

终末期肾病(end-stage renal disease,ESRD)的发病率及死亡率在世界范围内逐年升高[1]。JHA等[2]研究显示,40%~70%的ESRD患者存在不同程度的认知功能障碍,ESRD可能是导致患者临床痴呆的独立危险因素,而这种认知功能水平下降是肾病脑损伤的结果。认知功能障碍常导致患者执行功能、记忆功能、逻辑思维及判断能力的下降,干扰患者对慢性肾病治疗的依从性和药物使用的准确性,进一步影响疾病总体进程及患者预后。因此,早期筛查合并认知障碍的ESRD患者,延缓此类患者的认知功能损伤至关重要。目前,临床普遍认为ESRD患者认知功能损伤可能与较高的颅内小血管病(cerebral small vessel disease,CSVD)发病率有关,且CSVD是血管性认知障碍的首因[3]。因此,伴有认知障碍的肾病患者颅内有更高概率出现慢性微出血灶及急性腔隙性梗塞灶等微小血管病变。磁敏感加权成像(susceptibility-weighted imaging,SWI)是一种高灵敏度的功能磁共振成像技术,可精准显示颅内出血产物沉积和顺磁性物质出现,并可进行定量分析,呈现大脑微出血灶情况,进而反映患者颅内微小血管病变的严重程度。通过SWI呈现的大脑微出血灶的形成及分布探究认知损伤的发展变化过程,可为肾病脑损伤的研究提供新思路。本研究拟通过SWI技术探究ESRD患者大脑微出血灶的形成和分布特征,分析其与认知功能障碍的相关性,为临床早期识别ESRD患者认知功能障碍和合理有效干预提供影像学依据,从而促进ESRD脑损伤的早期筛查和治疗。
1 对象与方法
1.1 研究对象及样本量估计
前瞻性纳入2023年1月—2024年3月在上海交通大学医学院附属第六人民医院住院的ESRD患者,并收集其临床资料。纳入标准:①规律行维持性血液透析且透析时间>1年。ESRD诊断标准参照2013年改善全球肾脏病预后组织(Kidney Disease:Improving Global Outcomes,KDIGO)制定的慢性肾脏病诊断和分期标准[4]。②年龄18~55岁,右利手。③无明显中枢神经系统疾病史(包括脑卒中、脑肿瘤、脑炎及明显脱髓鞘病变等)。④无重大精神心理创伤史。⑤无MRI检查禁忌证。⑥无恶性肿瘤病史。排除标准:①无法配合MRI检查或认知量表测试。②合并严重心肝功能不全。
本研究采用横断面调查的样本量估算公式计算样本量:n=Z2×p×(1-p)÷E2。其中95%置信水平对应的Z值为1.96,选择合理的发生概率p=0.20及允许的误差E=0.13,计算得出n为36。
1.2 MRI数据采集与处理
所有患者在入组后即分别行常规MRI序列扫描[T1加权成像(T1-weighted imaging,T1WI)、液体衰减反转恢复T2加权成像(T2 fluid attenuated inversion recovery,T2-FLAIR)]及SWI扫描,常规序列筛查临床上的静息病灶,SWI技术直接生成全脑相位图及幅值图。使用美国GE公司Discovery MR750 3.0T高场磁共振成像仪进行扫描,采用配套的8通道相控阵头部线圈。检查时要求患者放松、闭眼并保持清醒。患者头部用软垫加以固定,并用软耳塞塞住外耳道以减少噪音干扰。
扫描主要参数如下。T1WI序列:重复时间(repetition time,TR)/回波时间(echo time,TE)为500 ms/14 ms,层厚为4 mm,层距为1 mm,激励次数为1,视野(field of view,FOV)为240 mm×240 mm,矩阵为256×160。T2-FLAIR序列:TR/TE为3 000 ms/40 ms,层厚为4 mm,间距为1 mm,激励次数为1,FOV为240 mm×240 mm。SWI序列:TR/TE为1 350 ms/5 ms,翻转角为155°,层厚为4 mm,层距为0 mm,矩阵为128×128,扫描覆盖范围与T1WI及T2-FLAIR相一致。采用GE公司AW4.4工作站中的Functool软件对SWI图像进行后处理。后处理方法:在工作站中选择SWI图像并启动Functool,Cursor设为1×1,不进行平滑处理,阈值设置中使得绿色斜线区域覆盖整个脑部,选择相位滤波器的大小,用以过滤背景引起的相位变化,选择默认32×32,不加入计算的回波图像。选择所获得的相位图及幅值图,将用于显示脑实质静脉结构像的最小密度投影(minimum intensity projection,MIP)图叠加到相位图上,以寻找评估大脑微出血灶。
