Journal of Shanghai Jiao Tong University (Medical Science) ›› 2023, Vol. 43 ›› Issue (1): 36-43.doi: 10.3969/j.issn.1674-8115.2023.01.005
• Clinical research • Previous Articles Next Articles
WANG Fei( ), GONG Yan, XU Liya, LIU Qingxu, LI Yan, GUO Sheng, LI Pin()
), GONG Yan, XU Liya, LIU Qingxu, LI Yan, GUO Sheng, LI Pin()
Received:2022-07-18
Accepted:2022-11-09
Online:2022-12-20
Published:2022-12-20
Contact:
LI Pin
E-mail:w-fly0620 @163.com;lipin21@126.com
Supported by:CLC Number:
WANG Fei, GONG Yan, XU Liya, LIU Qingxu, LI Yan, GUO Sheng, LI Pin. Effect of short-term GnRH pulse therapy on pituitary-testicular function in adolescent male patients with congenital hypogonadotropic hypogonadism[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(1): 36-43.
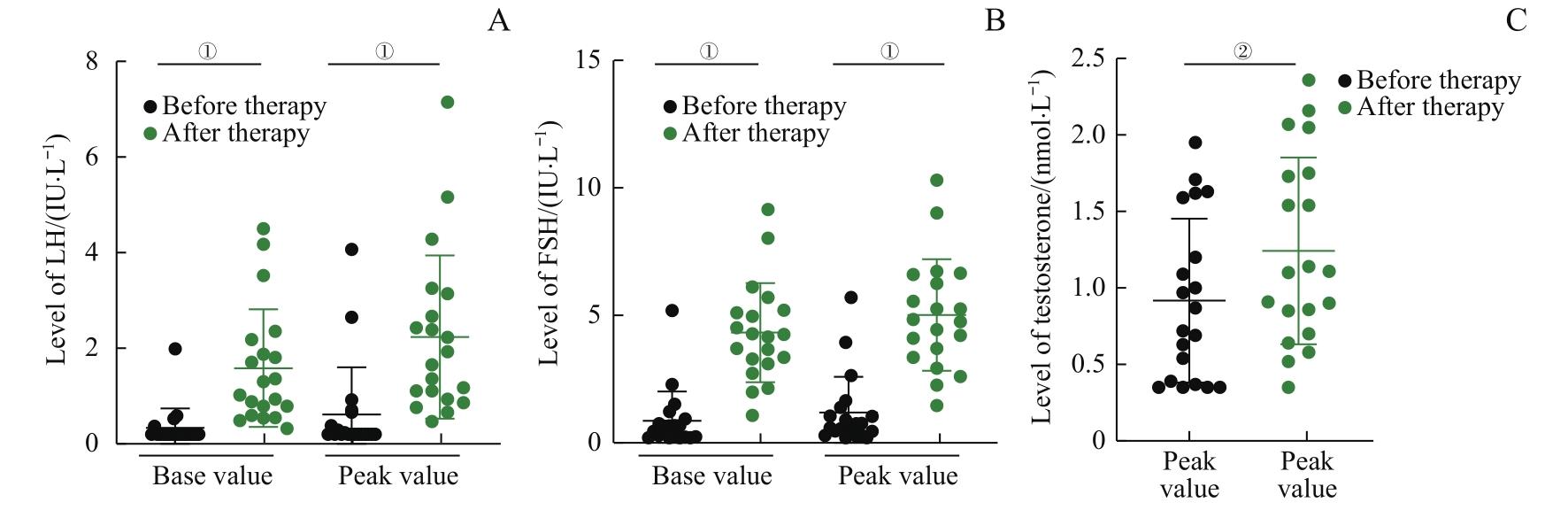
Fig 1 Changes of LH, FSH and testosterone levels in the adolescent boys with CHH after continuous GnRH pulse therapy for 1 week (n=20)
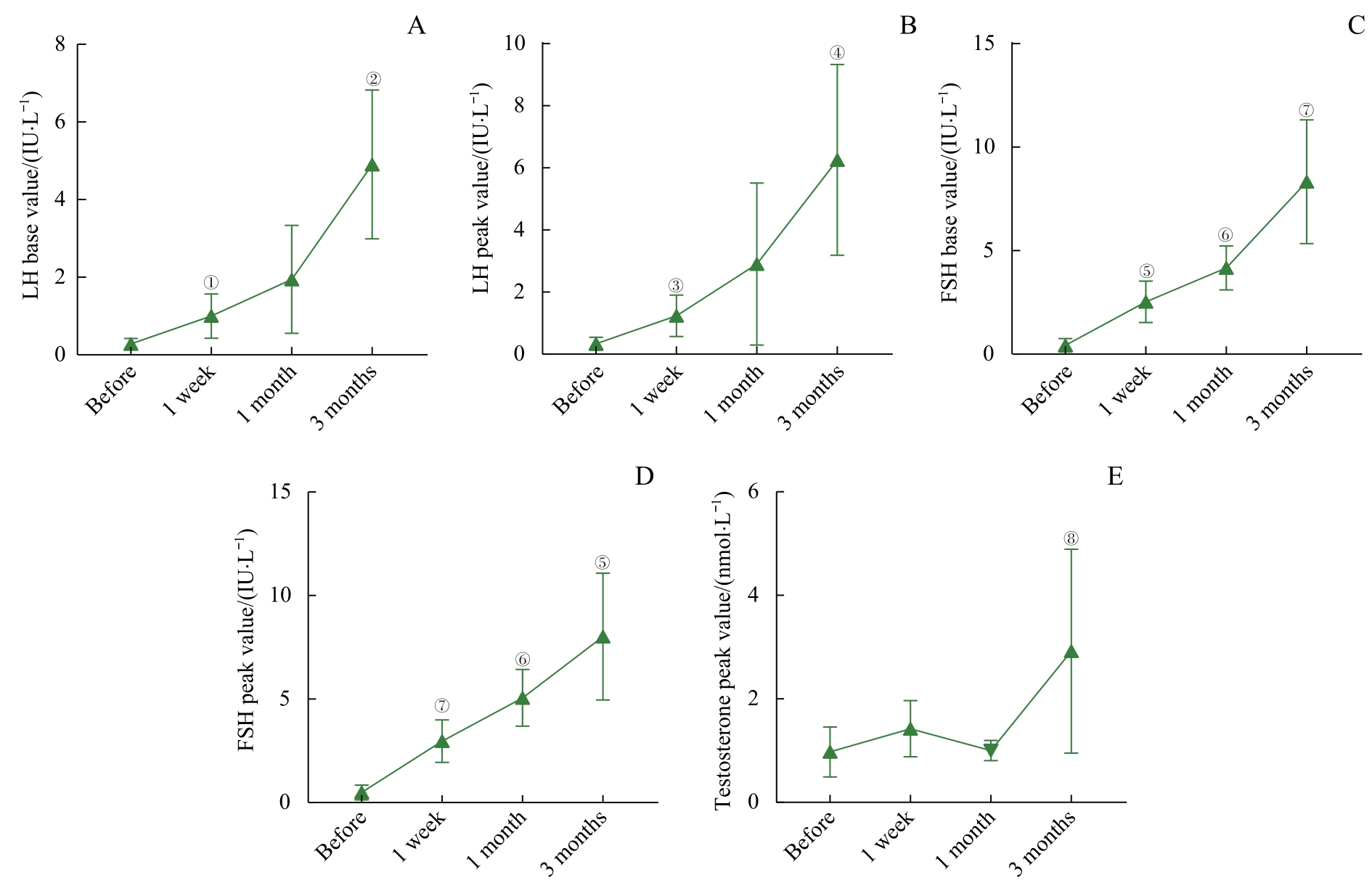
Fig 2 Changes of LH, FSH and testosterone levels in the adolescent boys with CHH during the continuous GnRH pulse therapy for 3 months (n=5)
| Gene | Inheritance | Variant | Amino acid | Type of variant | Pathogenicity | Source of variant |
|---|---|---|---|---|---|---|
| FGFR1 | AD | c.1695_1696 insT | p.Lys566Ter | Heterozygous | P | De novo |
| FGFR1 | AD | c.25G>A | p.Gly9Ser | Heterozygous | VUS | Mother |
| FGFR1 | AD | c.761G>A | p.Arg254Gln | Heterozygous | LP | Father |
| FGFR1 | AD | c.963dupA | p.Glu322Argfs*13 | Heterozygous | P | De novo |
| FGFR1 | AD | c.350A>G | p.Asn117Ser | Heterozygous | VUS | Mother |
| FGFR1 | AD | c.580G>T | p.Gly194Cys | Heterozygous | VUS | De novo |
| FGFR1 | AD | c.1981C>T | p.Arg661* | Heterozygous | P | De novo |
| ANOS1 | XLR | c.1267C>T | p.Arg423* | Hemigygote | P | Mother |
| ANOS1 | XLR | c.1897C>T | p.Arg631Ter | Hemigygote | P | Mother |
| ANOS1 | XLR | c.1525delA | p.Ser509Valfs*40 | Hemigygote | P | De novo |
| ANOS1 | XLR | c.463A>G | p.Asn155Asp | Hemigygote | VUS | De novo |
