Changes of serum high mobility group box 1 and soluble triggering receptor expressed on myeloid cells-1 in patients with multiple injuries and their prognostic significance
WANG Guijie,, DU Chuanchong, LU Ye, ZHAO Jian, SHEN Xie, JIN Donglin, GENG Jiacai,
Department of Emergency Medicine, Suzhou Ninth People′s Hospital, Jiangsu Province, Suzhou 215000, China
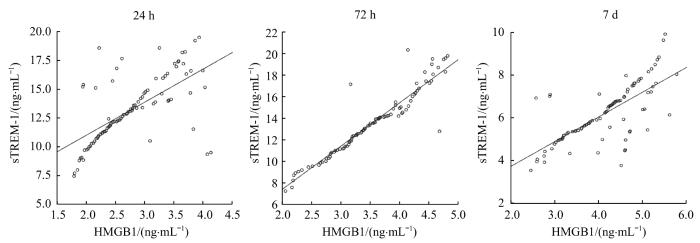
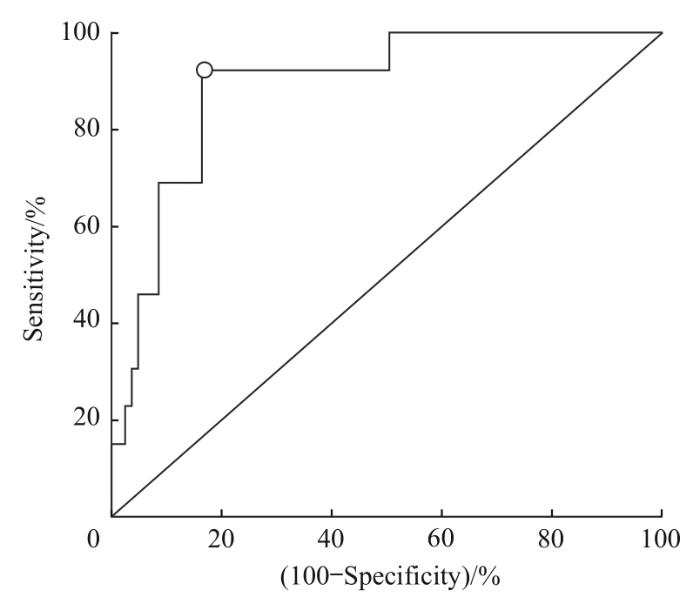
Objective ·To detect the serum levels of high mobility group box 1 (HMGB1) and soluble triggering receptor expressed on myeloid cells-1 (sTREM-1) in patients with multiple injuries at different time points, and to analyze their correlation with disease severity, complications and prognosis. Methods ·Ninety-two patients with multiple injuries admitted to the Department of Emergency Medicine of the Suzhou Ninth People′s Hospital from December 2020 to December 2022 were selected. According to the injury severity scores of the patients at admission, the patients were divided into light injury group (n=24), grave injury group (n=58) and severe injury group (n=10). According to whether there was multiple organ dysfunction syndrome (MODS) after admission, the patients were divided into MODS group (n=20) and non-MODS group (n=72). According to the outcome within 28 d after trauma, the patients were divided into death group (n=13) and survival group (n=79). Inflammatory factor indicators in venous blood of patients after admission were detected. Enzyme linked immunosorbent assay (ELISA) was used to detect the serum HMGB1 and sTREM-1 levels at 24 h, 72 h and 7 d after trauma, and the differences of serum HMGB1 and sTREM-1 levels among different groups were analyzed. Multiple Logistic regression was used to analyze the influencing factors of adverse outcomes in patients with multiple injuries. The receiver operating characteristic (ROC) curve was used to evaluate the predictive value of HMGB1 and sTREM-1 for adverse outcomes. Results ·The levels of HMGB1 and sTREM-1 in the grave injury and severe injury groups were significantly higher than those in the light injury group (P<0.05). The levels of HMGB1 at 72 h and 7 d, and sTREM-1 at 24 h and 72 h in the severe injury group were significantly higher than those in the grave injury group (P<0.05). There was a positive correlation between HMGB1 and sTREM-1 levels at various time points (r=0.645, r=0.942, r=0.722; all P<0.05). The levels of HMGB1 at 72 h and 7 d, and sTREM-1 at 24 h and 72 h in the MODS group were significantly higher than those in the non-MODS group (all P<0.05). The levels of HMGB1 at 72 h and 7 d, and sTREM-1 at 24 h and 72 h in the death group were significantly higher than those in the survival group (all P<0.05). Logistic regression analysis showed that HMGB1 at 7 d, admission time and hypersensitive C-reactive protein (hs-CRP) were independent factors of adverse outcomes in patients with multiple injuries (all P<0.05). The ROC curve showed that the area under the curve of HMGB1 for predicting poor prognosis at 7 days after trauma was 0.890, the sensitivity was 83.5%, and the specificity was 92.3%. Conclusion ·The levels of HMGB1 and sTREM-1 are correlated with MODS and survival outcomes in patients with multiple injuries at different time points after trauma, and HMGB1 at 7 d after trauma is an independent factor affecting adverse outcomes in patients with multiple injuries.
