Preliminary study of pelvic floor structural changes in early and middle pregnant women with cervical incompetence
HE Ping,1, SHAO Feixue,2, GUO Lili,1, LI Keting1, MAO Xiaoyuan2, BAO Yirong2, WANG Lei3
1.Department of Ultrasound, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai 201204, China
2.Department of Obstetrics, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, Shanghai 201204, China
3.Department of Ultrasound, International Peace Maternal and Child Health Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200011, China
目的·通过超声检查探究有宫颈机能不全(cervical incompetence,CIC)史的孕妇早、中孕期盆底结构的变化特点。方法·收集2022年8月至2023年1月在同济大学附属第一妇婴保健院建卡的早、中孕期孕妇,所有孕妇均有且仅有1次早产,或者中孕流产、引产史,按照前次妊娠有无CIC病史将其分为CIC组和对照组。比较2组孕妇的年龄、体质量指数(BMI)、孕周、尿道内口漏斗形成率、尿失禁发生率。运用二维、三维及四维盆底超声对静息状态、盆底肌收缩(pelvic floor muscle contraction,PFMC)状态和瓦尔萨尔瓦动作(Valsalva maneuver,VM)状态下2组女性盆底结构进行测量;测量参数包括:膀胱颈位置、尿道倾斜角、尿道旋转角、膀胱后角、膀胱颈移动度、宫颈位置、直肠壶腹部位置、肛提肌裂孔面积(area of urogenital hiatus,HA)、肛提肌裂孔左右径、肛提肌裂孔前后径。采用一般线性回归模型校正混杂因素影响,分析CIC病史与盆底结构差异指标的相关性。结果·共纳入早、中孕期孕妇76例,其中CIC组39例,对照组37例。2组孕妇年龄差异无统计学意义,CIC组BMI、孕周均显著大于对照组,差异均有统计学意义(均P<0.05)。静息状态和PFMC状态下,2组孕妇盆底结构参数差异均无统计学意义(均P>0.05);VM状态下,CIC组HA(P=0.016)和肛提肌裂孔前后径(P=0.014)显著增大,其他指标差异无统计学意义。一般线性回归模型校正2组孕妇的孕周及BMI后发现,CIC病史与VM状态下HA(P=0.038)和肛提肌裂孔前后径(P=0.049)均存在相关性。CIC组和对照组尿道内口漏斗形成率分别为10.25%和0,压力性尿失禁发生率分别为23.07%和13.51%,差异均无统计学意义(均P>0.05)。结论·有CIC病史的孕妇VM状态下,HA和肛提肌裂孔前后径明显增大,肛提肌裂孔的形态改变以纵轴增加更为明显。
关键词:宫颈机能不全
;
超声检查
;
盆底
;
孕期
;
盆底功能障碍性疾病
Abstract
Objective ·To explore the changes of pelvic floor structure in the early and middle pregnant women with the history of cervical incompetence (CIC) by ultrasound. Methods ·The pregnant women during early and middle trimesters were collected from Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine from August 2022 to January 2023. All the pregnant women had only one history of premature delivery, abortion or induced labor in the middle trimester, and were divided into CIC group and control group according to whether having the history of CIC in the previous pregnancy. Age, body mass index (BMI), gestational age, the prevalence of funneling of internal urethral orifice and the prevalence of urinary incontinence were compared between the two groups. Two-dimensional, three-dimensional, and four-dimensional pelvic floor ultrasound was used to measure the pelvic floor structures of the women in the states of resting, pelvic floor muscle contraction (PFMC) and Valsalva maneuver (VM). The parameters of pelvic floor structure included bladder neck position, urethral inclination angle, urethral rotation angle, posterior angle of bladder, bladder neck mobility, cervix position, position of ampulla of rectum, area of urogenital hiatus (HA), hiatal transverse diameter, and hiatal anteroposterior diameter. General linear regression model was used to correct the influence of confounders and to analyze the association between the history of CIC and the different indexes of pelvic floor structure. Results ·A total of 76 pregnant women in early and middle trimesters were collected, including 39 women in the CIC group and 37 women in the control group. There was no significant difference in the age between the two groups, while BMI and gestational age in the CIC group were significantly greater than those of the control group, and the differences were significant (both P<0.05). At the states of resting and PFMC, there were no significant differences in structural parameters (all P> 0.05); at the state of VM, HA (P=0.016) and hiatal anteroposterior diameter (P=0.014) increased in the CIC group, while other parameters did not change significantly. It was found that the CIC history was associated with HA (P=0.038) and hiatal anteroposterior diameter (P=0.049) at VM after adjusting gestational age and BMI by the general linear regression model. The incidence rates of funneling of internal urethral orific in the CIC group and the control group were 10.25% and 0, respectively; the incidence rates of stress incontinence were 23.07% and 13.51%, respectively. Neither of the differences were significant (both P>0.05). Conclusion ·In the pregnant women with the history of CIC, HA and hiatal anteroposterior diameter at VM increase, and the morphological change of the levator ani hiatus is more obvious with the increase of the vertical axis.