| PROKR2 | AD | c.991G>A | p.Val331Met | Heterozygous | VUS | Mother |
| PROKR2 | AD | c.533G>C | p.Trp178Ser | Heterozygous | VUS | De novo |
| PROK2 | AD | c.223-4C>A | Unknown | Heterozygous | VUS | De novo |
Tab 1 Gene variants in 14 CHH patients
| Gene | Inheritance | Variant | Amino acid | Type of variant | Pathogenicity | Source of variant |
|---|---|---|---|---|---|---|
| FGFR1 | AD | c.1695_1696 insT | p.Lys566Ter | Heterozygous | P | De novo |
| FGFR1 | AD | c.25G>A | p.Gly9Ser | Heterozygous | VUS | Mother |
| FGFR1 | AD | c.761G>A | p.Arg254Gln | Heterozygous | LP | Father |
| FGFR1 | AD | c.963dupA | p.Glu322Argfs*13 | Heterozygous | P | De novo |
| FGFR1 | AD | c.350A>G | p.Asn117Ser | Heterozygous | VUS | Mother |
| FGFR1 | AD | c.580G>T | p.Gly194Cys | Heterozygous | VUS | De novo |
| FGFR1 | AD | c.1981C>T | p.Arg661* | Heterozygous | P | De novo |
| ANOS1 | XLR | c.1267C>T | p.Arg423* | Hemigygote | P | Mother |
| ANOS1 | XLR | c.1897C>T | p.Arg631Ter | Hemigygote | P | Mother |
| ANOS1 | XLR | c.1525delA | p.Ser509Valfs*40 | Hemigygote | P | De novo |
| ANOS1 | XLR | c.463A>G | p.Asn155Asp | Hemigygote | VUS | De novo |
| PROKR2 | AD | c.991G>A | p.Val331Met | Heterozygous | VUS | Mother |
| PROKR2 | AD | c.533G>C | p.Trp178Ser | Heterozygous | VUS | De novo |
| PROK2 | AD | c.223-4C>A | Unknown | Heterozygous | VUS | De novo |
| Index | Gene mutation | Statistical value | P value | |
|---|---|---|---|---|
| FGFR1 (n=7) | ANOS1 (n=4) | |||
| Age/year | 14.90 (14.33, 15.42) | 14.75 (14.42, 15.39) | 0.378 | 0.705 |
| BMI/(kg·m-2) | 26.01 (22.89, 27.92) | 22.66 (15.71, 29.78) | 0.756 | 0.450 |
| Height/cm | 168.86 (162.80, 175.00) | 152.10 (147.90, 155.70) | 2.457 | 0.014 |
| Cryptorchid/n | 1 | 1 | ‒ | ‒ |
| Dysosmia/n | 2 | 2 | ‒ | ‒ |
| Testicular volume/mL | 1.12 (0.49, 2.00) | 0.86 (0.43, 1.24) | 0.213 | 0.831 |
| INHB/(pg·mL-1) | 31.03 (10.08, 53.92) | 41.09 (2.23, 79.84) | 0.189 | 0.850 |
| ΔLH base value/(IU·L-1)① | 0.82 (0.35, 1.98) | 0.71 (0.41, 2.09) | 0.095 | 0.925 |
