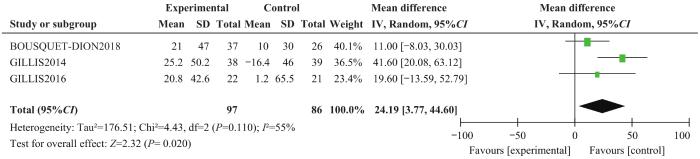
目的·系统评价预康复对择期行胃肠道手术患者术后恢复的影响。方法·系统检索PubMed、EMbase、Cochrane Library、Web of Science、CINAHL、中国生物医学文献数据库(CBM)、中国知网、万方、维普数据库,检索时限均为建库至2022年1月31日。按照预先设定的标准筛选文献,对文献质量进行评价并提取资料,对纳入的随机对照试验采用RevMan 5.4进行meta分析。主要观察指标为术后总体并发症发生率和手术部位感染发生率,次要观察指标为住院天数、6 min步行试验(6-minute walk test,6MWT)、医院焦虑抑郁量表(Hospital Anxiety and Depression Scale,HADS)评分,以及死亡率和预康复执行的依从性。结果·共纳入16篇文献,其中英文15篇,中文1篇,共1 616例研究对象,纳入研究的总体质量较好。Meta分析结果显示,相较于对照组,实施了预康复的试验组患者术后总体并发症的发生率降低[比值比(odds ratio,OR)=0.57,95%置信区间(confidence interval,CI)0.35~0.94,P=0.030],手术部位感染发生率降低(OR=0.64,95%CI 0.46~0.90,P=0.009),住院天数缩短[均数差值(mean difference,MD)=-2.45,95%CI -3.17~-1.73,P=0.000]。2组患者术前6MWT水平的差异无统计学意义;试验组术前6MWT水平相较于基线的提升程度优于对照组(MD=24.19,95%CI 3.77~44.60,P=0.020)。2组患者术前HADS评分和术后死亡率差异均无统计学意义。结论·预康复有利于降低胃肠道择期手术患者术后总体并发症发生率,尤其是手术部位感染发生率,从而缩短住院天数,有利于患者康复。
关键词:胃肠道手术
;
预康复
;
术后恢复
;
系统评价
;
meta分析
Abstract
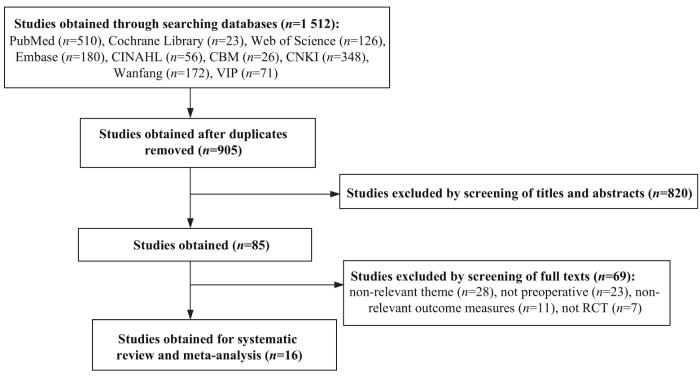
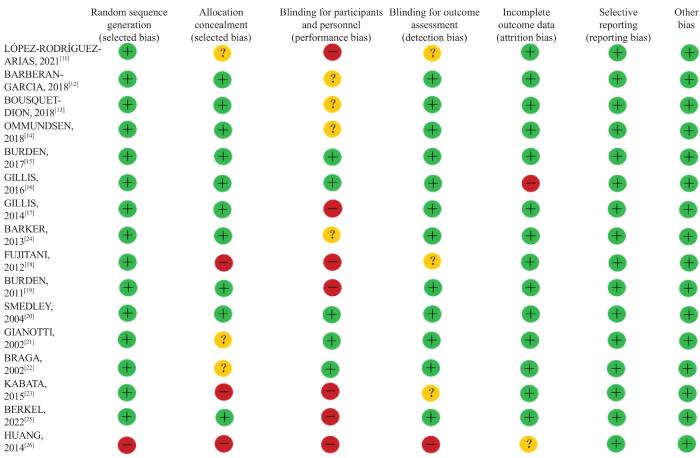
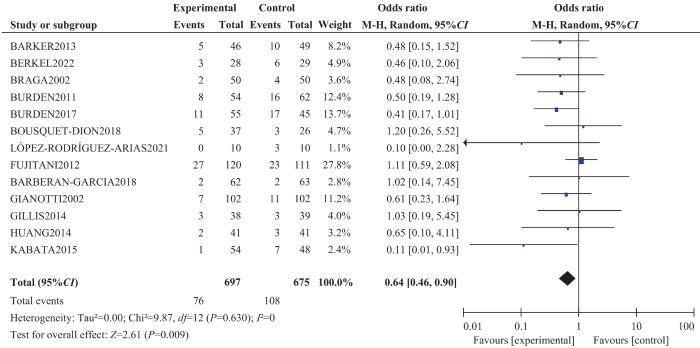
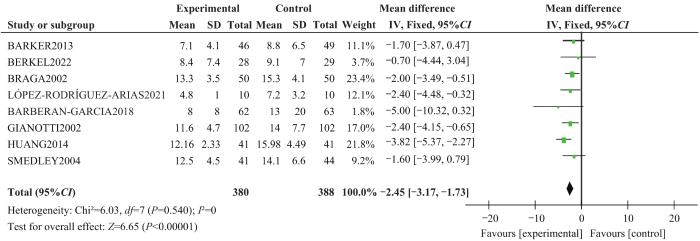
Objective ·To systematically evaluate the effect of prehabilitation on outcomes in patients undergoing elective gastrointestinal surgery. Methods ·PubMed, EMbase, Cochrane Library, Web of Science, CINAHL, Chinese BioMedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Wanfang and VIP Database were searched systematically from the establishment of each database to January 31, 2022. The literatures were screened, and evaluated according to the preset inclusion and exclusion criteria. The literature quality was evaluated and the data were extracted. Meta-analysis was performed