Keywords:multiple injury
;
high mobility group box 1 (HMGB1)
;
soluble triggering receptor expressed on myeloid cell-1 (sTREM-1)
;
prognosis
WANG Guijie, DU Chuanchong, LU Ye, ZHAO Jian, SHEN Xie, JIN Donglin, GENG Jiacai. Changes of serum high mobility group box 1 and soluble triggering receptor expressed on myeloid cells-1 in patients with multiple injuries and their prognostic significance. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(3): 350-357 doi:10.3969/j.issn.1674-8115.2024.03.007
多发伤指由1个致病因素导致2个及以上组织或器官的创伤,具有创伤程度重、病情变化快及易进展等特点,患者死亡风险较高[1-2]。准确评估病情的严重程度及预后,并进行合理临床决策,是降低并发症和死亡率、改善患者预后的关键。研究[3-4]证实,多发伤患者存在全身性的炎症水平升高,且与多发伤病情进展有关。高迁移率族蛋白B1(high mobility group box 1,HMGB1)是革兰阴性菌脂多糖、白介素和肿瘤坏死因子α(tumor necrosis factor α,TNF-α)等刺激巨噬细胞后产生的一种蛋白质,是重要的晚期炎症介质之一[5]。可溶性髓样细胞触发受体-1(soluble triggering receptor expressed on myeloid cell-1,sTREM-1)是近年来发现的炎症反应激发受体,也被证实在炎症触发和放大过程中具有重要意义[6]。目前有证据[7]显示,HMGB1与sTREM-1具有相关性。同时还有研究[8-9]发现,多发伤患者HMGB1及sTREM-1水平明显升高,且HMGB1及sTREM-1高水平患者预后较差。但关于多发伤患者创伤发生后不同时间点HMGB1和sTREM-1水平变化及其与病情严重程度、并发症及死亡的相关性研究尚不多见,相关结论也不够明确。因此,本研究通过检测多发伤患者创伤发生后24 h、72 h及7 d时的血清HMGB1及TREM-1水平,分析患者HMGB1及sTREM-1变化与病情严重程度、并发症及死亡的相关性,以期为患者病情判断、预后评估及干预措施的研究提供依据,从而辅助临床合理决策,改善患者预后。
患者入院后立即行ISS评分及格拉斯哥昏迷评分(Glasgow coma score,GCS)评估。ISS评分:将人体划分为头颈部、面部、胸部、腹部、四肢/骨盆、体表6个部分,每个部分得分按照简明损伤评分(abbrebiated injury scale,AIS)计算(1~5分);取评分最高的3个AIS值的平方和即为ISS分值,最高75分。GCS评分:依据睁眼反应、语言反应、运动反应的不同情况进行评分和分级,最高15分。
Tab 1 Comparison of HMGB1 and sTREM-1 levels in patients with multiple injuries of different severity
Variable
Light injury group
(n=24)
Grave injury group
(n=58)
Severe injury group
(n=10)
P value③
P value④
P value⑤
HMGB1/(ng·mL-1)①
24 h
2.47±0.61
2.86±0.65
2.99±0.52
0.013
0.030
0.531
72 h
3.12±0.73
3.57±0.66
4.22±0.31
0.006
0.000
0.005
7 d
3.63±0.83
4.19±0.77
4.96±0.35
0.003
0.000
0.004
sTREM-1/(ng·mL-1)②
24 h
11.71±3.00
13.43±2.65
15.38±1.95
0.010
0.000
0.037
72 h
12.77±3.47
14.46±2.74
16.51±1.99
0.017
0.001
0.041
7 d
5.52±1.24
6.47±1.25
6.72±1.20
0.006
0.015
0.463
Note:①Fgroup=9.579, Pgroup=0.000; Ftime=295.409, Ptime=0.000; Ftime×group=4.137, Ptime×group=0.002. ②Fgroup=7.262, Pgroup=0.001; Ftime=427.712, Ptime=0.000; Ftime×group=2.598, Ptime×group=0.038. ③P value of comparison between the light injury group and the grave injury group; ④P value of comparison between the light injury group and the severe injury group; ⑤P value of comparison between the grave injury group and the severe injury group.
The study was designed and conducted by WANG Guijie, DU Chuanchong, LU Ye and GENG Jiacai. The data were collected and analyzed by WANG Guijie, DU Chuanchong, LU Ye, ZHAO Jian, SHEN Xie and JIN Donglin. The manuscript was drafted and revised by WANG Guijie and GENG Jiacai. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
TACHINO J, KATAYAMA Y, KITAMURA T, et al. Assessment of the interaction effect between injury regions in multiple injuries: a nationwide cohort study in Japan[J]. J Trauma Acute Care Surg, 2021, 90(1): 185-190.
LINGITZ M T, WOLLNER G, BAUER J, et al. Elevation of neutrophil-derived factors in patients after multiple trauma[J]. J Cell Mol Med, 2023, 27(13): 1859-1866.
RELJA B, YANG B, BUNDKIRCHEN K, et al. Different experimental multiple trauma models induce comparable inflammation and organ injury[J]. Sci Rep, 2020, 10(1): 20185.
