目的·描述儿童和青少年癌症患者多症状困扰及体力活动水平,并分析其多症状困扰的潜在剖面,探讨潜在剖面与体力活动的关系。方法·采用方便抽样的方法,选取2021年11月—2023年3月在上海交通大学医学院附属上海儿童医学中心血液/肿瘤科和附属新华医院小儿血液肿瘤科住院治疗或门诊就诊的10~18岁且治疗时间>1个月的儿童及青少年癌症患者。采用一般资料问卷、记忆症状评估量表(Memorial Symptom Assessment Scale 10-18,MSAS 10-18)、修订版儿童休闲活动调查问卷(Modified Chinese Version of Children′s Leisure Time Activities Study Survey,CLASS-C)进行资料收集。采用潜在剖面分析识别癌症患儿多症状困扰的水平是否存在人群异质性及其外显特征,并分析不同潜在症状剖面间体力活动水平是否存在差异。结果·共回收有效问卷165份,有效回收率91.7%。癌症患儿发生率前5位症状的困扰得分依次为缺乏体力1(1,2)分、恶心1(1,2)分、没有食欲2(2,3)分、出汗1(1,2)分、疼痛1(1,2)分。患儿以轻度体力活动为主,轻度体力活动水平中位数为2 530.00(1 577.50,3 721.00)min/周;中重度体力活动较少,为70.00(10.00,197.50)min/周。癌症患儿多症状困扰可分为2个潜在剖面,“高疲乏-高恶心-高头发减少-高昏昏欲睡”和“高疲乏-低恶心-低呕吐-低昏昏欲睡”,分别命名为高水平症状困扰(n=47,30.6%)和低水平症状困扰(n=118,69.4%)。多元Logistic回归分析显示,急性淋巴细胞白血病患儿归类为高水平症状困扰组的可能性高,最近一次就诊方式为门诊就诊的患儿归类为低水平症状困扰组的可能性高(均P<0.05);进一步分析显示经历高症状困扰患儿轻体力活动更高(P<0.05),中重度体力活动水平更低,但差异无统计学意义。结论·儿童和青少年癌症患者的多症状困扰水平存在人群异质性,疾病类型(急性淋巴细胞白血病)和最近一次就诊方式(门诊就诊)是癌症患儿症状困扰潜在剖面的预测因素;且经历高水平症状困扰的患儿轻度体力活动水平更高,中重度体力活动水平可能更低。
关键词:症状困扰
;
癌症
;
儿童
;
青少年
;
体力活动
;
潜在剖面分析
Abstract
Objective ·To describe the level of multiple symptom distress and physical activity in children and adolescents with cancer, analyze symptom distress profiles, and explicit the relationship between latent profiles and physical activity. Methods ·From November 2021 to March 2023, the convenient sample method was used to recruit children and adolescents with cancer aged 10-18 years old, who had been treated for more than 1 month in the Departments of Hematology/Oncology, Shanghai Children′s Medical Center and Xin Hua Hospital, Shanghai Jiao Tong University School of Medicine. The questionnaires, including General Information Questionnaire, Memorial Symptom Assessment Scale 10-18 (MSAS 10-18) and Modified Chinese Version of Children′s Leisure Time Activities Study Survey (CLASS-C), were used. Latent profile analysis was used to identify whether the level of multiple symptom distress in children and adolescents with cancer was population heterogeneity and its explicit characteristics. Whether there were differences in physical activity levels among different profiles of symptom distress was also analyzed. Results ·A total of 165 valid questionnaires were collected, with an effective response rate of 91.7%. The symptom distress scores of the top five occurrence rates of symptoms in children and adolescents with cancer were lack of energy with a median of 1 (1, 2) point, nausea 1 (1, 2) point, lack of appetite 2 (2, 3) points, sweat 1 (1, 2) point, and pain 1 (1, 2) point. The physical activity level of the patients was mainly light, with a median of 2 530.00 (1 577.50, 3 721.00) min/week, and moderate to vigorous physical activity was relatively lower [70.00 (10.00, 197.50) min/week]. The patients with cancer could be divided into two latent profiles: "high fatigue-high nausea-high hair loss-high sleepy" and "high fatigue-low nausea-low vomiting-low sleepy", which were named as high symptom distress (n=47, 30.6%) and low symptom distress (n=118, 69.4%) separately. Multivariate Logistic regression analysis showed that patients with acute lymphoblastic leukemia were more likely to be classified as high symptom distress group, and outpatients in the latest hospital visit were more likely to classified as low symptom distress group (both P<0.05). In addition, patients with high symptom distress had a higher level of light physical activity (P<0.05), and had a lower level of moderate to vigorous physical activity, but the difference was not statistically significant. Conclusion ·There is population heterogeneity in the multiple symptom distress in children and adolescents with cancer. Disease type (acute leukemia) and the way of the latest hospital visit (through outpatient department) are the predictors of symptoms profiles of patients with cancer. Patients who experience high symptom distress have higher level of light physical activity, and perhaps lower level of moderate to vigorous physical activity.
