目的·系统评价体动记录仪对于抑郁症患者昼夜节律特征的评估效果。方法·检索PubMed、Embase、Web of Science、Cochrane Library、PsycINFO、中国知网(CNKI)、万方数据知识服务平台(WanFang)、中国生物医学文献数据库(Chinese biomedical literature database,CBM),检索文献发表时间为从各数据库建库开始至2023年05月05日,收集使用体动记录仪评估抑郁症患者的昼夜节律并与健康对照进行比较的横断面研究。由2名研究者根据纳入与排除标准独立筛选文献,并采用Newcastle-Ottawa Scale(NOS)文献质量评价量表对纳入的文献进行质量评价,最后使用RevMan5.4软件进行meta分析。结果·共纳入9篇文献,包括抑郁症患者390名,健康对照288名。Meta分析结果显示,抑郁症患者昼夜节律余弦函数的中值(midline statistic of rhythm,MESOR)(SMD=-0.29,95% CI -0.51~-0.07,P=0.009)小于健康对照;抑郁症患者的入睡时间(sleep onset)(MD=33.06,95% CI 14.90~51.23,P=0.000)和觉醒时间(sleep offset)(MD=53.80,95% CI 22.38~85.23,P=0.000)晚于健康对照;抑郁症患者和健康对照1 d中最活跃的10 h的活动量(activity during the 10 most active hours,M10)(SMD=-0.26,95% CI -0.52~0.01,P=0.060)间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势;抑郁症患者和健康对照昼夜节律余弦函数的峰值相位(acrophase)(MD=25.33,95% CI -12.41~63.06,P=0.190)间差异无统计学意义;抑郁症患者和健康对照昼夜节律余弦函数的振幅(amplitude)(SMD=-0.14,95% CI -0.42~0.14,P=0.340)以及1 d中最不活跃的5 h的活动量(activity during the 5 least active hours,L5)(SMD=0.31,95% CI -0.10~0.71,P=0.140)间差异的统计学意义并不明确。结论·体动记录仪能够在一定程度上反映抑郁症患者的昼夜节律紊乱,但因纳入研究数量有限,研究人群及方法不一致,对分析质量和结果产生了一定影响,需要更多高质量的临床试验提供证据。
关键词:抑郁症
;
体动记录仪
;
昼夜节律
;
meta分析
;
系统综述
Abstract
Objective ·To systematically review the effectiveness of actigraphy on the evaluation of circadian rhythm characteristics in patients with depression. Methods ·A systematic literature search was conducted in PubMed, Embase, Web of Science, Cochrane Library, PsycINFO, CNKI, WanFang Data, and Chinese biomedical literature database (CBM), from the inception of each database to May 5th, 2023. Case control studies that used actigraphy to evaluate circadian rhythms in patients with depression and compared them with healthy controls were collected. Literature was screened according to the inclusion and exclusion criteria, and the quality of the included literature was evaluated by using the Newcastle-Ottawa Scale. The meta-analysis was performed by using RevMan 5.4 software. Results ·A total of 9 articles were included, including 390 patients with depression and 288 healthy controls. The meta-analysis showed that the MESOR (midline statistic of rhythm) (SMD=-0.29, 95% CI -0.51 ‒ -0.07, P=0.009) of the circadian cosine function in patients with depression was lower than that in healthy controls; sleep onset (MD=33.06, 95% CI 14.90 ‒ 51.23, P=0.000) and sleep offset (MD=53.80, 95% CI 22.38 ‒ 85.23, P=0.000) were later in patients with depression than those in healthy controls; no statistical difference was found in the activity level of the most active 10 hours (SMD=-0.26, 95% CI -0.52 ‒ 0.01, P=0.060) between patients with depression and healthy controls, although there was a trend for lower activity in patients with depression; no statistical difference was found in the acrophase (MD=25.33, 95% CI -12.41 ‒ 63.06, P=0.190) of the circadian cosine function between patients with depression and healthy controls; no clear statistical significance of the difference was found in the amplitude (SMD=-0.14, 95% CI -0.42 ‒ 0.14, P=0.340) and the activity level of the least active 5 hours (SMD=0.31, 95% CI -0.10 ‒ 0.71, P=0.140) between patients with depression and healthy controls. Conclusion ·Actigraphy can reflect circadian rhythm disruption in patients with depression to some extent, but the limited number of included studies and inconsistencies in the study populations and methodologies have affected the quality and results of the analyses. More high-quality clinical trials are needed to provide evidence.
