

川崎病(Kawasaki disease,KD),又称皮肤黏膜淋巴结综合征,1967年由日本医师川崎富作首次报道,是多发于5岁以下儿童的急性系统性血管炎症疾病[1]。目前川崎病病因不明,多数认为是由感染因素触发的急性免疫性血管炎症疾病,可并发冠状动脉(冠脉)病变(coronary artery lesion)。对于一些存在严重冠脉病变的川崎病患儿,其冠脉病变可随时间逐年进展[2]。目前,作为川崎病合并冠脉病变患儿最常规的随访手段,二维超声心动图(心超)对于严重冠脉病变的患儿,尤其是存在冠脉狭窄及闭塞的病例,存在一定的漏诊及误诊情况[3-4]。而冠状动脉造影(coronary angiography,CAG)是冠脉病变诊断的金标准,可以全面准确地了解冠脉病变情况。本研究旨在将存在严重冠脉病变的川崎病患儿的CAG复查结果进行总结,对比分析CAG复查前后冠脉病变的进展情况,并将复查前的心超与CAG对冠脉病变的评价进行对比分析。
1 对象和方法
1.1 研究对象
1.2 研究方法
心超使用Philips SONOS 7500型、iE33超声诊断仪。采用S5-1或S8-3探头,探头射频4~8 MHz。患儿取仰卧位,行常规二维及彩色多普勒心超检查。测量患儿左主干(left main coronary artery,LM)、左前降支(left anterior descending branch,LAD)、左回旋支(left circumflex artery,LCX)和右冠状动脉(right coronary artery,RCA)的近、中、远段及后室间沟内径。记录有无冠脉瘤及其大小、位置,有无异常回声,冠脉内血流情况,室壁运动情况及左室射血分数(left ventricular ejection fraction,LVEF)。
CAG使用Philips UNIQ Clarity FD20数字减影血管造影X线机,造影剂为优维显(碘普罗胺)。吸入全身麻醉下,根据患儿体质量及年龄选择相应的血管鞘,经皮穿刺股动脉置入血管鞘,予100 U/kg肝素抗凝。应用4F或5F猪尾导管经股动脉逆行至主动脉根部,注射造影剂行主动脉根部造影(正侧位),观察左、右冠脉全程形态及走行。显影不佳时行左、右冠脉选择性造影,术中持续监测心电图、血压和血氧饱和度。记录有无冠脉瘤及其位置、大小,有无充盈缺损或钙化,有无狭窄或闭塞,及侧支循环形成情况。
1.3 统计学方法
应用SPSS 26.0软件进行统计分析,定量资料用M(最小值~最大值)表示,定性资料用频数(百分比)表示。心超与CAG测量冠脉瘤大小的差异采用Bland-Altman一致性检验进行分析。
2 结果
2.1 一般情况
21例患儿中男15例(71.4%)、女6例(28.6%),中位发病年龄为3岁6个月(1个月~12岁11个月);其中16例行2次CAG,2例行3次CAG,3例行4次CAG。本研究取患儿第2次CAG时年龄作为复查年龄。初次CAG的中位年龄为7岁11个月(7个月~13岁8个月),发病时间与初次CAG中位间隔时间为4年5个月;CAG复查的中位年龄为9岁2个月,与初次CAG中位间隔时间为1年3个月。
21例患儿中初次造影前共有8例出现明显临床症状,其中活动耐量下降2例,胸部不适3例(心前区钝痛1例、胸骨后刺痛1例、胸骨后紧缩感1例),胸闷2例,反复晕厥1例,纳差、水肿、少尿1例。
初次造影后有6例行冠状动脉旁路移植术(coronary artery bypass grafting,CABG),并在1年后复查CAG。另15例患儿在后续随访中心超发现病变进展后再行CAG复查,其中8例患儿冠脉病变存在不同程度的恶化,并有1例患儿于术中行冠状动脉球囊扩张,1例复查后行CABG。
2.2 初次CAG情况
21例患儿初次CAG检查,有13例患儿发生冠脉狭窄或闭塞。13例患儿中LM狭窄1例,LAD均匀性狭窄1例,LAD瘤后闭塞伴侧支形成2例,RCA中段闭塞伴侧支形成、LCX扩张后远端供应RCA 1例,RCA中段闭塞、LAD血管钙化狭窄、LCX扩张后远端供应RCA及LAD远端2例,RCA串珠样改变伴狭窄及侧支形成1例,RCA近段瘤后闭锁伴侧支形成3例,RCA近段闭锁钙化伴LAD近段狭窄1例,LCX巨大血栓导致血流闭塞1例。此13例冠脉狭窄或闭塞的患儿病变复杂,大都为冠脉瘤后并发冠脉狭窄及闭塞,且伴有不同程度的侧支形成;其中7例在CAG检查后结合心超结果,在原阿司匹林和华法林的基础上加用美托洛尔,6例CAG后行CABG,并有1例同时行室壁瘤切除术。