Keywords:symptom distress
;
cancer
;
child
;
adolescent
;
physical activity
;
latent class analysis
LIU Yanyan, YANG Tiantian, SHEN Nanping, HE Mengxue, ZHANG Hongyan. Latent profile analysis of multiple symptom distress in children and adolescents with cancer and its effect on their physical activity. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(11): 1408-1416 doi:10.3969/j.issn.1674-8115.2023.11.008
儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制。该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为。杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83。修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间。每一部分的体力活动得分为过去一周内各类活动时间的总和。
采用Mplus 8.0进行潜在剖面分析[22]。模型适配指标包括:① 赤池信息量准则(Akaike information criteria,AIC)、贝叶斯信息准则(Bayesian information criteria,BIC)和校正BIC(adjusted BIC,aBIC),数值越小表示模型拟合越好。② 熵(entropy)值范围为0~1,越接近1表示分类越精确;当Entropy=0.8时,提示分类精确率>90%。③ 采用LMR似然比检验(Lo-Mendell-Rubin likelihood ratio test,LMRT)、aLMR似然比检验(adjusted Lo-Mendell-Rubin likelihood ratio test,aLMRT)和基于bootstrap的似然比检验(bootstrapped likelihood ratio test,BLRT)用于模型比较。P<0.05时表示第K个模型拟合优于第(K-1)个模型。综合上述指标,从单一类别模型开始,逐步增加模型中的类别数目,直至拟合指标达到最佳。
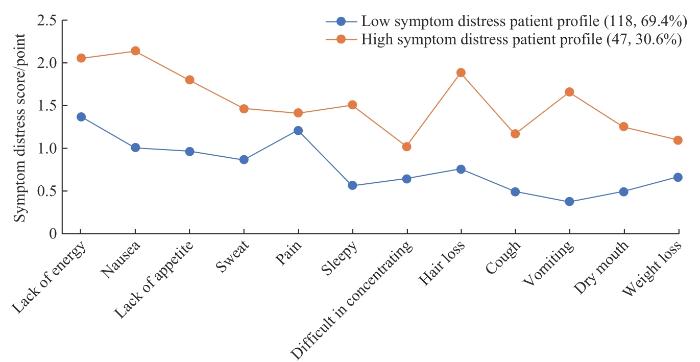
采用以个体为中心的潜在剖面分析可以更深入了解患儿经历的多症状潜在组别。本研究确定的最佳模型为高水平症状困扰和低水平症状困扰2个潜在组别,同时也证明了癌症患儿经历的多症状困扰具有人群异质性。WU等[33]和BUCKNER等[11]的研究同样证实这一点。WU等[33]的研究将癌症患儿治疗期疲乏、疼痛等13个症状分为症状轻度困扰、中度困扰和重度困扰3个类别;BUCKNER等[11]将癌症患儿焦虑、抑郁、疲乏、疼痛及身体功能状态分为4个类别。WANG等[34]采用儿童患者报告结局测量信息系统(Patient-Reported Outcomes Measurement Information System,PROMIS)简表评估患儿化疗期间症状及身体功能纵向变化,并将其变化轨迹分为2个类别。现有研究显示,因纳入症状数量和类型的不同,多症状困扰潜在组别存在差异,这需要后续研究进一步探讨。本研究2组患儿困扰水平均较高的症状包括疲乏、昏昏欲睡等躯体症状,恶心、呕吐、没有食欲等消化道症状以及与自身形象有关的症状(如脱发)等,这一发现与WU等[33]和AMERINGER等[35]的研究相一致,提示这些症状均是研究和实践中需要干预的重点。该结果也提示癌症患儿经历的症状困扰存在明显的人群差异性,特别是对高水平症状困扰的患儿需要给予更高频次的评估及精准干预。
The study was designed by LIU Yanyan and SHEN Nanping. The data collection and data collation were carried out by HE Mengxue and ZHANG Hongyan. The data collation and analysis were finished by LIU Yanyan and YANG Tiantian. The manuscript was drafted and revised by LIU Yanyan, YANG Tiantian and SHEN Nanping. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
World Health Organization. WHO launches new tools to help countries build effective childhood cancer programmes[EB/OL]. (2021-02-15)[2023-06-17]. https://www.who.int/news/item/15-02-2021-who-launches-new-tools-to-help-countries-build-effective-childhood-cancer-programmes.
