Establishment of discriminative models for predicting the infiltration degree of patients with lung adenocarcinoma based on clinical laboratory indicators
WANG Mengfei,1,2,3, YANG Shouzhi4, QIAO Yongxia,1, HUANG Lin,2,3
1.School of Public Health, Shanghai Jiao Tong University, Shanghai 200025, China
2.Department of Clinical Laboratory Medicine, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200030, China
3.Shanghai Chest Cancer Research Institute, Shanghai Chest Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200030, China
4.School of Biomedical Engineering, Shanghai Jiao Tong University, Shanghai 200030, China
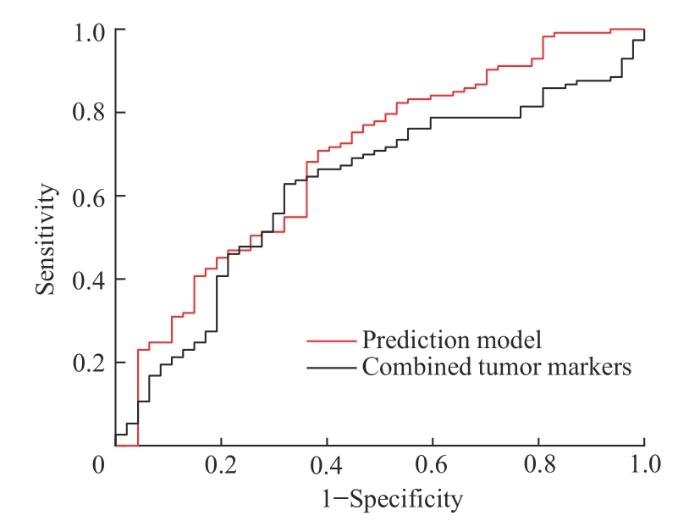
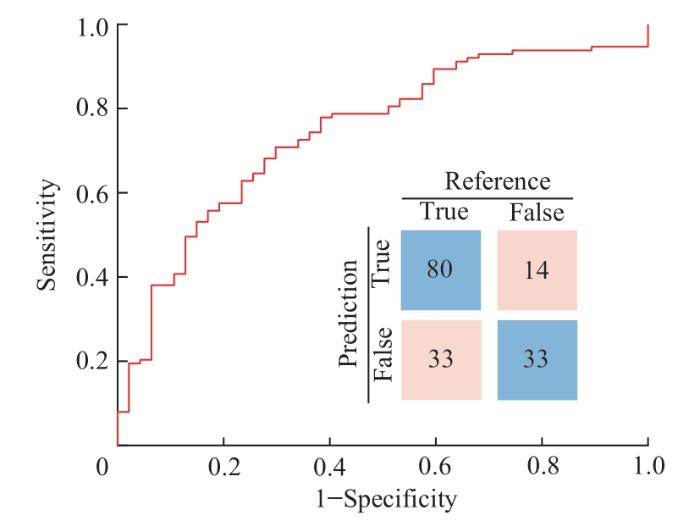
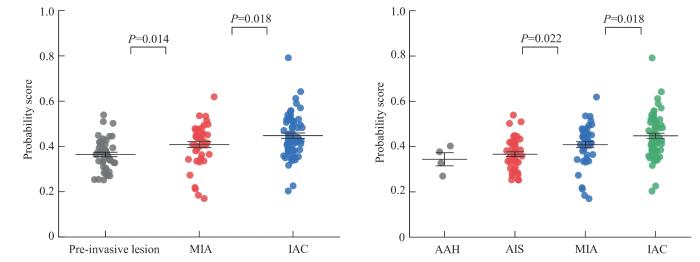
目的·利用肿瘤标志物、凝血功能指标、血常规指标与生化指标等临床易得检验指标,建立非小细胞肺腺癌患者浸润程度的多因素判别模型。方法·回顾性选取2022年上海交通大学医学院附属胸科医院收治的肺腺癌患者,通过多因素Logistic回归分析筛选预测肺腺癌患者浸润程度的独立影响因素并建立回归模型,同时引入人工智能算法构建判别模型,采用受试者工作特征曲线下面积(area under curve,AUC)评价模型对肺腺癌患者浸润程度的判别能力。结果·共纳入肺腺癌患者202例,分为浸润前病变组(59例)以及浸润性病变组(143例)。多因素Logistic回归分析结果显示,尿素、嗜碱性粒细胞百分比、白蛋白浓度是预测肺腺癌患者浸润程度的独立影响因素(均P<0.05)。预测模型表达式为P=e X /(1+e X ),其中X=(0.534×尿素浓度)+(1.527×嗜碱性粒细胞百分比)-(1.916×白蛋白浓度)+6.373。机器学习结果显示,纳入尿素、纤维蛋白原、白蛋白浓度、嗜碱性粒细胞百分比、前白蛋白、癌胚抗原(carcino embryonic antigen,CEA)6个指标时模型判别性能最佳。通过DeLong检验比较8种机器学习算法(分别基于岭回归、最小绝对收缩和选择算子、神经网络、随机森林、k近邻、支持向量机、决策树和自适应增强算法)的判别性能,选择AUC最高的岭回归算法,预测模型AUC为0.744(95%CI 0.656~0.832),敏感度为70.8%,特异度为70.2%。结论·使用尿素、纤维蛋白原、白蛋白浓度、嗜碱性粒细胞百分比、前白蛋白、CEA这6个指标建立综合判别模型,可有效预测肺腺癌患者肿瘤浸润程度,有望为临床肺腺癌分级判别和辅助治疗提供更精确的指导。
关键词:肺腺癌
;
肿瘤标志物
;
凝血功能指标
;
临床生化指标
;
预测判别模型
Abstract
Objective ·To establish a multifactorial discriminative model for predicting the degree of infiltration in patients with non-small cell lung adenocarcinoma based on clinically accessible laboratory indicators, such as tumor markers, coagulation function indicators, routine blood count indicators, and biochemical indicators. Methods ·A retrospective study was conducted on 202 patients with lung adenocarcinoma admitted to Shanghai Chest Hospital in 2022. Multifactorial Logistic regression analysis