SUN Chenyin, WU Baichuan, ZHANG Huifeng, FANG Yiru, PENG Daihui. Evaluation of circadian rhythms in depression by using actigraphy: a systematic review and meta-analysis. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(5): 606-616 doi:10.3969/j.issn.1674-8115.2024.05.009
在昼夜节律的研究中,体动记录仪存储的信息可通过余弦函数进行分析:。其中,代表中值(midline statistic of rhythm,MESOR),反映昼夜活动量的平均水平;代表振幅(amplitude),反映1 d中活动量波动的幅度;代表峰值相位(acrophase),反映每个昼夜周期中活动量达到峰值的时间;代表一个昼夜周期的持续时间;代表误差项[14]。昼夜节律的非参数分析包括1 d中最活跃的10 h的活动量(activity during the 10 most active hours,M10)和最不活跃的5 h的活动量(activity during the 5 least active hours,L5)。入睡时间(sleep onset)和觉醒时间(sleep offset)则是由软件算法确定的。
系统检索PubMed、Embase、Web of Science、Cochrane Library、PsycINFO、中国知网(CNKI)、万方数据知识服务平台(WanFang)、中国生物医学文献数据库(Chinese Biomedical Literature Database,CBM)。通过组合抑郁症关键词和体动记录仪关键词以构建检索词。英文主题检索词包括“depressive disorder”“depressive disorder,major”“actigraphy”等,中文主题检索词包括“抑郁”“抑郁症”“体动描记术”等。检索文献发表时间为从各数据库建库开始至2023年05月05日。
1.2 文献纳入和排除标准
纳入标准:① 抑郁症患者和健康对照均使用体动记录仪评估昼夜节律的病例对照研究(case control study)。② 抑郁症患者需由专业精神科医师诊断,诊断标准基于DSM或ICD。③ 研究指标包括振幅、中值、峰值相位、M10、L5、入睡时间、觉醒时间。
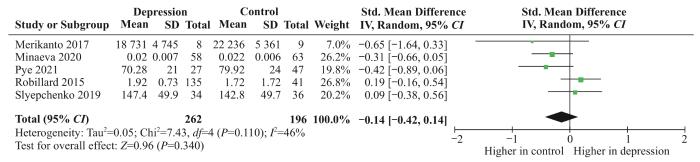
共有5项研究[17-21],包括262名抑郁症患者和196名健康对照,比较了2组的振幅。结果显示抑郁症患者和健康对照的振幅间差异无统计学意义(SMD=-0.14,95% CI -0.42~0.14,P=0.340),且可能存在中等程度的异质性(χ2=7.43,df=4,P=0.110,I2=46%),见图2。
共有5项研究[17,19-22],包括293名抑郁症患者和213名健康对照,比较了2组的峰值相位。其中3项研究[17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析。结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4。同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义。
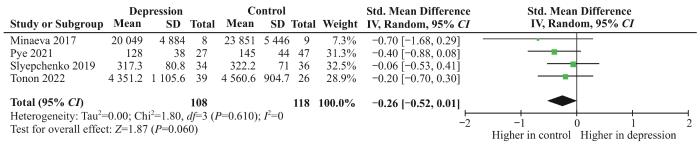
共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的M10。结果显示抑郁症患者和健康对照的M10间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势(SMD=-0.26,95% CI -0.52~0.01,P=0.060),且无明显异质性(χ2=1.80,df=3,P=0.610,I2=0),见图5。
Fig 5
Forest plot of activity during the 10 most active hours
2.4.5 L5
共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的L5。结果显示抑郁症患者和健康对照的L5间差异无统计学意义(SMD=0.31,95% CI -0.10~0.71,P=0.140),且可能存在中等程度或实质性的异质性(χ2=6.24,df=3,P=0.100,I2=52%),见图6。
Fig 6
Forest plot of activity during the 5 least active hours
2.4.6 入睡时间
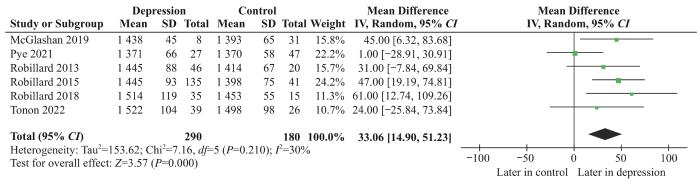