on randomized controlled trials by using RevMan 5.4. The main observation indexes were the postoperative complication rate and the incidence of surgical site infection. The secondary indexes were hospitalization days, 6-minute walk test (6MWT), Hospital Anxiety and Depression Scale (HADS) score, mortality and compliance of prerehabilitation execution. Results ·Sixteen articles were included, including 15 articles in English and 1 article in Chinese, with a total of 1 616 patients. The overall quality of the included researches was good. The meta-analysis results showed that compared with the control group, the incidences of postoperative complications and surgical site infection were reduced [(odds ratio, OR)=0.57, 95% (confidence interval, CI)0.35‒0.94, P=0.030; OR=0.64, 95%CI 0.46‒0.90, P=0.009]; the length of hospital stay was shortened [mean difference (MD)=-2.45, 95%CI -3.17 ‒ -1.73, P=0.000] in the experimental group after the implementation of prehabilitation. There was no significant difference in preoperative 6MWT level between the two groups. Compared with the baseline, the change of 6MWT level before operation of the experimental group was bigger than that of the control group (MD=24.19, 95%CI 3.77‒44.60, P=0.020). There were no significant differences in the preoperative HADS score and the postoperative mortality between the two groups. Conclusion ·Prehabilitation can reduce the incidence of postoperative complications, especially surgical site infection, in patients undergoing elective gastrointestinal surgery, thus shortening the length of hospital stay and promoting the recovery of patients.