PATOULIAS D, KALOGIROU M S, PATOULIAS I. Triggering receptor expressed on myeloid cells-1 (TREM-1) and its soluble in the plasma form (sTREM-1) as a diagnostic biomarker in neonatal sepsis[J]. Folia Med Cracov, 2018, 58(2): 15-19.
PAKNEJAD M, SATTARI M, ROOZBAHANI Z, et al. Relationships between high-mobility group protein B1 and triggering receptor expressed on myeloid cells concentrations in gingival crevicular fluid and chronic periodontitis[J]. Iran J Allergy Asthma Immunol, 2016, 15(5): 381-385.
POLITO F, CICCIU′ M, AGUENNOUZ M, et al. Prognostic value of HMGB1 and oxidative stress markers in multiple trauma patients: a single-centre prospective study[J]. Int J Immunopathol Pharmacol, 2016, 29(3): 504-509.
ZHENG S Q, ZHANG W. Predictive values of sTREM-1, PCT and CRP for multiple trauma-induced acute respiratory distress syndrome complicated with pulmonary infection[J]. Clin Lab, 2022, 68(12). DOI: 10.7754/Clin.Lab.2022.211258.
Trauma Care and Multiple Injury Group of Traumatology Society of Chinese Medical Association. Consensus on medical documentation and diagnosis of multiple injury[J]. Journal of Traumatic Surgery, 2014, 16(2): 192.
LI Y, ZHANG L Y. Research progress and error analysis of abbreviated injury scale/injury severity score[J]. Chinese Journal of Trauma, 2021, 37(1): 11-14.
Trauma Infection Group, Trauma First Aid and Multiple Injury Group, Chinese Society of Trauma, Chinese Society of Trauma. Expert consensus on the definition and diagnosis of post-traumatic complications[J]. Chinese Journal of Trauma, 2013, 29(6): 481-484.
SHU X Y, FAN S H, XU Y, et al. Research progress on release mechanism of high mobility group protein B1 in acute respiratory distress syndrome[J]. Chinese Critical Care Medicine, 2021, 33(7): 889-893.
VIJAYAKUMAR E C, BHATT L K, PRABHAVALKAR K S. High mobility group box-1 (HMGB1): a potential target in therapeutics[J]. Curr Drug Targets, 2019, 20(14): 1474-1485.
OTTESTAD W, ROGNES I N, PISCHKE S E, et al. Biphasic release of the alarmin high mobility group box 1 protein early after trauma predicts poor clinical outcome[J]. Crit Care Med, 2019, 47(8): e614-e622.
WANG H, LI S G. Prognostic value of serum high mobility group protein B1 and procalcitonin in the patients with traumatic brain injury[J]. Chinese Journal of Critical Care Medicine, 2020, 40(5): 417-421.
YANG Z S, SIMOVIC M O, EDSALL P R, et al. HMGB1 inhibition to ameliorate organ failure and increase survival in trauma[J]. Biomolecules, 2022, 12(1): 101.
LIU F S, LI S, GUO L F, et al. The relationship between the levels of HMGB-1, cTnI and Ang2 and vascular endothelial injury and the risk of hospital death in patients with multiple injuries in the emergency department[J]. Journal of Molecular Diagnosis and Therapy, 2021, 13(8): 1349-1352.
SONG C, CAI H Z, ZHOU F, et al. Predictive value of serum HMGB-1,Mb,CK,IL-6 indicators in patients with acute abdominal multiple trauma on severity and prognosis[J]. Chinese Journal of Current Advances in General Surgery, 2020, 23(1): 27-30.
PIVA S, ALBANI F, FAGONI N, et al. High-mobility group box-1 protein as a novel biomarker to diagnose healthcare-associated ventriculitis and meningitis: a pilot study[J]. Minerva Anestesiol, 2021, 87(1): 43-51.
DU Q R, PAN S M, LI M, et al. The value of serum markers combined with acute physiology and chronic health evaluation score in the diagnosis and prognosis of multiple trauma with multiple organ dysfunction syndrome[J]. Chinese Journal for Clinicians, 2022, 50(2): 181-184.
FENG J Y, SU W J, PAN S W, et al. Role of TREM-1 in pulmonary tuberculosis patients: analysis of serum soluble TREM-1 levels[J]. Sci Rep, 2018, 8(1): 8223.
CHEN M K, ZHU Y. Utility of sTREM-1 and presepsin (sCD14-ST) as diagnostic and prognostic markers of sepsis[J]. Clin Lab, 2020, 66(4). DOI: 10.7754/Clin.Lab.2019.190508.
MAO Y S, LI Z X, LV T, et al. The significance of soluble triggering receptor expressed on myeloid cells-1 in the early diagnosis and prognosis of sepsis in patients with multiple trauma[J]. Chinese Journal of Trauma, 2015, 31(12): 1102-1105.
MA Y D, MENG F X, SONG Y. Relevance of the soluble triggering receptors expressed on myeloid cells-1 with multiple organ dysfunction syndrome after severe multiple trauma[J]. Shandong Medicine, 2013, 53(4): 11-13.



{kind=link}
{kind=link}
{kind=link}
{kind=link}