共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的入睡时间。结果显示抑郁症患者的入睡时间晚于健康对照(MD=33.06,95% CI 14.90~51.23,P=0.000),且可能无明显异质性或存在中等程度的异质性(χ2=7.16,df=5,P=0.210,I2=30%),见图7。
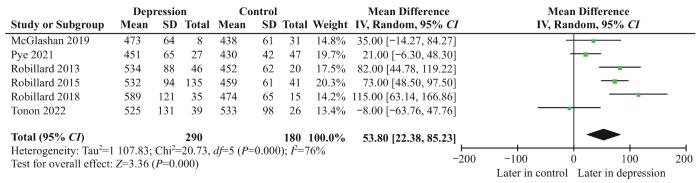
共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的觉醒时间。结果显示抑郁症患者的觉醒时间晚于健康对照(MD=53.80,95% CI 22.38~85.23,P=0.000),且存在较大的异质性(χ2=20.73,df=5,P=0.000,I2=76%),见图8。
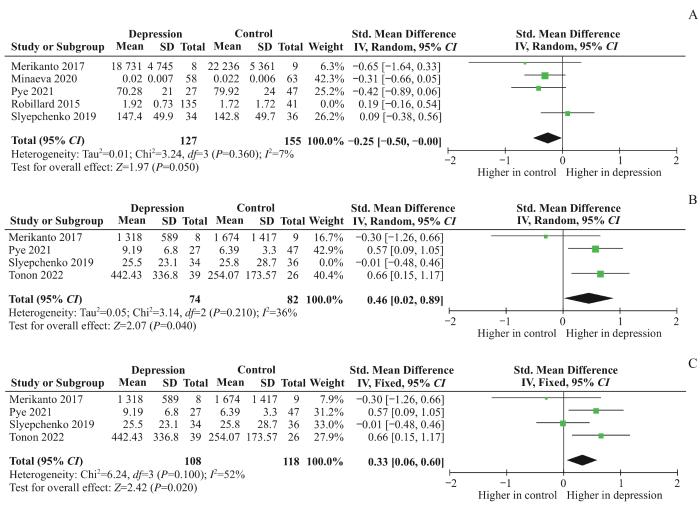
然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度。
Note: A. Forest plot for sensitivity analysis of amplitude. B. Forest plot for sensitivity analysis of L5 (excluding studies). C. Forest plot for sensitivity analysis of L5 (changing statistical models).
SUN Chenyin and WU Baichuan were responsible for determining the meta-analysis topic, developing the literature search strategy and the inclusion criteria, literature screening, data extraction, quality evaluation and writing the article. ZHANG Huifeng was responsible for determining the meta-analysis topic and providing decision-making in the event of disagreement in literature screening, data extraction and quality evaluation. FANG Yiru and PENG Daihui were responsible for revising and reviewing the article. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
DUARTE FARIA A, CARDOSO T D, CAMPOS MONDIN T, et al. Biological rhythms in bipolar and depressive disorders: a community study with drug-naïve young adults[J]. J Affect Disord, 2015, 186: 145-148.
MONDIN T C, CARDOSO T A, SOUZA L D M, et al. Mood disorders and biological rhythms in young adults: a large population-based study[J]. J Psychiatr Res, 2017, 84: 98-104.
OZCELIK M, SAHBAZ C. Clinical evaluation of biological rhythm domains in patients with major depression[J]. Braz J Psychiatry, 2020, 42(3): 258-263.
TAZAWA Y, WADA M, MITSUKURA Y, et al. Actigraphy for evaluation of mood disorders: a systematic review and meta-analysis[J]. J Affect Disord, 2019, 253: 257-269.
BURTON C, MCKINSTRY B, SZENTAGOTAI TĂTAR A, et al. Activity monitoring in patients with depression: a systematic review[J]. J Affect Disord, 2013, 145(1): 21-28.