HE Ping, SHAO Feixue, GUO Lili, LI Keting, MAO Xiaoyuan, BAO Yirong, WANG Lei. Preliminary study of pelvic floor structural changes in early and middle pregnant women with cervical incompetence. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(4): 459-465 doi:10.3969/j.issn.1674-8115.2023.04.008
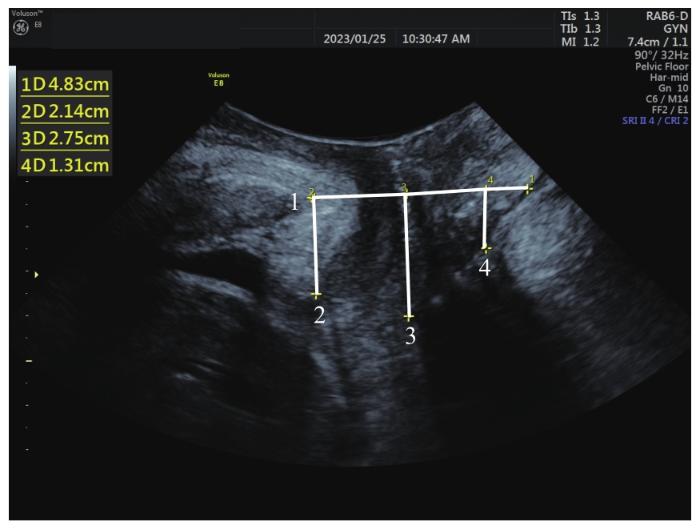
Note: 1—The reference line is a horizontal line placed at the inferoposterior margin of the symphysis pubis; 2—vertical distance of bladder neck; 3—vertical distance of cervix; 4—vertical distance of rectal ampulla position.
Fig 1
Measurements of bladder neck position, lowest edge of cervix and rectal ampulla position by pelvic floor ultrasound in pregnant women at rest
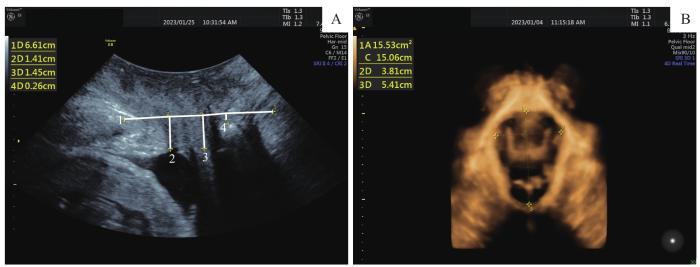
Note:A. Bladder neck position, lowest edge of cervix and rectal ampulla position observed by ultrasound at VM. 1—The reference line is a horizontal line placed at the inferoposterior margin of the symphysis pubis; 2—vertical distance of bladder neck; 3—vertical distance of cervix; 4—vertical distance of rectal ampulla position. B. HA measured by 4-dimensional ultrasound at VM.
Fig 2
Ultrasonic images and measurements of pelvic floor in pregnant women at VM
The study was designed by GUO Lili and SHAO Feixue. The manuscript was drafted and revised by HE Ping. Data collection and analysis were performed by LI Keting. Participant recruitment was performed by MAO Xiaoyuan, BAO Yirong and WANG Lei. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No.142: cerclage for the management of cervical insufficiency[J]. Obstet Gynecol, 2014, 123(2 Pt 1): 372-379.
DE VOS M, NUYTINCK L, VERELLEN C, et al. Preterm premature rupture of membranes in a patient with the hypermobility type of the Ehlers-Danlos syndrome. A case report[J]. Fetal Diagn Ther, 1999, 14(4): 244-247.