was applied to screen independent factors that influenced the predictive infiltration degree of lung adenocarcinoma and to establish a regression model. In addition, machine learning was used to construct a discriminative model, and the area under the receiver operating characteristic curve (AUC) was used to evaluate the discriminative ability of the model to discriminate the degree of infiltration in lung adenocarcinoma patients. Results ·A total of 202 patients with lung adenocarcinoma were included in the study, and divided into pre-invasive lesion group (n=59) and invasive lesion group (n=143). Multifactorial Logistic regression analysis revealed that urea, percentage of basophilic granulocytes, and albumin were independent factors for predicting the degree of infiltration of lung adenocarcinoma (all P<0.05). The predictive model expression was P = eX / (1 + eX ), where X = (0.534×urea) + (1.527×percentage of basophilic granulocytes) - (1.916×albumin) + 6.373. Machine learning results showed that the model performed best when urea, fibrinogen, albumin, percentage of basophilic granulocytes, prealbumin and carcino embryonic antigen (CEA) were included. After comparing the performance of 8 machine learning algorithms (based on ridge regression, least absolute shrinkage and selection operator, neural network, random forest, k-nearest neighbors, support vector machine, decision tree, and adaptive boosting algorithms) using the DeLong test, the ridge regression algorithm with the highest AUC was selected. The AUC of the predictive model was calculated to be 0.744 (95% CI 0.656-0.832), with a sensitivity of 70.8% and a specificity of 70.2%. Conclusion ·A comprehensive differentiation model constructed by urea, fibrinogen, albumin, percentage of basophilic granulocytes, prealbumin and CEA can effectively predict the infiltration degree of the enrolled lung adenocarcinoma patients, holding the potential to provide more precise guidance for the clinical grading and adjunctive treatment of lung adenocarcinoma.