初次CAG检查另外8例未发现冠脉狭窄的患儿中,5例为双侧冠脉瘤,3例为单侧冠脉瘤;包括RCA近中段串珠样改变1例、LM至LAD大型冠脉瘤伴RCA近段大型冠脉瘤1例(图1)、LM及RCA近段大型冠脉瘤扩张1例、RCA及LAD中远段多发中小瘤样改变1例、RCA近段大型冠脉瘤样改变伴LAD小瘤改变2例、LAD瘤样改变2例。此8例患儿在CAG检查后继续口服华法林和阿司匹林治疗,未加用额外药物,继续随访。
图1
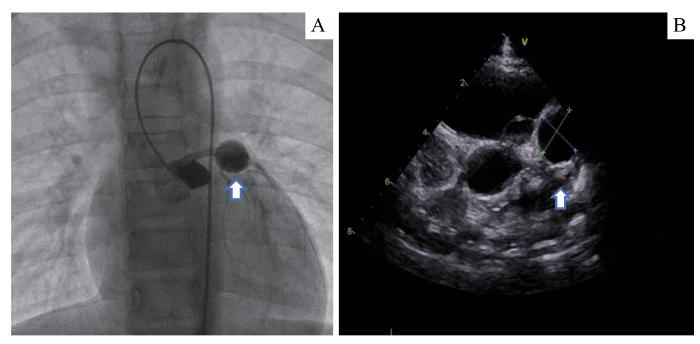
图1
川崎病患儿的冠脉瘤CAG与相应的心超影像
Note:A girl, 8 years and 7 months old, had been found to have coronary artery dilatation for 4 years. CAG (A) found a large coronary aneurysm (arrow), 12 mm×11 mm, in the proximal segment of LM, and the echocardiography (B) also found a coronary aneurysm (arrow) at the corresponding site.
Fig 1
CAG and corresponding echocardiography of a coronary aneurysm in a patient with KD
2.3 CAG复查情况
21例患儿复查CAG,有8例发现病变较前明显进展,7例未发现明显进展;另6例患儿在初次CAG后行CABG手术,1年后常规行CAG复查,复查显示桥血管通畅,未见明显狭窄。
在8例病变进展的患儿中,有2例出现临床症状:1例出现胸痛,1例出现反复晕厥。5例复查后发现原冠脉狭窄较初次CAG检查明显进展,侧支循环丰富;并有2例出现冠脉闭锁,其中1例术中即行冠脉内球囊扩张术,1例术后行CABG与室壁瘤切除术。另3例复查后发现冠脉扩张较前进展,扩张程度均较初次CAG检查显著。具体见表1。
表1 8例冠脉病变进展的川崎病患儿的详细复查资料
Tab 1
| No. | Gender | Age of first CAG | Result of first CAG | Age of CAG review | Result of CAG review | ||
|---|---|---|---|---|---|---|---|
| 1 | Male | 13 years | 13 years and 7 months | 17 years and 2 months | |||
| 2 | Male | 6 months | 3 years and 6 months | S | 7 years and 6 months (chest pain for 10 d) | ||
| 3 | Male | 3 years | 3 years and 3 months | 4 years and 3 months | |||
| 4 | Male | 4 months | 4 years | 6 years | |||
| 5 | Female | 2 years and 4 months | 3 years | 3 years and 9 months | |||
| 6 | Male | 2 years | 5 years | 7 years | |||
| 7 | Male | 9 years | 12 years (2 times of syncope in 3 years) | 15 years | |||
| 8 | Female | 2 years | 3 years | 4 years and 5 months |
2.4 心脏超声与CAG的结果对比
表2 21例患儿初次造影以及同期心超中冠脉病变的位置、类型 (n)