| ΔLH peak value/(IU·L-1)① | 1.12 (0.56, 2.85) | 1.20 (0.59, 3.81) | 0.189 | 0.850 |
| ΔFSH base value/(IU·L-1)① | 2.59 (1.79, 4.75) | 2.16 (-0.06, 3.85) | 1.323 | 0.186 |
| ΔFSH peak value/(IU·L-1)① | 2.66 (1.67, 5.72) | 2.53 (-0.05, 5.10) | 0.567 | 0.571 |
| ΔTestosterone peak value/(nmol·L-1)① | 1.41 (0.90, 2.16) | 1.48 (0.78, 2.00) | 0.095 | 0.927 |
Tab 2 Comparison of clinical phenotypes between the CHH patients with FGFR1 and ANOS1 gene mutation
| Index | Gene mutation | Statistical value | P value | |
|---|---|---|---|---|
| FGFR1 (n=7) | ANOS1 (n=4) | |||
| Age/year | 14.90 (14.33, 15.42) | 14.75 (14.42, 15.39) | 0.378 | 0.705 |
| BMI/(kg·m-2) | 26.01 (22.89, 27.92) | 22.66 (15.71, 29.78) | 0.756 | 0.450 |
| Height/cm | 168.86 (162.80, 175.00) | 152.10 (147.90, 155.70) | 2.457 | 0.014 |
| Cryptorchid/n | 1 | 1 | ‒ | ‒ |
| Dysosmia/n | 2 | 2 | ‒ | ‒ |
| Testicular volume/mL | 1.12 (0.49, 2.00) | 0.86 (0.43, 1.24) | 0.213 | 0.831 |
| INHB/(pg·mL-1) | 31.03 (10.08, 53.92) | 41.09 (2.23, 79.84) | 0.189 | 0.850 |
| ΔLH base value/(IU·L-1)① | 0.82 (0.35, 1.98) | 0.71 (0.41, 2.09) | 0.095 | 0.925 |
| ΔLH peak value/(IU·L-1)① | 1.12 (0.56, 2.85) | 1.20 (0.59, 3.81) | 0.189 | 0.850 |
| ΔFSH base value/(IU·L-1)① | 2.59 (1.79, 4.75) | 2.16 (-0.06, 3.85) | 1.323 | 0.186 |
| ΔFSH peak value/(IU·L-1)① | 2.66 (1.67, 5.72) | 2.53 (-0.05, 5.10) | 0.567 | 0.571 |
| ΔTestosterone peak value/(nmol·L-1)① | 1.41 (0.90, 2.16) | 1.48 (0.78, 2.00) | 0.095 | 0.927 |
| 1 | CANGIANO B, SWEE D S, QUINTON R, et al. Genetics of congenital hypogonadotropic hypogonadism: peculiarities and phenotype of an oligogenic disease[J]. Hum Genet, 2021, 140(1): 77-111. |
| 2 | BIANCO S D C, KAISER U B. The genetic and molecular basis of idiopathic hypogonadotropic hypogonadism[J]. Nat Rev Endocrinol, 2009, 5(10): 569-576. |
| 3 | SWEE D S, QUINTON R. Current concepts surrounding neonatal hormone therapy for boys with congenital hypogonadotropic hypogonadism[J]. Expert Rev Endocrinol Metab, 2022, 17(1): 47-61. |