Keywords:lung adenocarcinoma
;
tumor markers
;
coagulation function indicators
;
clinical biochemical indicators
;
predictive discriminative model
WANG Mengfei, YANG Shouzhi, QIAO Yongxia, HUANG Lin. Establishment of discriminative models for predicting the infiltration degree of patients with lung adenocarcinoma based on clinical laboratory indicators. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(1): 98-107 doi:10.3969/j.issn.1674-8115.2024.01.011
肺癌是全球范围内死亡率最高的癌症。据全球癌症统计数据[1]显示,2020年全世界新增肺癌患者达220万例。近年来,我国肺癌的发病率和死亡率也在逐年升高。预计到2025年,我国每年将有超过100万例的患者死于肺癌[2-3]。肺腺癌是肺癌中最常见的病理类型,占所有肺癌病例的40%~45%[4]。肺腺癌的发展可分为4个阶段,包括非典型腺瘤性增生(atypical adenomatous hyperplasia,AAH)、原位腺癌(adenocarcinoma in situ,AIS)、微浸润腺癌(minimally invasive adenocarcinoma,MIA)和浸润性腺癌(invasive adenocarcinoma,IAC)[5]。根据目前的诊疗共识[6],可进一步将肺腺癌分为浸润前病变(包括AAH和AIS)和浸润性病变(包括MIA和IAC)两大类。研究[6-7]表明,浸润前病变的肺腺癌患者一般采用楔形切除术或者解剖性肺段切除术,而浸润性病变的肺腺癌患者则多需要采用肺叶切除术和淋巴结清扫。进行肺叶切除术往往会增加患者术后引流管的留置时间,导致患者经济负担加重[8]。若术前可根据肺腺癌患者浸润程度确定手术方式,将进一步缩短手术时间,降低患者住院费用,进而加快医院病床利用率,实现医疗资源的合理配置。因此,术前判断肺腺癌患者浸润程度对降低肺腺癌相关死亡率和辅助临床决策具有重要意义。
透景Tesmi F4000全自动流式荧光发光免疫分析仪及配套原装试剂盒(上海透景生命科技股份有限公司),希森美康CA7000全自动凝血分析仪及其配套定标品、质控品(希森美康,日本),迈瑞BC-6800Plus全自动血液细胞分析仪及配套原装试剂盒(深圳迈瑞生物医疗电子股份有限公司),贝克曼库尔特AU5800全自动生化分析仪及配套原装试剂盒(贝克曼库尔特,美国),罗氏cobas u 601尿液分析仪及其配套原装试剂盒(罗氏,美国),爱威AVE-562全自动粪便分析仪及其配套原装试剂盒(爱威科技股份有限公司)。
Tab 3 Multivariate Logistic regression analysis of test indicators and clinical data predicting infiltration degree in patients with lung adenocarcinoma
WANG Mengfei contributed to the manuscript writing, data collection, data analysis, and figure preparation of this study. YANG Shouzhi participated in the data collection and data analysis of this study. QIAO Yongxia participated in the data collection and manuscript revision of this study. HUANG Lin contributed to the conceptualization and manuscript revision of this study.
SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249.
Editorial Board of Chinese Journal of Clinical Oncology and Rehabilitation. The latest cancer data in China in 2017[J]. Chinese Journal of Clinical Oncology and Rehabilitation, 2017, 24(6): 760.
LI X, GAO S. Trend analysis of the incidence, morbidity and mortality of lung cancer in China from 1990 to 2019[J]. Chinese Journal of Prevention and Control of Chronic Diseases, 2021, 29(11): 821-826.
LI M Y, LIU L Z, DONG M. Progress on pivotal role and application of exosome in lung cancer carcinogenesis, diagnosis, therapy and prognosis[J]. Mol Cancer, 2021, 20(1): 22.
SUCCONY L, RASSL D M, BARKER A P, et al. Adenocarcinoma spectrum lesions of the lung: detection, pathology and treatment strategies[J]. Cancer Treat Rev, 2021, 99: 102237.