FANG Fang, TAI Rui, YU Qian, ZHANG Yaqing. Effect of prehabilitation on outcomes in patients undergoing elective gastrointestinal surgery: a systematic review. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(1): 70-78 doi:10.3969/j.issn.1674-8115.2023.01.009
外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面。围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3]。因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4]。“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5]。预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6]。近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价。随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8]。本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据。
1 资料与方法
本研究已在PROSPERO数据库注册,注册号为CRD42021288139。
1.1 文献纳入与排除标准
1.1.1 纳入标准
① 研究类型为随机对照试验(randomized controlled trial,RCT)。② 研究对象为初次行择期胃肠道手术的成年患者。③ 干预措施:试验组包括单独或者联合多种方式(多模式)实施术前预康复策略;对照组包括标准术前护理、给予安慰剂、仅术后康复、术前准备指导以及围术期常规护理(例如戒烟、戒酒等);2组术后执行一致的康复方案。④ 主要结局指标:术后总体并发症的发生率(采用Clavien-Dindo外科手术并发症分级系统[9]对术后的并发症进行定义和分级)、胃肠术后常见并发症手术部位感染(surgical site infection,SSI)发生率;次要结局指标:住院天数、6 min步行试验(6-minute walk test,6MWT)、医院焦虑抑郁量表(Hospital Anxiety and Depression Scale,HADS)评分,以及死亡率和预康复执行的依从性。
Adults, elective surgery for colon or rectal neoplasm
10/10
A 30-d trimodal prehabilitation program with recommendations on physical exercise, nutritional supplementation, and relaxation exercises to be performed at home before surgery and the first 30 d after hospital discharge
Adults, elective major abdominal surgery with high risk
62/63
A personalized prehabilitation program based on their health conditions and social circumstances which encompassed 3 major steps: motivational interview to assess the patients′ adherence profile and to codesign the characteristics of the physical activity program with the patient; personalized program to promote daily physical activity; supervised high-intensity endurance exercise training program
Adults, elective surgery for colon or rectal neoplasm
37/26
A 4-week multi-modal home-based exercise program with once-weekly supervision consisted of exercise intervention, nutritional intervention and anxiety-reduction strategies
Adults, elective surgery for colon or rectal neoplasm
22/21
A whey protein supplement was provided in a quantity that matched the patient′s need according to the estimated deficit in dietary protein intake for approximately 4 weeks leading up to the surgery
≤80 years, elective total gastrectomy, body weight loss of 10 percent or less within 6 months before entry
127/117
Preoperative oral supplementation of 1 000 mL/d in the form of an immunonutrient-enriched enteral feed added to normal diet for 5 d consecutively before the surgery
Adults, elective, radical gastroin-testinal, cancer surgery
41/41
Oral nutritional supplement (25 mL/kg) for 7 d before the surgery
Normal diet
Before discharge
①②⑥
Note: I—Intervention group; C—Control group. ① the rate of postoperative complications; ② length of hospital stay (day); ③ 6MWT;④ HADS; ⑤ mortality; ⑥ SSI; ⑦ compliance with the program.
The study was designed by ZHANG Yaqing and FANG Fang. TAI Rui and YU Qian completed the literature retrieval, literature quality evaluation and data extration. The meta-analysis was performed by FANG Fang and TAI Rui. The manuscript was drafted and revised by ZHANG Yaqing, FANG Fang, TAI Rui and YU Qian. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
MCDERMOTT F D, HEENEY A, KELLY M E, et al. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks[J]. Br J Surg, 2015, 102(5): 462-479.
GOVAERT J A, FIOCCO M, VAN DIJK W A, et al. Costs of complications after colorectal cancer surgery in the Netherlands: building the business case for hospitals[J]. Eur J Surg Oncol, 2015, 41(8): 1059-1067.
KIRCHHOFF P, CLAVIEN P A, HAHNLOSER D. Complications in colorectal surgery: risk factors and preventive strategies[J]. Patient Saf Surg, 2010, 4(1): 5.
GUSTAFSSON U O, SCOTT M J, HUBNER M, et al. Guidelines for perioperative care in elective colorectal surgery: enhanced recovery after surgery (ERAS®) society recommendations: 2018[J]. World J Surg, 2019, 43(3): 659-695.
LI C, CARLI F, LEE L, et al. Impact of a trimodal prehabilitation program on functional recovery after colorectal cancer surgery: a pilot study[J]. Surg Endosc, 2013, 27(4): 1072-1082.