1.3 患者分组
患者入组后,即采用蒙特利尔认知评估量表(Montreal Cognitive Assessment,MoCA)进行认知功能评估。MoCA是国际上对认知功能进行快速筛查的评定工具,敏感性高,测试时间短,适合临床运用。MoCA包括注意与集中、执行功能、记忆、语言、视结构技能、抽象思维、计算和定向力等8个认知领域的11个检查项目。总分为30分,通用标准以26分为界,≥26分视为认知功能正常,<26分则被认为存在一种或多种的认知障碍[5]。本研究中将得分≥26分者归为ESRD无认知障碍组,<26分者为ESRD合并认知障碍组。
1.4 统计学方法
采用SPSS 25.0软件进行数据分析。符合正态分布的定量资料用x±s表示,组间比较采用独立样本t检验或fisher精确检验。定性资料采用例数(百分率)表示,组间比较采用χ2检验。定量资料的相关性检验采用皮尔森相关分析。P<0.05表示差异具有统计学意义。
2 结果
2.1 患者一般临床资料
将107例接受治疗的ESRD患者依照纳入及排除标准,最终入组38例患者,其中男性23例,女性15例,平均年龄分别为(37.9±8.1)岁、(40.2±6.5)岁。依照MoCA得分结果,将患者分为ESRD合并认知障碍组16例、无认知障碍组22例。2组患者在年龄、受教育时间、性别、入组时血压水平以及距离上次透析时长上差异均无统计学意义(表1)。
表1 2组患者一般资料比较
Tab 1
| Characteristic | ESRD with cognitive impairment (n=16) | ESRD without cognitive impairment (n=22) | t/χ2 value | P value |
|---|---|---|---|---|
| Age/year | 37.2±7.3 | 38.8±7.5 | 1.313 | 0.242 |
| Gender/n | 0.210 | 0.743 | ||
| Male | 9 | 14 | ||
| Female | 7 | 8 | ||
| Duration of education/year | 11.32±2.61 | 11.88±2.25 | -0.219 | 0.844 |
| Systolic pressure①/mmHg | 152.40±19.61 | 147.58±13.22 | 1.840 | 0.069 |
| Duration of recent dialysis/d | 2.6±0.9 | 2.1±1.3 | 0.359 | 0.731 |
2.2 大脑微出血灶与认知障碍的关系
经SWI检测,ESRD合并认知障碍组16例患者中有大脑微出血灶者14例(87.50%),无大脑微出血灶者2例(12.50%);无认知障碍组22例患者中有大脑微出血灶者12例(54.55%),无大脑微出血灶者10例(45.45%)。2组大脑微出血灶发生人数差异有统计学意义(χ2=4.66,P=0.033)。
表2 患者不同脑区微出血灶数目比较
Tab 2
| Brain region | CMB in ESRD group with cognitive impairment (n=106) | CMB in ESRD group without cognitive impairment (n=47) | χ2 | P value |
|---|---|---|---|---|
| Cortex and subcortical area/n(%) | 63 (59.43) | 19 (40.43) | 4.74 | 0.029 |
| Basal ganglion/n(%) | 21 (19.81) | 22 (46.80) | 11.25 | 0.001 |
| Brainstem/n(%) | 7 (6.60) | 2 (4.26) | ‒ | 0.440 |
| Cerebellum/n(%) | 15 (14.15) | 4 (8.51) | ‒ | 0.244 |
图1
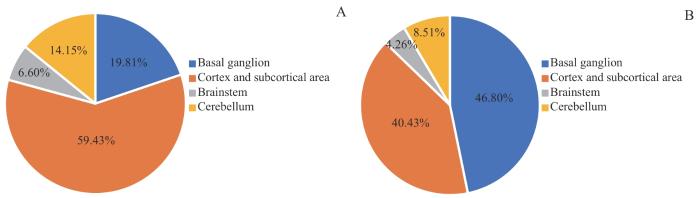
图1
患者不同脑区微出血灶分布的比例
Note:A. ESRD with cognitive impairment. B. ESRD without cognitive impairment.