JIANG G N, CHEN C, ZHU Y M, et al. Shanghai pulmonary hospital experts consensus on the management of groundglass nodules suspected as lung adenocarcinoma (version 1)[J]. Chinese Journal of Lung Cancer, 2018, 21(3): 147-159.
CHEN S Y, YU Z T, LIN J X, et al. The impact of early invasive lung adenocarcinoma on the economic cost of hospitalization in patients choosing minimally invasive surgery[J]. Modern Hospitals, 2023, 23(4): 607-609, 618.
LIANG X, SONG Y Y, GAO T, et al. An analysis of influence of severe perioperative complications and preoperative basic diseases on the hospitalization expenses of surgical lung cancer patients[J]. Chinese Hospitals, 2021, 25(4): 58-61.
LORTET-TIEULENT J, SOERJOMATARAM I, FERLAY J, et al. International trends in lung cancer incidence by histological subtype: adenocarcinoma stabilizing in men but still increasing in women[J]. Lung Cancer, 2014, 84(1): 13-22.
PAN J F, KUANG P D, YING M L, et al. Differential diagnosis of pulmonary invasive adenocarcinoma and preinvasive lesions in pure ground-glass nodules on high resolution targeted CT scan[J]. Zhejiang Medical Journal, 2016, 38(11): 826-828, 832.
BA W J, XU D, YIN K, et al. Application value of pulmonary nodule roundness on HRCT in predicting invasiveness of pure ground glass nodules and its correlation with long-short diameter ratio and depth of lobulation[J]. Radiologic Practice, 2020, 35(12): 1542-1546.
WU Q Y, BIAN G Y, CHENG H J, et al. Analysis on prognostic factors of lung adenocarcinoma and diagnostic efficacy of serum tumor markers[J]. Journal of Kunming Medical University, 2020, 41(9): 32-37.
ZHU T Y, BAO Y Y. Expression levels and significance of CEA, CA125, SCC, and fibrinogen in lung cancer patients[J]. Guide of China Medicine, 2019, 17(6): 141-142.
XU H P, XUE B, XU D. Application of combined detection of tumor markers CEA, NSE, and CYFRA21-1 in the diagnosis of lung cancer[J]. The Journal of Practical Medicine, 2010, 26(16): 2943-2944.
DU J H, QIAO H Y, YIN Y F. Prognostic value of serum CEA, CA125 and Cyfra21-1 inpatients with advanced nonsmall cell lung cancer[J]. Cancer Research on Prevention and Treatment, 2016, 43(2): 137-140.
ZHANG T S, REN H F, CAO J, et al. A diagnostic model combined with multiple laboratory indexes for ovarian cancer based on integrated machine learning[J]. Chinese Journal of Clinical Laboratory Science, 2018, 36(12): 908-913.
ZHANG W W, ZOU H, YANG R, et al. Predictive value of routine clinical test indicators in the diagnosis of colorectal cancer (CRC) and their correlation with clinicopathological parameters of CRC[J]. Chinese Journal of Clinical Laboratory Science, 2021, 39(3): 172-177.
WANG H, WU Y G, GUO Y T, et al. Construction of risk prediction model for preeclampsia based on routine clinical examination indicators[J]. Chinese Journal of Clinical Laboratory Science, 2022, 40(10): 731-736.
WINTER M C, POTTER V A, WOLL P J. Raised serum urea predicts for early death in small cell lung cancer[J]. Clin Oncol (R Coll Radiol), 2008, 20(10): 745-750.
ZUO Z H, YAN X, CAI S H. Analysis of the diagnostic value of carcinoembryonic antigen in lung adenocarcinoma[J]. People′s Military Surgeon, 2015, 58(5): 553-554.
QU T, ZHANG J W, XU N, et al. Diagnostic value analysis of combined detection of Trx, CYFRA21-1 and SCCA in lung cancer[J]. Oncol Lett, 2019, 17(5): 4293-4298.