WÜTHRICH F, NABB C B, MITTAL V A, et al. Actigraphically measured psychomotor slowing in depression: systematic review and meta-analysis[J]. Psychol Med, 2022, 52(7): 1208-1221.
WAN X, WANG W Q, LIU J M, et al. Estimating the sample mean and standard deviation from the sample size, Median, range and/or interquartile range[J]. BMC Med Res Methodol, 2014, 14: 135.
ROBILLARD R, HERMENS D F, NAISMITH S L, et al. Ambulatory sleep-wake patterns and variability in young people with emerging mental disorders[J]. J Psychiatry Neurosci, 2015, 40(1): 28-37.
MERIKANTO I, PARTONEN T, PAUNIO T, et al. Advanced phases and reduced amplitudes are suggested to characterize the daily rest-activity cycles in depressed adolescent boys[J]. Chronobiol Int, 2017, 34(7): 967-976.
SLYEPCHENKO A, ALLEGA O R, LENG X M, et al. Association of functioning and quality of life with objective and subjective measures of sleep and biological rhythms in major depressive and bipolar disorder[J]. Aust N Z J Psychiatry, 2019, 53(7): 683-696.
MINAEVA O, BOOIJ S H, LAMERS F, et al. Level and timing of physical activity during normal daily life in depressed and non-depressed individuals[J]. Transl Psychiatry, 2020, 10(1): 259.
PYE J, PHILLIPS A J, CAIN S W, et al. Irregular sleep-wake patterns in older adults with current or remitted depression[J]. J Affect Disord, 2021, 281: 431-437.
TONON A C, CONSTANTINO D B, AMANDO G R, et al. Sleep disturbances, circadian activity, and nocturnal light exposure characterize high risk for and current depression in adolescence[J]. Sleep, 2022, 45(7): zsac104.
ROBILLARD R, NAISMITH S L, ROGERS N L, et al. Delayed sleep phase in young people with unipolar or bipolar affective disorders[J]. J Affect Disord, 2013, 145(2): 260-263.
ROBILLARD R, CARPENTER J S, ROGERS N L, et al. Circadian rhythms and psychiatric profiles in young adults with unipolar depressive disorders[J]. Transl Psychiatry, 2018, 8(1): 213.
MCGLASHAN E M, COLEMAN M Y, VIDAFAR P, et al. Decreased sensitivity of the circadian system to light in current, but not remitted depression[J]. J Affect Disord, 2019, 256: 386-392.
ZHANG T S. The selection of appropriate statistical models for traditional meta-analysis[J]. Chinese Journal of Evidence-Based Medicine, 2020, 20(12): 1477-1481.
CARPENTER J S, CROUSE J J, SCOTT E M, et al. Circadian depression: a mood disorder phenotype[J]. Neurosci Biobehav Rev, 2021, 126: 79-101.
CROUSE J J, CARPENTER J S, SONG Y J C, et al. Circadian rhythm sleep-wake disturbances and depression in young people: implications for prevention and early intervention[J]. Lancet Psychiatry, 2021, 8(9): 813-823.
TONON A C, PILZ L K, MARKUS R P, et al. Melatonin and depression: a translational perspective from animal models to clinical studies[J]. Front Psychiatry, 2021, 12: 638981.
SCHUCH F, VANCAMPFORT D, FIRTH J, et al. Physical activity and sedentary behavior in people with major depressive disorder: a systematic review and meta-analysis[J]. J Affect Disord, 2017, 210: 139-150.
HASLER B P, BUYSSE D J, KUPFER D J, et al. Phase relationships between core body temperature, melatonin, and sleep are associated with depression severity: further evidence for circadian misalignment in non-seasonal depression[J]. Psychiatry Res, 2010, 178(1): 205-207.
GHANEAN H, CENITI A K, KENNEDY S H. Fatigue in patients with major depressive disorder: prevalence, burden and pharmacological approaches to management[J]. CNS Drugs, 2018, 32(1): 65-74.
GIANFREDI V, FERRARA P, PENNISI F, et al. Association between daily pattern of physical activity and depression: a systematic review[J]. Int J Environ Res Public Health, 2022, 19(11): 6505.
HAGENAUER M H, PERRYMAN J I, LEE T M, et al. Adolescent changes in the homeostatic and circadian regulation of sleep[J]. Dev Neurosci, 2009, 31(4): 276-284.