Tab 2
| Detection method | Coronary artery aneurysm | ||||||
|---|---|---|---|---|---|---|---|
| LM | LAD | RCA | LCX | LM | LAD | RCA | |
| CAG | 6 | 15 | 23 | 4 | 1 | 8 | 7 |
| Echocardiography | 8 | 15 | 25 | 3 | 1 | 0 | 0 |
图2
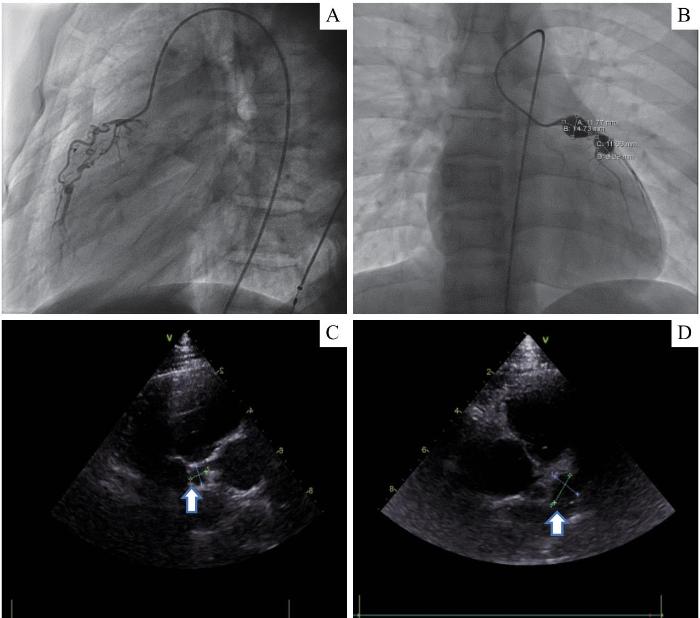
图2
CAG和心超对同一患者冠脉瘤和冠脉狭窄病变的影像对比
Note: A boy, aged 15 years and 8 months, had been found to have coronary artery aneurysm for 9 years. A. CAG showed stenosis of the proximal and middle segment of the RCA, close to atresia, and the formation of bridging collaterals. B. Two large coronary artery aneurysms with calcification were found by CAG in the proximal segment of the LAD, with the size of 14.73 mm×11.77 mm and 11.66 mm×8.89 mm, respectively. C/D. The corresponding echocardiography of this patient revealed 2 aneurysms in the LAD (arrows), while the RCA was not clearly visualized, and stenosis or atresia was not found.
Fig 2
Comparison of images of the same patient with coronary artery aneurysms and stenosis between CAG and echocardiography
最后,我们取初次CAG与邻近时间段内的心超对冠脉瘤最大直径的测量结果,针对2种检测手段的差值进行Bland-Altman分析,检验仅针对28处中大型冠脉瘤(最大直接≥4 mm)。Bland-Altman分析(图3)显示:2种检测手段测量冠脉瘤最大直径的差值为(1.63±2.33)mm,95%一致性界限为-2.95~6.21 mm。该界限超出了临床可接受的范畴,因此认为心超测量冠脉瘤大小存在一定的误差。
图3
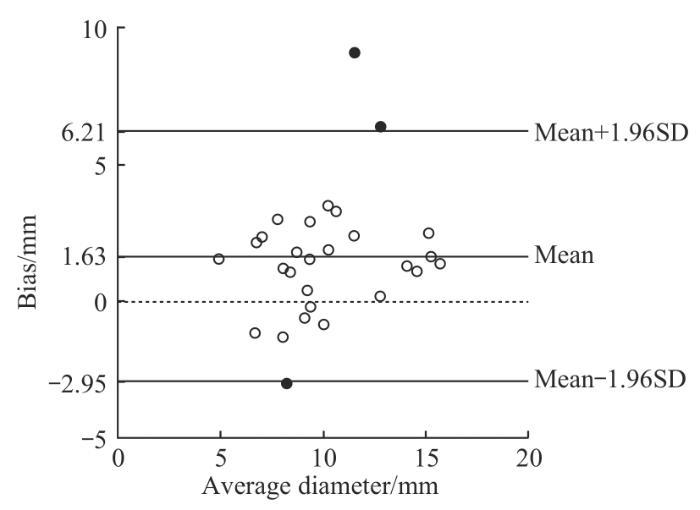
图3
CAG与心超测量中大型冠脉瘤直径的Bland-Altman一致性分析
Fig 3
Bland-Altman analysis of diameter measurements of medium and large coronary aneurysms by CAG and echocardiography
3 讨论
由于冠脉病变等级Ⅳ级及以上的患儿的冠脉瘤不会完全消退,并有一定概率进展为闭塞性病变,因此国内外指南[1,5-6]建议应在川崎病恢复早期行CAG以明确病变程度,之后的随访手段及频率因人而异,并没有指南明确对严重冠脉病变的患儿CAG复查的频率,但均强调针对此类患儿应进行个体化评估及治疗。通过对本组21例病变等级在Ⅳ级或Ⅳ级以上并进行CAG复查患儿的数据分析发现:若在规范的诊治及随访过程中出现新的症状,如胸痛、活动耐量明显下降、呼吸困难等,应进行及时造影复查;若心超或心电图提示有心肌缺血性改变(如室壁运动异常、局部室壁瘤形成),应该及时进行造影复查;由于常规的随访手段——心超对狭窄类的病变诊断并不敏感,因此若心超提示有冠脉内显示不清或新出现的冠脉内血栓,也应进行造影复查以明确诊断。