CLAVIEN P A, BARKUN J, DE OLIVEIRA M L, et al. The Clavien-Dindo classification of surgical complications: five-year experience[J]. Ann Surg, 2009, 250(2): 187-196.
LÓPEZ-RODRÍGUEZ-ARIAS F, SÁNCHEZ-GUILLÉN L, ARANAZ-OSTÁRIZ V, et al. Effect of home-based prehabilitation in an enhanced recovery after surgery program for patients undergoing colorectal cancer surgery during the COVID-19 pandemic[J]. Support Care Cancer, 2021, 29(12): 7785-7791.
BARBERAN-GARCIA A, UBRÉ M, ROCA J, et al. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: a randomized blinded controlled trial[J]. Ann Surg, 2018, 267(1): 50-56.
BOUSQUET-DION G, AWASTHI R, LOISELLE S È, et al. Evaluation of supervised multimodal prehabilitation programme in cancer patients undergoing colorectal resection: a randomized control trial[J]. Acta Oncol, 2018, 57(6): 849-859.
OMMUNDSEN N, WYLLER T B, NESBAKKEN A, et al. Preoperative geriatric assessment and tailored interventions in frail older patients with colorectal cancer: a randomized controlled trial[J]. Colorectal Dis, 2018, 20(1): 16-25.
GILLIS C, LOISELLE S E, FIORE J F J R, et al. Prehabilitation with whey protein supplementation on perioperative functional exercise capacity in patients undergoing colorectal resection for cancer: a pilot double-blinded randomized placebo-controlled trial[J]. J Acad Nutr Diet, 2016, 116(5): 802-812.
GILLIS C, LI C, LEE L, et al. Prehabilitation versus rehabilitation: a randomized control trial in patients undergoing colorectal resection for cancer[J]. Anesthesiology, 2014, 121(5): 937-947.
FUJITANI K, TSUJINAKA T, FUJITA J, et al. Prospective randomized trial of preoperative enteral immunonutrition followed by elective total gastrectomy for gastric cancer[J]. Br J Surg, 2012, 99(5): 621-629.
BURDEN S T, HILL J, SHAFFER J L, et al. An unblinded randomised controlled trial of preoperative oral supplements in colorectal cancer patients[J]. J Hum Nutr Diet, 2011, 24(5): 441-448.
SMEDLEY F, BOWLING T, JAMES M, et al. Randomized clinical trial of the effects of preoperative and postoperative oral nutritional supplements on clinical course and cost of care[J]. Br J Surg, 2004, 91(8): 983-990.
GIANOTTI L, BRAGA M, NESPOLI L, et al. A randomized controlled trial of preoperative oral supplementation with a specialized diet in patients with gastrointestinal cancer[J]. Gastroenterology, 2002, 122(7): 1763-1770.
KABATA P, JASTRZĘBSKI T, KĄKOL M, et al. Preoperative nutritional support in cancer patients with no clinical signs of malnutrition: prospective randomized controlled trial[J]. Support Care Cancer, 2015, 23(2): 365-370.
BARKER L A, GRAY C, WILSON L, et al. Preoperative immunonutrition and its effect on postoperative outcomes in well-nourished and malnourished gastrointestinal surgery patients: a randomised controlled trial[J]. Eur J Clin Nutr, 2013, 67(8): 802-807.
BERKEL A E M, BONGERS B C, KOTTE H, et al. Effects of community-based exercise prehabilitation for patients scheduled for colorectal surgery with high risk for postoperative complications: results of a randomized clinical trial[J]. Ann Surg, 2022, 275(2): e299-e306.
HUANG Z J, CHEN B S, YOU J, et al. The clinical significance of preoperative enteral immune nutrition in patients with malignant gastrointestinal tumors[J]. Journal of Sichuan University (Medical Sciences), 2014, 45(1): 167-170.