TOLA E N, KOROGLU N, YILDIRIM G Y, et al. The role of ADAMTS-2, collagen type-1, TIMP-3 and papilin levels of uterosacral and cardinal ligaments in the etiopathogenesis of pelvic organ prolapse among women without stress urinary incontinence[J]. Eur J Obstet Gynecol Reproductive Biol, 2018, 231: 158-163.
BEN-ZVI M, HERMAN H G, BAR J, et al. Are women with cervical incompetence at a higher risk of experiencing urinary and pelvic organ prolapse symptoms?[J]. Int Urogynecol J, 2020, 31(2): 385-389.
CHANG S R, LIN W A, LIN H H, et al. Cumulative incidence of urinary incontinence and associated factors during pregnancy and after childbirth: a cohort study[J]. Int Urogynecol J, 2022, 33(6): 1451-1461.
GRINBAUM M L, BIANCHI-FERRARO A M, RODRIGUES C A, et al. Impact of parity and delivery mode on pelvic floor function in young women: a 3D ultrasound evaluation[J]. Int Urogynecol J, 2023. DOI: 10.1007/s00192-022-05440-x.
DE ARAUJO C C, COELHO S A, STAHLSCHMIDT P, et al. Does vaginal delivery cause more damage to the pelvic floor than cesarean section as determined by 3D ultrasound evaluation? A systematic review[J]. Int Urogynecol J, 2018, 29(5): 639-645.
XU Z H, HE H L, YU B B, et al. Application of transperineal pelvic floor ultrasound in changes of pelvic floor structure and function between pregnant and non-pregnant women[J]. Int J Womens Health, 2022, 14: 1149-1159.
SHEK K L, KRUGER J, DIETZ H P. The effect of pregnancy on hiatal dimensions and urethral mobility: an observational study[J]. Int Urogynecol J, 2012, 23(11): 1561-1567.
CHAN S C, CHEUNG R K, YIU K W, et al. Pelvic floor biometry during a first singleton pregnancy and the relationship with symptoms of pelvic floor disorders: a prospective observational study[J]. BJOG, 2014, 121(1): 121-129.
CHAN S C, CHEUNG R K, YIU K W, et al. Pelvic floor biometry in Chinese primiparous women 1 year after delivery: a prospective observational study[J]. Ultrasound Obstet Gynecol, 2014, 43(4): 466-474.
CHAN S C, CHEUNG R K, LEE L L, et al. Longitudinal pelvic floor biometry: which factors affect it?[J]. Ultrasound Obstet Gynecol, 2018, 51(2): 246-252.
SHAO X H, KONG D J, ZHANG L W, et al. Ultrasound analysis of the effect of second delivery on pelvic floor function in Chinese women[J]. J Obstet Gynaecol, 2022, 42(2): 261-267.
JAMARD E, BLOUET M, THUBERT T, et al. Utility of 2D-ultrasound in pelvic floor muscle contraction and bladder neck mobility assessment in women with urinary incontinence[J]. J Gynecol Obstet Hum Reprod, 2020, 49(1): 101629.
VULIC M, STRINIC T, TOMIC S, et al. Difference in expression of collagen type I and matrix metalloproteinase-1 in uterosacral ligaments of women with and without pelvic organ prolapse[J]. Eur J Obstet Gynecol Reproductive Biol, 2011, 155(2): 225-228.
ALVES A P V D, FREITAS A B, LEVI J E, et al. COL1A1, COL4A3, TIMP2 and TGFB1 polymorphisms in cervical insufficiency[J]. J Perinat Med, 2021, 49(5): 553-558.
ALTMAN D, FORSMAN M, FALCONER CA, et al. Genetic influence on stress urinary incontinence and pelvic organ prolapse[J]. Eur Urol, 2008, 54(4): 918-923.
SHEYN D, ADDAE-KONAEDU K L, BAUER A M, et al. History of cervical insufficiency increases the risk of pelvic organ prolapse and stress urinary incontinence in parous women[J]. Maturitas, 2018, 107: 63-67.
BENDET A, LERON E, YARZA S, et al. Cervical insufficiency a prologue for future pelvic organ prolapse?[J]. Arch Gynecol Obstet, 2022, 306(4): 1053-1061.



{kind=link}
{kind=link}
{kind=link}
{kind=link}