| 4 | HAO M, NIE M, YU B Q, et al. Gonadotropin treatment for male partial congenital hypogonadotropic hypogonadism in Chinese patients[J]. Asian J Androl, 2020, 22(4): 390-395. |
| 5 | GONG C X, LIU Y, QIN M, et al. Pulsatile GnRH is superior to hCG in therapeutic efficacy in adolescent boys with hypogonadotropic hypogonadodism[J]. J Clin Endocrinol Metab, 2015, 100(7): 2793-2799. |
| 6 | YOUNG J, XU C, PAPADAKIS G E, et al. Clinical management of congenital hypogonadotropic hypogonadism[J]. Endocr Rev, 2019, 40(2): 669-710. |
| 7 | 孙首悦, 王卫庆, 蒋怡然, 等. 微量泵脉冲输注戈那瑞林治疗特发性低促性腺激素性性腺功能减退症[J]. 中华内分泌代谢杂志, 2011, 27(8): 654-658. |
| SUN S Y, WANG W Q, JIANG Y R, et al. Treatment of idiopathic hypogonadotropic hypogonadism with pulse infusion of gonadorelin via micro pump[J]. Chinese Journal of Endocrinology and Metabolism, 2011, 27(8): 654-658. | |
| 8 | GACH A, PINKIER I, SAŁACIŃSKA K, et al. Identification of gene variants in a cohort of hypogonadotropic hypogonadism: diagnostic utility of custom NGS panel and WES in unravelling genetic complexity of the disease[J]. Mol Cell Endocrinol, 2020, 517: 110968. |
| 9 | WANG Y, GONG C X, QIN M, et al. Clinical and genetic features of 64 young male paediatric patients with congenital hypogonadotropic hypogonadism[J]. Clin Endocrinol (Oxf), 2017, 87(6): 757-766. |
| 10 | MAIONE L, DWYER A A, FRANCOU B, et al. Genetics in endocrinology: genetic counseling for congenital hypogonadotropic hypogonadism and Kallmann syndrome: new challenges in the era of oligogenism and next-generation sequencing[J]. Eur J Endocrinol, 2018, 178(3): R55-R80. |
| 11 | AMATO L G L, MONTENEGRO L R, LERARIO A M, et al. New genetic findings in a large cohort of congenital hypogonadotropic hypogonadism[J]. Eur J Endocrinol, 2019, 181(2): 103-119. |
| 12 | GACH A, PINKIER I, SZARRAS-CZAPNIK M, et al. Expanding the mutational spectrum of monogenic hypogonadotropic hypogonadism: novel mutations in ANOS1 and FGFR1 genes[J]. Reprod Biol Endocrinol, 2020, 18(1): 8. |
| 13 | LIU Q X, YIN X Q, LI P. Clinical, hormonal, and genetic characteristics of 25 Chinese patients with idiopathic hypogonadotropic hypogonadism[J]. BMC Endocr Disord, 2022, 22(1): 30. |