STELIAROVA-FOUCHER E, COLOMBET M, RIES L A G, et al. International incidence of childhood cancer, 2001-10: a population-based registry study[J]. Lancet Oncol, 2017, 18(6): 719-731.
HE S, YOU L M, ZHENG J, et al. Uncertainty and personal growth through positive coping strategies among Chinese parents of children with acute leukemia[J]. Cancer Nurs, 2016, 39(3): 205-212.
BERDAN C A, TANGNEY C C, SCALA C, et al. Childhood cancer survivors and adherence to the American Cancer Society guidelines on nutrition and physical activity[J]. J Cancer Surviv, 2014, 8(4): 671-679.
Children′s Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers. Version 5.0[EB/OL]. [2023-02-17]. http://www.survivorshipguidelines.org/pdf/2018/COG_LTFU_Guidelines_v5.pdf.
GÖTTE M, KESTING S, WINTER C, et al. Comparison of self-reported physical activity in children and adolescents before and during cancer treatment[J]. Pediatr Blood Cancer, 2014, 61(6): 1023-1028.
WU W W, YU T H, JOU S T, et al. Physical activity self-efficacy mediates the effect of symptom distress on exercise involvement among adolescents undergoing cancer treatment[J]. Eur J Cancer Care (Engl), 2019, 28(4): e13045.
OUYANG N, CAI R Q, GONG N, et al. The barriers of physical activity for children with malignant tumor during treatment: a qualitative study[J]. Nursing Journal of Chinese People′s Liberation Army, 2019, 36(3): 33-36, 41.
BUCKNER T W, WANG J C, DEWALT D A, et al. Patterns of symptoms and functional impairments in children with cancer[J]. Pediatr Blood Cancer, 2014, 61(7): 1282-1288.
Chinese Children′s Cancer Group Acute Lymphoblastic Leukemia 2015 Study Group. Report of Chinese Children′s Cancer Group acute lymphoblastic leukemia 2015 multicenter study[J]. Chinese Journal of Pediatrics, 2022, 60(10): 1002-1010.
Hematology Group of the Pediatrics Branch of the Chinese Medical Association, Pediatrics Committee of the Chinese Anti-Cancer Association. Recommendations for the diagnosis and treatment of children with Hodgkin′s lymphoma[J]. Chinese Journal of Pediatrics, 2014, 52(8): 586-589.
ZHANG G W, ZHAO C L, LUO N, et al. Predictive value of CT imaging features in preoperative high-risk group of childhood hepatoblastoma[J]. Chinese Journal of Radiology, 2021, 55(9): 981-986.
PORTENOY R K, THALER H T, KORNBLITH A B, et al. The Memorial Symptom Assessment Scale: an instrument for the evaluation of symptom prevalence, characteristics and distress[J]. Eur J Cancer, 1994, 30(9): 1326-1336.
FENG F M, LOU J H, XU H, et al. Symptom experience among children with cancer: a cross-sectional study[J]. Chinese Nursing Management, 2012, 12(1): 30-34.
TELFORD A, SALMON J, JOLLEY D, et al. Reliability and validity of physical activity questionnaires for children: the Children′s Leisure Activities Study Survey (CLASS)[J]. Pediatr Exerc Sci, 2004, 16(1): 64-78.
HUANG Y J, WONG S H S, SALMON J. Reliability and validity of the modified Chinese version of the Children′s Leisure Activities Study Survey (CLASS) questionnaire in assessing physical activity among Hong Kong children[J]. Pediatr Exerc Sci, 2009, 21(3): 339-353.
LI H Y, CHEN P J, ZHUANG J. Revision and reliability validity amassment of Children′s Leisure Activities Study Survey[J]. Chinese Journal of School Health, 2011, 32(3): 268-270.
ZHENG Y, LIU K, BU X Q, et al. Survey and analysis of symptom clusters in children with acute leukemia during chemotherapy[J]. Chinese Journal of Nursing, 2016, 51(11): 1320-1324.