针对冠脉狭窄及闭塞的病变类型,在初次CAG时,21例患儿共发现13例冠脉狭窄及闭塞患儿,狭窄及闭塞多发于RCA与LAD;行CAG复查后有5例患儿冠脉狭窄出现进展并且有1例术中行球囊扩张,有1例术后行CABG术,并且侧支形成也均有不同程度的进展,表明川崎病所致严重冠脉病变可持续进展。2010年SAMADA等[7]对48例川崎病并发大型冠脉瘤患儿随访10~31年,发现34例(70.8%)并发冠状动脉狭窄和(或)闭塞。2011年SUDA等[8]随访了70例川崎病合并大型冠脉瘤的患儿,发现其30年的生存率为88%。而日本的一项包含245例川崎病患儿的多中心研究[9]发现,此类患儿30年的生存率为90%,但30年间无心脏事件生存率仅为36%,双侧冠脉受累的患儿更低,仅为21%。在长达30年的随访中,有69%的双侧冠脉受累患儿进行了CABG术,而单侧受累仅有20%行CABG术。中国台湾的一项大型冠脉瘤患儿的死亡率与无心脏事件生存率与日本相似[10]。本组21例患儿初次CAG后有6例行CABG术,并有1例行室壁瘤切除术;复查CAG后又有1例患儿行CABG术同时行室壁瘤切除术。本组数据与既往研究表明,川崎病所致严重冠脉病变即使死亡率不高,无心脏事件生存率也甚低,对于此类患儿需要定期随访,早期及时地临床干预。
将初次CAG与CAG术前的心超结果进行比对,以及Bland-Altman一致性分析后发现:在对冠脉瘤的数目、部位的诊断中,心脏超声与CAG有良好的相关性,心超在大型冠脉瘤患儿的随访过程中可为临床提供良好的诊断信息;但在冠脉瘤大小诊断方面存在一定的误差。对于冠脉狭窄的诊断,心超可能会出现误诊及漏诊。在本组病例初次CAG前,心超提示共有12处冠脉显示不清,后经CAG证实共有16处出现狭窄,1例出现冠脉血栓。因此,对于心超提示“病变冠脉显示不清”的描述,需要引起临床重视,可能会是狭窄或闭锁病变的表现。如表1中的病例2与病例4中,此2例患儿术前心超均提示相应冠脉瘤后的血管“显示不清或血栓形成”,后经CAG证实均为冠脉闭锁或狭窄伴侧支形成:1例患儿在长达3年的随访中,心超均提示患儿为LAD近段与RCA的2处冠脉瘤,但RCA中段显示不清,直到该患儿随访发现LVEF下降,后行CAG证实RCA主干扭曲变细,并且伴有侧支形成;另1例患儿在4年的随访过程中,心超仅提示患儿LAD与RCA近段的冠脉瘤样扩张,但LAD与RCA瘤后显示不清,后完善CAG检查,发现患儿RCA中段冠脉瘤后出现闭塞,而LAD近段发生冠脉狭窄。总体而言,心超作为川崎病最常用的复查手段,对冠脉狭窄的诊断,相较于心脏增强CT与CAG而言存在一定的局限[3],对于严重冠脉病变患儿需要进行CAG的检查,以明确复杂病变的诊断。
综上,川崎病导致的冠脉病变复杂,对于严重冠脉病变患儿,尤其是伴有冠脉狭窄的患儿,即使规范治疗和随访,其病变也可能不断进展;定期复查冠脉造影,有助于发现冠脉病变的进展,并及时处理,包括手术治疗或者药物治疗上的相应调整。
作者贡献声明
张锰、崔青参与研究方案的设计、论文的写作和修改,张锰、崔青、朱荻绮参与数据分析,张锰、崔青、朱荻绮、张玉奇、钟玉敏、沈捷参与数据采集、病例随访、研究实施。所有作者均阅读并同意了最终稿件的提交。
AUTHOR's CONTRIBUTIONS
The study was designed by ZHANG Meng and CUI Qing. The manuscript was drafted and revised by ZHANG Meng and CUI Qing. The data were analyzed by ZHANG Meng, CUI Qing and ZHU Diqi. Data collection, case follow-up and study implementation were completed by ZHANG Meng, CUI Qing, ZHU Diqi, ZHANG Yuqi, ZHONG Yumin and SHEN Jie. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
参考文献

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}