ADIAMAH A, SKOŘEPA P, WEIMANN A, et al. The impact of preoperative immune modulating nutrition on outcomes in patients undergoing surgery for gastrointestinal cancer: a systematic review and meta-analysis[J]. Ann Surg, 2019, 270(2): 247-256.
REECE L, DRAGICEVICH H, LEWIS C, et al. Preoperative nutrition status and postoperative outcomes in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy[J]. Ann Surg Oncol, 2019, 26(8): 2622-2630.
WU X W, ZHANG X F, YANG Y Y, et al. Surgical site infection after colorectal surgery in China from 2018 to 2020[J]. Chinese Journal of Gastrointestinal Surgery, 2022, 25(9): 804-811.
KUANG R K, WANG C L, QIANG G H, et al. Analysis of the influencing factors for SSI in colorectal cancer patients with different nutrition disorder[J]. Parenteral & Enteral Nutrition, 2021, 28(2): 84-87.
ZHANG F F, HU Y J, HUANG H Y, et al. Association of CT-assessed sarcopenia with postoperative surgical site infections in patients with colorectal cancer[J]. Chinese General Practice, 2022, 25(29): 3658-3663.
GILLIS C, BUHLER K, BRESEE L, et al. Effects of nutritional prehabilitation, with and without exercise, on outcomes of patients who undergo colorectal surgery: a systematic review and meta-analysis[J]. Gastroenterology, 2018, 155(2): 391-410.e4.
YANG J, ZHANG T, FENG D, et al. A new diagnostic index for sarcopenia and its association with short-term postoperative complications in patients undergoing surgery for colorectal cancer[J]. Colorectal Dis, 2019, 21(5): 538-547.
MALIETZIS G, JOHNS N, AL-HASSI H O, et al. Low muscularity and myosteatosis is related to the host systemic inflammatory response in patients undergoing surgery for colorectal cancer[J]. Ann Surg, 2016, 263(2): 320-325.
MALIETZIS G, CURRIE A C, JOHNS N, et al. Skeletal muscle changes after elective colorectal cancer resection: a longitudinal study[J]. Ann Surg Oncol, 2016, 23(8): 2539-2547.
PECORELLI N, FIORE J F JR, GILLIS C, et al. The six-minute walk test as a measure of postoperative recovery after colorectal resection: further examination of its measurement properties[J]. Surg Endosc, 2016, 30(6): 2199-2206.
MOUG S J, BARRY S J E, MAGUIRE S, et al. Does prehabilitation modify muscle mass in patients with rectal cancer undergoing neoadjuvant therapy? A subanalysis from the REx randomised controlled trial[J]. Tech Coloproctol, 2020, 24(9): 959-964.
XU L, PAN Q, LIN R. Prevalence rate and influencing factors of preoperative anxiety and depression in gastric cancer patients in China: preliminary study[J]. J Int Med Res, 2016, 44(2): 377-388.
VAN ROOIJEN S, CARLI F, DALTON S, et al. Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: the first international randomized controlled trial for multimodal prehabilitation[J]. BMC Cancer, 2019, 19(1): 98.
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
0
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... 外科手术是大多数胃肠道肿瘤患者首选的治疗手段,但手术不可避免地给患者带来巨大的应激反应,包含生理(心跳加快、呼吸急促等)和心理(紧张、焦虑、易怒等)2个方面.围术期应激反应不利于患者的术后康复,甚至会导致术后并发症的发生,从而延长住院时间,增加医疗成本[1-3].因此,加速康复外科(enhanced recovery after surgery,ERAS)理念下围术期护理优化的重点在于减轻手术应激反应,改善患者术后的活动能力和营养状态[4].“预康复(prehabilitation)”的概念由ERAS延伸而来,指的是在择期手术前增强个体功能的过程,目的是提高机体面对大手术应激反应的耐受性,并试图在改善术后结局方面发挥作用[5].预康复的组成内容各不相同,一般包括运动锻炼、营养支持或心理干预3个部分[6].近年来,胃肠道手术预康复成为新的研究热点,已发表的研究包括多种不同的预康复方案和效果评价.随着新证据的出现,预康复对胃肠道手术术后结局的影响尚不明确[7-8].本研究旨在评价预康复的实施对胃肠道择期手术患者术后恢复的影响,以期为胃肠道手术患者的预康复临床实践提供循证依据. ...