| 14 | FESTA A, UMANO G R, MIRAGLIA DEL GIUDICE E, et al. Genetic evaluation of patients with delayed puberty and congenital hypogonadotropic hypogonadism: is it worthy of consideration?[J]. Front Endocrinol (Lausanne), 2020, 11: 253. |
| 15 | KIM J H, SEO G H, KIM G H, et al. Targeted gene panel sequencing for molecular diagnosis of Kallmann syndrome and normosmic idiopathic hypogonadotropic hypogonadism[J]. Exp Clin Endocrinol Diabetes, 2019, 127(8): 538-544. |
| 16 | WANG Y, QIN M, FAN L J, et al. Correlation analysis of genotypes and phenotypes in Chinese male pediatric patients with congenital hypogonadotropic hypogonadism[J]. Front Endocrinol (Lausanne), 2022, 13: 846801. |
| 17 | LI S Y, ZHAO Y L, NIE M, et al. Clinical characteristics and spermatogenesis in patients with congenital hypogonadotropic hypogonadism caused by FGFR1 mutations[J]. Int J Endocrinol, 2020, 2020: 8873532. |
| 18 | NEOCLEOUS V, FANIS P, TOUMBA M, et al. GnRH deficient patients with congenital hypogonadotropic hypogonadism: novel genetic findings in ANOS1, RNF216, WDR11, FGFR1, CHD7, and POLR3A genes in a case series and review of the literature[J]. Front Endocrinol (Lausanne), 2020, 11: 626. |
| 19 | MOSBAH H, BOUVATTIER C, MAIONE L, et al. GnRH stimulation testing and serum inhibin B in males: insufficient specificity for discriminating between congenital hypogonadotropic hypogonadism from constitutional delay of growth and puberty[J]. Hum Reprod, 2020, 35(10): 2312-2322. |
| 20 | SEGAL T Y, MEHTA A, ANAZODO A, et al. Role of gonadotropin-releasing hormone and human chorionic gonadotropin stimulation tests in differentiating patients with hypogonadotropic hypogonadism from those with constitutional delay of growth and puberty[J]. J Clin Endocrinol Metab, 2009, 94(3): 780-785. |
| 21 | BINDER G, SCHWEIZER R, BLUMENSTOCK G, et al. Inhibin B plus LH vs GnRH agonist test for distinguishing constitutional delay of growth and puberty from isolated hypogonadotropic hypogonadism in boys[J]. Clin Endocrinol (Oxf), 2015, 82(1): 100-105. |