LIU L, ZHANG W, LIU B, et al. Clinical significance of Scc and CYFRA21-1 (serum tumor markers) in diagnosis of lung squamous cell carcinoma[J]. Progress in Modern Biomedicine, 2010, 10(20): 3862-3865.
PENG Y, WANG Y, LI J L, et al. Utility of NSE, ProGRP and LDH in diagnosis and treatment in patients with small cell lung cancer[J]. Chinese Journal of Lung Cancer, 2016, 19(9): 590-594.
FU X H, CHEN B J, MA P, et al. The value of combined detection of serum tumor markers in the diagnosis of lung cancer[J]. Guangdong Medical Journal, 2013, 34(3): 401-404.
LIU L J, TENG J L, ZHANG L J, et al. The combination of the tumor markers suggests the histological diagnosis of lung cancer[J]. Biomed Res Int, 2017, 2017: 2013989.
ZHONG M H, ZHANG Y, PAN Z G, et al. Clinical utility of circulating tumor cells in the early detection of lung cancer in patients with a solitary pulmonary nodule[J]. Technol Cancer Res Treat, 2021, 20: 15330338211041465.
ZHANG J, NIE X H, HE H F. Correlation study of plasma D-dimer, fibrinogen, carcinoembryonic antigen, and cytokeratin 19 fragment in non-small cell lung cancer patients[J]. West China Medical Journal, 2022, 37(2): 218-223.
YI W W, QIAO T T, YANG Z Y, et al. The regulation role and diagnostic value of fibrinogen-like protein 1 revealed by pan-cancer analysis[J]. Mater Today Bio, 2022, 17: 100470.
TANG X Y, XIONG Y L, SHI A P, et al. The downregulation of fibrinogen-like protein 1 inhibits the proliferation of lung adenocarcinoma via regulating MYC-target genes[J]. Transl Lung Cancer Res, 2022, 11(3): 404-419.
LI Y L, LI L, ZHANG L, et al. Relationships between serum albumin and urea level andthe clinical pathological characteristics and survival time in patients with lung cancer[J]. Chinese Journal of Lung Cancer, 2017, 20(3): 175-186.
KUIKEL S, PATHAK N, POUDEL S, et al. Neutrophil-lymphocyte ratio as a predictor of adverse outcome in patients with community-acquired pneumonia: a systematic review[J]. Health Sci Rep, 2022, 5(3): e630.
LIU C, ZHAO X Z, BAI Y Q, et al. Correlation of clinical parameters with serum markers in patients with lung adenocarcinoma[J]. Journal of Tongji University (Medical Science) , 2019, 40(1): 87-90, 97.
WENG S H, SUN Y F, XU X, et al. 18F-FDG PET combined with serum tumor markers in the staging of lung adenocarcinoma[J]. Journal of Clinical Radiology, 2020, 39(4): 800-804.
HUANG G, JIANG B B, XIE X Q, et al. Establishment of a diagnostic model for lung adenocarcinoma with invasive tendency by CT and laboratory indexes[J]. Computerized Tomography Theory and Applications, 2021, 30(1): 81-90.
REN X L, ZHANG Y X, LYU Y, et al. Lactate dehydrogenase and serum tumor markers for predicting metastatic status in geriatric patients with lung adenocarcinoma[J]. Cancer Biomark, 2019, 26(2): 139-150.
ZHENG H, LI J Y, WANG S, et al. Evaluation on the invasion of lung cancer by diagnostic model nomogram based on the CT characteristics of pulmonary ground glass nodules[J]. Radiologic Practice, 2021, 36(4): 470-474.
ZHANG T Q, LI X L, LIU J H. Prediction of the invasiveness of ground-glass nodules in lung adenocarcinoma by radiomics analysis using high-resolution computed tomography imaging[J]. Cancer Control, 2022, 29: 10732748221089408.
YANG S C, LAI W W, SU W C, et al. Estimating the lifelong health impact and financial burdens of different types of lung cancer[J]. BMC Cancer, 2013, 13: 579.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}