Fig 1
Proportion of CMB distribution in different brain regions of patients
图2
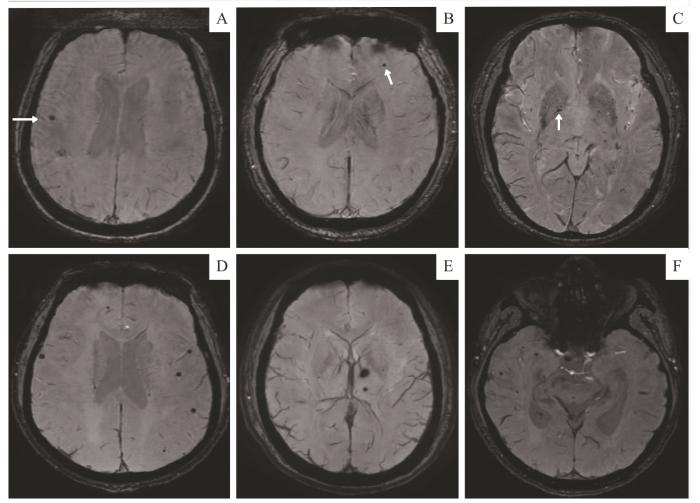
图2
2例患者不同脑区微出血灶的SWI图像
Note: A‒C. A 36-year-old female with ESRD who had undergone hemodialysis for 3 years had a few lesions in the right frontal lobe proximal cortex (A), the left frontal subcortex (B) and the right globus pallidus (C). The white arrows show the lesions in each brain region. This patient had no cognitive impairment, with a MoCA score of 28. D‒F. A 41-year-old male with ESRD who had undergone hemodialysis for 1.5 years showed multiple scattered CMBs in the frontal, temporal and occipital lobe (D and F), as well as in the left basal ganglia (E). This patient had cognitive impairment, with a MoCA score of 17.
Fig 2
SWI images of CMBs in different brain regions in two patients
进一步分析皮层及皮层下、基底节区大脑微出血灶数量与MoCA总分的关系,合并认知障碍患者双侧基底节微出血灶数量与MoCA总分无相关性(r=-0.11,P=0.291),而皮层及皮层下脑组织微出血灶数量与MoCA总分存在显著负相关(r=-0.718,P=0.030)。
3 讨论
本研究发现,ESRD患者合并认知功能下降是普遍存在的,相较于认知功能正常的ESRD患者,这类患者通常大脑微出血灶数量更多,且呈多个脑区散在分布。对于慢性肾病患者而言,肾脏功能损害以及长期血液透析引起的体内毒素淤积、电解质代谢紊乱、贫血状态和氧化应激反应均可能导致患者脑部血管内皮功能障碍或内皮细胞损伤,进而发生脑缺血、脑白质病变以及脑微出血等各种小血管病变[6]。因此,血管性认知障碍可能是ESRD患者认知障碍的重要因素。大脑微出血灶作为一种典型的由多种致病因素导致的脑实质微小血管损伤后改变,是ESRD患者重要的亚临床损害之一[7-8]。ESRD的多种病理改变长期累及微小血管,使血管壁通透性增加,管壁弹性降低,最终导致血管渗血甚至破裂出血[9]。而大脑微出血灶的出现,又会破坏脑白质结构的完整性,进一步影响着大脑神经功能的连接[10],恶性循环使得患者认知障碍加剧。
本研究还表明,ESRD合并认知障碍患者的大脑微出血灶分布具有一定特点,以双侧皮层及皮层下最为多见。皮层及皮层下多个区域是人体执行能力、注意力、语言及视觉空间能力等多种认知功能的核心区域,此区域微出血灶形成则意味着相应的认知水平下降[11-13]。这类患者执行功能受损是最为普遍的,因为大脑微出血灶影响到额顶叶皮层及皮层下区域的神经网络连接。本研究结果也说明皮层及皮层下微出血灶的存在是影响认知水平的重要因素。此外,本研究还发现分布于皮层及皮层下的微出血灶的数量与患者认知水平呈显著负相关。WERRING等[14]的研究也表明,双侧额叶皮层微出血灶较多者,执行能力存在明显障碍。JANSEN等[15]采用客观的认知评估量表及主观随访评估有小血管病变而无明显痴呆的老年人群的认知能力,发现大脑微出血灶的出现,尤其是集中分布于双侧额、颞叶及基底节区等深部结构的微出血灶,对患者的反应能力和注意力影响尤为重大。因此本研究结果与既往研究相仿,同样证实了特定脑部区域微出血灶数量与认知受损程度的密切关系。