| 22 | GAO Y T, DU Q, LIU L Y, et al. Serum inhibin B for differentiating between congenital hypogonadotropic hypogonadism and constitutional delay of growth and puberty: a systematic review and meta-analysis[J]. Endocrine, 2021, 72(3): 633-643. |
| 23 | VARIMO T, MIETTINEN P J, KÄNSÄKOSKI J, et al. Congenital hypogonadotropic hypogonadism, functional hypogonadotropism or constitutional delay of growth and puberty? An analysis of a large patient series from a single tertiary center[J]. Hum Reprod, 2017, 32(1): 147-153. |
| 24 | 中华医学会内分泌学分会性腺学组. 特发性低促性腺激素性性腺功能减退症诊治专家共识[J]. 中华内科杂志, 2015, 54(8): 739-744. |
| Division of Gonadal Disease, Chinese Society of Endocrinology. Expert consensus on the diagnosis and treatment of idiopathic hypogonadotropic hypogonadism[J]. Chinese Journal of Internal Medicine, 2015, 54(8): 739-744. | |
| 25 | SHAH R, PATIL V, SARATHI V, et al. Prior testosterone replacement therapy may impact spermatogenic response to combined gonadotropin therapy in severe congenital hypogonadotropic hypogonadism[J]. Pituitary, 2021, 24(3): 326-333. |
| 26 | 中华医学会儿科学分会内分泌遗传代谢学组. 性发育异常的儿科内分泌诊断与治疗共识[J]. 中华儿科杂志, 2019, 57(6): 410-418. |
| The Subspecialty Group of Endocrinologic, Hereditary and Metabolic Diseases, the Society of Pediatrics, Chinese Medical Association. Consensus statement on the diagnosis and endocrine treatment of children with disorder of sex development[J]. Chinese Journal of Pediatrics, 2019, 57(6): 410-418. | |
| 27 | LIU Y, REN X Y, PENG Y G, et al. Efficacy and safety of human chorionic gonadotropin combined with human menopausal gonadotropin and a gonadotropin-releasing hormone pump for male adolescents with congenital hypogonadotropic hypogonadism[J]. Chin Med J (Engl), 2021, 134(10): 1152-1159. |
| Viewed | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
Full text 1424
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
Abstract 457
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||