. Chinese Journal of Evidence-Based Cardiovascular Medicine, 2021, 13(2): 154-161.
XU F, LU H, QI Y. Analysis on somatization symptoms and anxiety and depression status in patients with acute myocardial infarction following emergency percutaneous coronary intervention[J]. Chinese Community Doctors,2022, 38(3): 34-36.
Chinese Society of Cardiology, Editorial Office of Chinese Journal of Cardiology, Editorial Office of Chinese Circulation Journal. Guidelines for the diagnosis and treatment of acute myocardial infarction[J]. Chinese Journal of Cardiology, 2001, 29(12): 710-725.
Cardiovascular Rehabilitation Branch-Chinese Association of Rehabilitation Medicine, China Committee of Cardio-Cerebral-Vascular Diseases of GSC. China expert consensus on psychological prescription for patients with cardiovascular disease[J]. Chinese Journal of Cardiology, 2014, 42(1): 6-13.
Neuropsychology and Behavioral Neurology Group, Neurology Branch, Chinese Medical Association. Expert consensus on diagnosis and treatment of anxiety, depression, and somatization symptoms in general hospitals[J]. Chinese Journal of Neurology, 2016, 49(12): 908-917.
HU J Y, CHEN B X, MAO J L, et al. Investigation on somatization symptoms, anxiety, and depression in patients visiting cardiology department[J]. Preventive Medicine, 2019, 31(12): 1241-1244.
HUSSER O, BODI V, SANCHIS J, et al. White blood cell subtypes after STEMI: temporal evolution, association with cardiovascular magnetic resonance-derived infarct size and impact on outcome[J]. Inflammation, 2011, 34(2): 73-84.
SONG L Y. Predictive value of systemic immune-inflammation index combined with modified shock index in patients with STEMI for in-hospital mace after primary PCI[D]. Changchun: Jilin University, 2023.
PARK J S, SEO K W, CHOI B J, et al. Importance of prognostic value of neutrophil to lymphocyte ratio in patients with ST-elevation myocardial infarction[J]. Medicine (Baltimore), 2018, 97(48): e13471.
MEEUWSEN J A L, WESSELING M, HOEFER I E, et al. Prognostic value of circulating inflammatory cells in patients with stable and acute coronary artery disease[J]. Front Cardiovasc Med, 2017, 4: 44.
CANDEMIR M, KIZILTUNÇ E, NURKOÇ S, et al. Relationship between systemic immune-inflammation index (SII) and the severity of stable coronary artery disease[J]. Angiology, 2021, 72(6): 575-581.
YANG Y L, WU C H, HSU P F, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease[J]. Eur J Clin Invest, 2020, 50(5): e13230.
LEE Y S G, BARADI A, PEVERELLE M, et al. Usefulness of platelet-to-lymphocyte ratio to predict long-term all-cause mortality in patients at high risk of coronary artery disease who underwent coronary angiography[J]. Am J Cardiol, 2018, 121(9): 1021-1026.
GAO J B, MA R C, LIU C R, et al. The value of systemic immune inflammation index in predicting in-hospital major adverse cardiovascular events after direct percutaneous coronary intervention in patients with acute myocardial infarction[J]. Journal of Clinical Emergency, 2022, 23(3):192-197.
Cardiovascular Disease Prevention and Rehabilitation Professional Committee of China Rehabilitation Medicine Association, China Committee of Cardio-Cerebral-Vascular Diseases of GSC, Psychosomatic Medicine Branch of the Chinese Medical Association. China expert consensus on psychological prescription for patients with cardiovascular disease (2020)[J]. Chinese Journal of Internal Medicine, 2020, 59(10): 764-771.
KERNAN W N, OVBIAGELE B, BLACK H R, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack[J]. Stroke, 2014, 45(7): 2160-2236.
HU D Y. Implementation of “double heart medicine” service model: attaching great importance to mental and psychological problems in doctor education and science communication[J]. Chinese General Practice, 2019, 22(18): 2150-2151.
WANG D X, LIU N, SHI Z Y, et al. Development status and nursing intervention of psycho-cardiology[J]. Chinese Journal of Geriatric Care, 2022, 20(3): 112-115.



{kind=link}
{kind=link}
{kind=link}
{kind=link}