HICKIE I, CARPENTER J, ROBILLARD R. Variations in the sleep-wake cycle from childhood to adulthood: chronobiological perspectives[J]. ChronoPhysiology Ther, 2015: 37.
TAKAESU Y, KANDA, NAGAHAMA Y, et al. Delayed sleep-wake rhythm is associated with cognitive dysfunction, social dysfunction, and deteriorated quality of life in patients with major depressive disorder[J]. Front Psychiatry, 2022, 13: 1022144.
CHAN J W, LAM S P, LI S X, et al. Eveningness and insomnia: independent risk factors of nonremission in major depressive disorder[J]. Sleep, 2014, 37(5): 911-917.
ANGEL V D, LEWIS S, WHITE K, et al. Digital health tools for the passive monitoring of depression: a systematic review of methods[J]. NPJ Digit Med, 2022, 5(1): 3.
ALI F Z, PARSEY R V, LIN S, et al. Circadian rhythm biomarker from wearable device data is related to concurrent antidepressant treatment response[J]. NPJ Digit Med, 2023, 6(1): 81.
XAVIER N B, ABREU A C V O, AMANDO G R, et al. Chronobiological parameters as predictors of early treatment response in major depression[J]. J Affect Disord, 2023, 323: 679-688.
DUNCAN W C Jr, SLONENA E, HEJAZI N S, et al. Motor-activity markers of circadian timekeeping are related to ketamine′s rapid antidepressant properties[J]. Biol Psychiatry, 2017, 82(5): 361-369.
... 在昼夜节律的研究中,体动记录仪存储的信息可通过余弦函数进行分析:.其中,代表中值(midline statistic of rhythm,MESOR),反映昼夜活动量的平均水平;代表振幅(amplitude),反映1 d中活动量波动的幅度;代表峰值相位(acrophase),反映每个昼夜周期中活动量达到峰值的时间;代表一个昼夜周期的持续时间;代表误差项[14].昼夜节律的非参数分析包括1 d中最活跃的10 h的活动量(activity during the 10 most active hours,M10)和最不活跃的5 h的活动量(activity during the 5 least active hours,L5).入睡时间(sleep onset)和觉醒时间(sleep offset)则是由软件算法确定的. ...
5
... 使用Review Manager(RevMan)5.4进行数据分析.由于各研究间使用的计算方法不同导致振幅、中值、M10、L5的均数相差较大,故采用标准化均数差值(standardized mean difference,SMD)和95%置信区间(confidence interval,CI)合并效应量.峰值相位、入睡时间、觉醒时间均由“HH:MM”格式转换为分钟数,例如14∶30记录为(14×60)+30=870 min.上述3个指标均采用均数差值(mean difference,MD)和95%CI合并效应量.通过Q检验和I2值分析研究之间的异质性.Cochrane手册[15]推荐Q检验的P<0.10表明存在显著的异质性,I2值为0~40%代表异质性可能并不重要,I2值为30%~60%代表可能存在中等程度的异质性,I2值为50%~90%代表可能存在实质性的异质性,I2值为70%~100%代表存在较大的异质性.由于Cochrane Handbook[15]认为不应基于异质性的统计检验来选择固定效应模型或随机效应模型,且各研究间的参与者、体动记录仪信息存在客观差异,因此上述指标均采用随机效应模型进行分析.对于以M(IQR)表示数据的研究,根据WAN等[16]的方法将数据转换为.但是,当研究以M(IQR)而非表示数据时,通常代表数据呈偏态分布[15].因此,尽管WAN等[16]的方法适用于偏态数据,但为了观察数据转换对于结果的影响和检验meta分析结果的稳定性,对所有指标均进行了敏感度分析.如纳入本次meta分析的文献数量大于10篇,则绘制漏斗图并对漏斗图的不对称性进行检验,以观察是否存在发表偏倚[15]. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有5项研究[17-21],包括262名抑郁症患者和196名健康对照,比较了2组的振幅.结果显示抑郁症患者和健康对照的振幅间差异无统计学意义(SMD=-0.14,95% CI -0.42~0.14,P=0.340),且可能存在中等程度的异质性(χ2=7.43,df=4,P=0.110,I2=46%),见图2. ...