1
... ① 研究类型为随机对照试验(randomized controlled trial,RCT).② 研究对象为初次行择期胃肠道手术的成年患者.③ 干预措施:试验组包括单独或者联合多种方式(多模式)实施术前预康复策略;对照组包括标准术前护理、给予安慰剂、仅术后康复、术前准备指导以及围术期常规护理(例如戒烟、戒酒等);2组术后执行一致的康复方案.④ 主要结局指标:术后总体并发症的发生率(采用Clavien-Dindo外科手术并发症分级系统[9]对术后的并发症进行定义和分级)、胃肠术后常见并发症手术部位感染(surgical site infection,SSI)发生率;次要结局指标:住院天数、6 min步行试验(6-minute walk test,6MWT)、医院焦虑抑郁量表(Hospital Anxiety and Depression Scale,HADS)评分,以及死亡率和预康复执行的依从性. ...
Adults, elective surgery for colon or rectal neoplasm
10/10
A 30-d trimodal prehabilitation program with recommendations on physical exercise, nutritional supplementation, and relaxation exercises to be performed at home before surgery and the first 30 d after hospital discharge
Standard care
12 weeks postoper-ative
①②⑥
BARBERAN-GARCIA, 2018[12]
Adults, elective major abdominal surgery with high risk
62/63
A personalized prehabilitation program based on their health conditions and social circumstances which encompassed 3 major steps: motivational interview to assess the patients′ adherence profile and to codesign the characteristics of the physical activity program with the patient; personalized program to promote daily physical activity; supervised high-intensity endurance exercise training program
Adults, elective surgery for colon or rectal neoplasm
10/10
A 30-d trimodal prehabilitation program with recommendations on physical exercise, nutritional supplementation, and relaxation exercises to be performed at home before surgery and the first 30 d after hospital discharge
Standard care
12 weeks postoper-ative
①②⑥
BARBERAN-GARCIA, 2018[12]
Adults, elective major abdominal surgery with high risk
62/63
A personalized prehabilitation program based on their health conditions and social circumstances which encompassed 3 major steps: motivational interview to assess the patients′ adherence profile and to codesign the characteristics of the physical activity program with the patient; personalized program to promote daily physical activity; supervised high-intensity endurance exercise training program
Adults, elective surgery for colon or rectal neoplasm
37/26
A 4-week multi-modal home-based exercise program with once-weekly supervision consisted of exercise intervention, nutritional intervention and anxiety-reduction strategies
Adults, elective surgery for colon or rectal neoplasm
22/21
A whey protein supplement was provided in a quantity that matched the patient′s need according to the estimated deficit in dietary protein intake for approximately 4 weeks leading up to the surgery
Placebo
4 weeks postoper-ative
③⑥
GILLIS, 2014[17]
Adults, elective surgery for colon or rectal neoplasm
38/39
A 4-week trimodal prehabilitation program at home included exercise intervention, nutrition intervention, and coping strategies to reduce anxiety
Adults, elective surgery for colon or rectal neoplasm
22/21
A whey protein supplement was provided in a quantity that matched the patient′s need according to the estimated deficit in dietary protein intake for approximately 4 weeks leading up to the surgery
Placebo
4 weeks postoper-ative
③⑥
GILLIS, 2014[17]
Adults, elective surgery for colon or rectal neoplasm
38/39
A 4-week trimodal prehabilitation program at home included exercise intervention, nutrition intervention, and coping strategies to reduce anxiety
≤80 years, elective total gastrectomy, body weight loss of 10 percent or less within 6 months before entry
127/117
Preoperative oral supplementation of 1 000 mL/d in the form of an immunonutrient-enriched enteral feed added to normal diet for 5 d consecutively before the surgery
Normal diet
Before discharge
①②⑥
BURDEN, 2011[19]