SADRUDDIN M M, HAMEED-UR-REHMAN M. Understanding the perceptions of children battling cancer about self and others through drawing[J]. South Asian J Cancer, 2013, 2(3): 113-118.
BELUM V R, WASHINGTON C, PRATILAS C A, et al. Dermatologic adverse events in pediatric patients receiving targeted anticancer therapies: a pooled analysis[J]. Pediatr Blood Cancer, 2015, 62(5): 798-806.
CHUNG O K, LI H C W, CHIU S Y, et al. The impact of cancer and its treatment on physical activity levels and behavior in Hong Kong Chinese childhood cancer survivors[J]. Cancer Nurs, 2014, 37(3): E43-E51.
GRIMSHAW S L, TAYLOR N F, MECHINAUD F, et al. Physical activity for children undergoing acute cancer treatment: a qualitative study of parental perspectives[J]. Pediatr Blood Cancer, 2020, 67(6): e28264.
LAM K K, HO CHEUNG WILLIAM L, HO K Y E, et al. Factors contributing to the low physical activity level for Hong Kong Chinese children hospitalised with cancer: an exploratory study[J]. J Clin Nurs, 2017, 26(1/2): 190-201.
OUYANG N, CAI R Q, ZHOU X Z, et al. Effects of a group-based physical activity program for pediatric patients with cancer on physical activity and symptom experience: a quasi-experimental study[J]. Pediatr Blood Cancer, 2019, 66(11): e27965.
CHEUNG A T, LI W H C, HO L L K, et al. Efficacy of mobile instant messaging-delivered brief motivational interviewing for parents to promote physical activity in pediatric cancer survivors: a randomized clinical trial[J]. JAMA Netw Open, 2022, 5(6): e2214600.
WU W W, LIN K C, LIANG S Y, et al. Using a patient-centered approach to identify symptom clusters among adolescents with cancer[J]. Cancer Nurs, 2019, 42(3): 198-207.
WANG J C, JACOBS S, DEWALT D A, et al. A longitudinal study of PROMIS pediatric symptom clusters in children undergoing chemotherapy[J]. J Pain Symptom Manage, 2018, 55(2): 359-367.
AMERINGER S, ELSWICK R K Jr, SHOCKEY D P, et al. A pilot exploration of symptom trajectories in adolescents with cancer during chemotherapy[J]. Cancer Nurs, 2013, 36(1): 60-71.
XU Y H. A pilot heterogeneity research of multiple symptom patterns in children with leukemia based on latent profile analysis[D]. Shanghai: Shanghai Jiao Tong University, 2018.
SAMPASA-KANYINGA H, COLMAN I, GOLDFIELD G S, et al. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: a systematic review[J]. Int J Behav Nutr Phys Act, 2020, 17(1): 72.
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 儿童休闲活动调查问卷(Children′s Leisure Time Activities Study Survey,CLASS)由澳大利亚迪肯大学TELFORD等[18]于2004年编制.该工具经修订先后应用于中国香港[19]和内地[20]健康儿童,评估其体力活动及静坐行为.杨静[21]根据恶性肿瘤对患儿学习及生活等活动的影响,对该工具进行了修订,形成修订版CLASS(Modified Chinese Version of CLASS,CLASS-C),应用于癌症患儿的重测信度为0.83.修订后的问卷分为2个部分:第一部分用于询问过去一周内进行9种轻度体力活动次数和时间;第二部分用于询问过去一周内参加16种中等强度以上(中重度)体力活动的次数和时间.每一部分的体力活动得分为过去一周内各类活动时间的总和. ...
1
... 采用Mplus 8.0进行潜在剖面分析[22].模型适配指标包括:① 赤池信息量准则(Akaike information criteria,AIC)、贝叶斯信息准则(Bayesian information criteria,BIC)和校正BIC(adjusted BIC,aBIC),数值越小表示模型拟合越好.② 熵(entropy)值范围为0~1,越接近1表示分类越精确;当Entropy=0.8时,提示分类精确率>90%.③ 采用LMR似然比检验(Lo-Mendell-Rubin likelihood ratio test,LMRT)、aLMR似然比检验(adjusted Lo-Mendell-Rubin likelihood ratio test,aLMRT)和基于bootstrap的似然比检验(bootstrapped likelihood ratio test,BLRT)用于模型比较.P<0.05时表示第K个模型拟合优于第(K-1)个模型.综合上述指标,从单一类别模型开始,逐步增加模型中的类别数目,直至拟合指标达到最佳. ...



{kind=link}
{kind=link}