... 共有5项研究[17,19-22],包括293名抑郁症患者和213名健康对照,比较了2组的峰值相位.其中3项研究[17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... [17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的入睡时间.结果显示抑郁症患者的入睡时间晚于健康对照(MD=33.06,95% CI 14.90~51.23,P=0.000),且可能无明显异质性或存在中等程度的异质性(χ2=7.16,df=5,P=0.210,I2=30%),见图7. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的觉醒时间.结果显示抑郁症患者的觉醒时间晚于健康对照(MD=53.80,95% CI 22.38~85.23,P=0.000),且存在较大的异质性(χ2=20.73,df=5,P=0.000,I2=76%),见图8. ...
... 然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的M10.结果显示抑郁症患者和健康对照的M10间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势(SMD=-0.26,95% CI -0.52~0.01,P=0.060),且无明显异质性(χ2=1.80,df=3,P=0.610,I2=0),见图5. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的L5.结果显示抑郁症患者和健康对照的L5间差异无统计学意义(SMD=0.31,95% CI -0.10~0.71,P=0.140),且可能存在中等程度或实质性的异质性(χ2=6.24,df=3,P=0.100,I2=52%),见图6. ...
... 然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... [18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
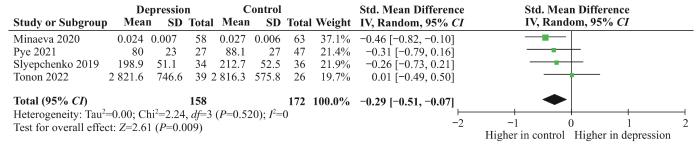
... 共有4项研究[19-22],包括158名抑郁症患者和172名健康对照,比较了2组的中值.结果显示抑郁症患者的中值小于健康对照(SMD=-0.29,95% CI -0.51~-0.07,P=0.009),且无明显异质性(χ2=2.24,df=3,P=0.520,I2=0),见图3. ...
... 共有5项研究[17,19-22],包括293名抑郁症患者和213名健康对照,比较了2组的峰值相位.其中3项研究[17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... [19]均报告2组的峰值相位间差异无统计学意义. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的M10.结果显示抑郁症患者和健康对照的M10间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势(SMD=-0.26,95% CI -0.52~0.01,P=0.060),且无明显异质性(χ2=1.80,df=3,P=0.610,I2=0),见图5. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的L5.结果显示抑郁症患者和健康对照的L5间差异无统计学意义(SMD=0.31,95% CI -0.10~0.71,P=0.140),且可能存在中等程度或实质性的异质性(χ2=6.24,df=3,P=0.100,I2=52%),见图6. ...
... 然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有5项研究[17,19-22],包括293名抑郁症患者和213名健康对照,比较了2组的峰值相位.其中3项研究[17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有5项研究[17-21],包括262名抑郁症患者和196名健康对照,比较了2组的振幅.结果显示抑郁症患者和健康对照的振幅间差异无统计学意义(SMD=-0.14,95% CI -0.42~0.14,P=0.340),且可能存在中等程度的异质性(χ2=7.43,df=4,P=0.110,I2=46%),见图2. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的M10.结果显示抑郁症患者和健康对照的M10间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势(SMD=-0.26,95% CI -0.52~0.01,P=0.060),且无明显异质性(χ2=1.80,df=3,P=0.610,I2=0),见图5. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的L5.结果显示抑郁症患者和健康对照的L5间差异无统计学意义(SMD=0.31,95% CI -0.10~0.71,P=0.140),且可能存在中等程度或实质性的异质性(χ2=6.24,df=3,P=0.100,I2=52%),见图6. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的入睡时间.结果显示抑郁症患者的入睡时间晚于健康对照(MD=33.06,95% CI 14.90~51.23,P=0.000),且可能无明显异质性或存在中等程度的异质性(χ2=7.16,df=5,P=0.210,I2=30%),见图7. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的觉醒时间.结果显示抑郁症患者的觉醒时间晚于健康对照(MD=53.80,95% CI 22.38~85.23,P=0.000),且存在较大的异质性(χ2=20.73,df=5,P=0.000,I2=76%),见图8. ...