Adults, elective surgery for colon or rectal neoplasm
54/62
Oral supplementary drink of 400 mL daily, and dietary advice for 10 d before the operation
Dietary advice only
Before discharge
①②⑥
SMEDLEY, 2004[20]
Adults, elective moderate to severe lower gastrointestinal surgery
48/50
Oral nutritional supplement in small, frequent quantities between meals for 7 d before the operation, the volume consumed was recorded
≤80 years, elective total gastrectomy, body weight loss of 10 percent or less within 6 months before entry
127/117
Preoperative oral supplementation of 1 000 mL/d in the form of an immunonutrient-enriched enteral feed added to normal diet for 5 d consecutively before the surgery
Normal diet
Before discharge
①②⑥
BURDEN, 2011[19]
Adults, elective surgery for colon or rectal neoplasm
54/62
Oral supplementary drink of 400 mL daily, and dietary advice for 10 d before the operation
Dietary advice only
Before discharge
①②⑥
SMEDLEY, 2004[20]
Adults, elective moderate to severe lower gastrointestinal surgery
48/50
Oral nutritional supplement in small, frequent quantities between meals for 7 d before the operation, the volume consumed was recorded
≤80 years, elective total gastrectomy, body weight loss of 10 percent or less within 6 months before entry
127/117
Preoperative oral supplementation of 1 000 mL/d in the form of an immunonutrient-enriched enteral feed added to normal diet for 5 d consecutively before the surgery
Normal diet
Before discharge
①②⑥
BURDEN, 2011[19]
Adults, elective surgery for colon or rectal neoplasm
54/62
Oral supplementary drink of 400 mL daily, and dietary advice for 10 d before the operation
Dietary advice only
Before discharge
①②⑥
SMEDLEY, 2004[20]
Adults, elective moderate to severe lower gastrointestinal surgery
48/50
Oral nutritional supplement in small, frequent quantities between meals for 7 d before the operation, the volume consumed was recorded
≥60 years, elective surgery for colon or rectal neoplasm
28/29
A personalized 3-week (3 sessions per week, 9 sessions in total) supervised exercise program
Standard care
90 d postoper-ative
①②⑥
HUANG, 2014[26]
Adults, elective, radical gastroin-testinal, cancer surgery
41/41
Oral nutritional supplement (25 mL/kg) for 7 d before the surgery
Normal diet
Before discharge
①②⑥
Note: I—Intervention group; C—Control group. ① the rate of postoperative complications; ② length of hospital stay (day); ③ 6MWT;④ HADS; ⑤ mortality; ⑥ SSI; ⑦ compliance with the program. ...
≥60 years, elective surgery for colon or rectal neoplasm
28/29
A personalized 3-week (3 sessions per week, 9 sessions in total) supervised exercise program
Standard care
90 d postoper-ative
①②⑥
HUANG, 2014[26]
Adults, elective, radical gastroin-testinal, cancer surgery
41/41
Oral nutritional supplement (25 mL/kg) for 7 d before the surgery
Normal diet
Before discharge
①②⑥
Note: I—Intervention group; C—Control group. ① the rate of postoperative complications; ② length of hospital stay (day); ③ 6MWT;④ HADS; ⑤ mortality; ⑥ SSI; ⑦ compliance with the program. ...
≥60 years, elective surgery for colon or rectal neoplasm
28/29
A personalized 3-week (3 sessions per week, 9 sessions in total) supervised exercise program
Standard care
90 d postoper-ative
①②⑥
HUANG, 2014[26]
Adults, elective, radical gastroin-testinal, cancer surgery
41/41
Oral nutritional supplement (25 mL/kg) for 7 d before the surgery
Normal diet
Before discharge
①②⑥
Note: I—Intervention group; C—Control group. ① the rate of postoperative complications; ② length of hospital stay (day); ③ 6MWT;④ HADS; ⑤ mortality; ⑥ SSI; ⑦ compliance with the program. ...




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}