此外,既往也有采用其他影像学技术并通过定量分析脑组织信号异常程度来辨别患者是否存在认知障碍的研究。基于动脉自旋标记法(arterial spin labeling,ASL)的研究[18]发现,慢性肾病认知功能损伤者,其大脑内侧前额叶和颞中回皮层结构的局部脑血流量(cerebral blood flow,CBF)明显减少。采用静息态功能磁共振成像(resting-state functional magnetic resonance imaging,rs-fMRI)的脑功能连接分析发现,ESRD合并认知障碍者的默认模式网络中多个脑区连通活动普遍减少[19]。这类研究均表明,ESRD患者是否合并认知障碍以及认知障碍的程度是可以侧面通过中枢神经系统的影像学特征反映出来的。本研究与上述功能成像技术研究的结果大致相符。然而,ESRD患者的认知功能损伤并非无法治愈,通过透析过滤患者体内过多的尿毒症相关毒素,以及纠正贫血状态后,患者认知水平下降的状态可以暂时性得到缓解;然而随着病情进展,颅内微血管病变逐渐加剧,患者的认知障碍状态将会愈发加剧、持续时间延长,且难以转复[20]。因此,ESRD患者大脑微出血灶的形成及数量是微血管病变所致的肾病脑损伤的重要预测因子。
SWI作为一种无创快速的磁共振成像技术,是发现ESRD患者颅内微血管病变的最佳影像学手段。本研究认为,ESRD患者在长期透析治疗过程中有必要定期行SWI检查,以便纵向评估患者中枢神经系统病变状态及认知水平。基于SWI检测大脑微出血灶的形成与分布区域,可以为临床早期干预患者认知水平下降提供重要的影像学依据,以满足临床早期预防筛查的需求。
伦理批准和知情同意
本研究通过上海交通大学医学院附属第六人民医院伦理委员会审批(编号:2021-KY-125)。经批准本研究已豁免书面知情同意,研究开始前,已告知患者研究目的。
Ethics Approval and Patient Consent
This study has been approved by the Ethics Committee of Shanghai Sixth People's Hospital, Shanghai Jiao Tong University School of Medicine (Approval letter No. 2021-KY-125). After being approved, this study has been exempted from written informed consent, and the purpose of the study was explained to the patients prior to its initiation.
作者贡献声明
顾梁瑞负责资料收集、数据分析、论文撰写,方统磊及颜碧从负责统计学数据核验、影像图像选择,吴金亮参与研究设计、监督,以及论文指导。所有作者均阅读并同意了最终稿件的提交。
AUTHOR's CONTRIBUTIONS
GU Liangrui was responsible for data collection and analysis, and original draft writing. FANG Tonglei and YAN Bicong were responsible for statistical data verification and image selection. WU Jinliang participated in research design, supervision and writing guidance. All authors have read the final version of paper and agreed to submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
参考文献

{kind=link}
{kind=link}
{kind=link}
{kind=link}