... 然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... ,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有4项研究[19-22],包括158名抑郁症患者和172名健康对照,比较了2组的中值.结果显示抑郁症患者的中值小于健康对照(SMD=-0.29,95% CI -0.51~-0.07,P=0.009),且无明显异质性(χ2=2.24,df=3,P=0.520,I2=0),见图3. ...
... 共有5项研究[17,19-22],包括293名抑郁症患者和213名健康对照,比较了2组的峰值相位.其中3项研究[17,20,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... ,22](包括232名抑郁症患者和130名健康对照)被纳入meta分析.结果显示抑郁症患者和健康对照的峰值相位间差异无统计学意义(MD=25.33,95% CI -12.41~63.06,P=0.190),且可能存在中等程度的异质性(χ2=3.62,df=2,P=0.160,I2=45%),见图4.同样,另2项研究[19]均报告2组的峰值相位间差异无统计学意义. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的M10.结果显示抑郁症患者和健康对照的M10间差异无统计学意义,但抑郁症患者的活动量有小于健康对照的趋势(SMD=-0.26,95% CI -0.52~0.01,P=0.060),且无明显异质性(χ2=1.80,df=3,P=0.610,I2=0),见图5. ...
... 共有4项研究[18-19,21-22],包括108名抑郁症患者和118名健康对照,比较了2组的L5.结果显示抑郁症患者和健康对照的L5间差异无统计学意义(SMD=0.31,95% CI -0.10~0.71,P=0.140),且可能存在中等程度或实质性的异质性(χ2=6.24,df=3,P=0.100,I2=52%),见图6. ...
... 然而对于振幅,在剔除ROBILLARD等[17]的研究后,剩余4项研究[18-21](包括127名抑郁症患者和155名健康对照)的meta分析结果变为抑郁症患者的振幅小于健康对照(SMD=-0.25,95% CI -0.50~-0.00,P=0.050),且无明显异质性(χ2=3.24,df=3,P=0.360,I2=7%,图9A);对于L5,在剔除SLYEPCHENKO等[19]的研究后,剩余3项研究[18,21,22](包括74名抑郁症患者和82名健康对照)的meta分析结果变为抑郁症患者的L5大于健康对照(SMD=0.46,95% CI 0.02~0.89,P=0.040),且可能无明显异质性或存在中等程度的异质性(χ2=3.14,df=2,P=0.210,I2=36%,图9B);此外,固定效应模型的合并结果同样表明抑郁症患者和健康对照的差异有统计学意义(SMD=0.33,95% CI 0.06~0.60,P=0.020,图9C);说明上述2个指标meta分析的结果不稳定,在解释时需要持谨慎态度. ...
... Quality assessment of the included studiesTab 2
Study
Selection
Comparability
Outcome
Quality score
①
②
③
④
①
②
①
②
③
ROBILLARD, 2015[17]
1
1
1
1
1
1
1
1
1
9
MERIKANTO, 2017[18]
1
1
1
1
1
1
1
1
0
8
SLYEPCHENKO, 2019[19]
0
1
1
1
1
1
1
1
0
7
MINAEVA, 2020[20]
0
1
1
1
1
1
1
1
1
8
PYE, 2021[21]
0
1
0
1
1
0
1
1
1
6
TONON, 2022[22]
0
1
1
1
0
1
1
1
0
6
ROBILLARD, 2013[23]
1
1
0
0
0
1
1
1
1
6
ROBILLARD, 2018[24]
0
1
1
1
0
1
1
1
1
7
MCGLASHAN, 2019[25]
0
0
1
1
0
1
1
1
1
6
Note: The quality assessment was conducted by using NOS. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的入睡时间.结果显示抑郁症患者的入睡时间晚于健康对照(MD=33.06,95% CI 14.90~51.23,P=0.000),且可能无明显异质性或存在中等程度的异质性(χ2=7.16,df=5,P=0.210,I2=30%),见图7. ...
... 共有6项研究[17,21-25],包括290名抑郁症患者和180名健康对照,比较了2组的觉醒时间.结果显示抑郁症患者的觉醒时间晚于健康对照(MD=53.80,95% CI 22.38~85.23,P=0.000),且存在较大的异质性(χ2=20.73,df=5,P=0.000,I2=76%),见图8. ...






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}