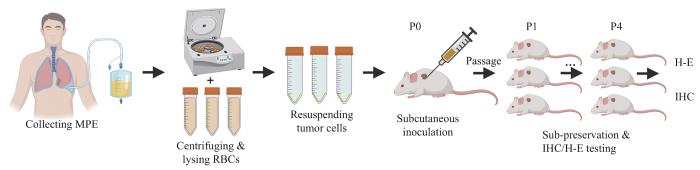
Objective ·To establish a patient-derived tumor xenograft (PDX) model using tumor cells sourced from malignant pleural effusion (MPE) in patients with lung cancer, and to conduct experimental validation. Methods ·Gene expression data were downloaded from the Gene Expression Omnibus (GEO), including single-cell RNA sequencing data for lung cancer with MPE (GSE131907) and for solid lung cancer (GSE203360). Data were clustered, and differential gene ontology functional enrichment analysis was performed to ascertain the feasibility of modeling by using MPE. MPE samples from patients with lung cancer were collected and processed through centrifugation and red blood cell lysis to enrich cells. The enriched cells were then implanted subcutaneously into non-obese diabetic/severe combined immunodeficient (NOD/SCID) mice. Tumor growth was monitored, and when tumors reached 1 000 mm³, they were passaged and preserved. Histopathological examination was conducted on stable passaged tumors, the cell morphology was observed via hematoxylin-eosin (H-E) staining and the expression of lung cancer biomarkers was detected by using immunohistochemistry (IHC). Results ·Single-cell data analysis revealed stronger proliferative functions of tumor cells in MPE, suggesting that PDX modeling using MPE tumor cells may yield better tumor formation. A total of 35 samples of MPE from lung cancer patients were collected, and 13 PDX models were successfully constructed, with a success rate of 37.14%. Histopathological examination showed significant cellular atypia by H-E staining, and IHC result showed positive expression of lung cancer biomarkers such as cytokeratin 7 (CK7), thyroid transcription factor-1 (TTF1), and Napsin A. Conclusion ·By enriching tumor cells from MPE of lung cancer patients, a more convenient, efficient, and dynamically modelable PDX model is successfully constructed. This model retains the malignant characteristics and protein expression features of tumor cells from lung cancer patients, providing an important experimental model tool for basic research and clinical drug guidance for lung cancer patients with MPE.
WANG Mengting, CHEN Yinan, XUANYUAN Xinyang, YUAN Haihua. Construction and experimental validation of mouse PDX model by malignant pleural effusion-derived tumor cells from lung cancer. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(4): 435-443 doi:10.3969/j.issn.1674-8115.2024.04.003
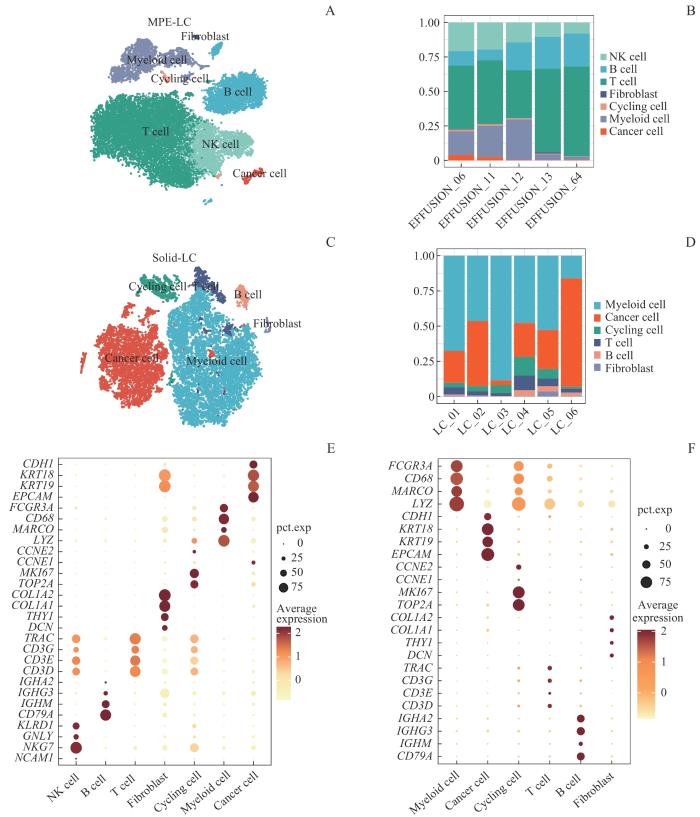
Note: A. Clustering and dimension reduction identified 7 cell subtypes in 5 malignant pleural effusion lung cancer (MPE-LC) samples. B. Stacked percentage bar charts for MPE-LC show the cell proportions in each subtype. C. Clustering and dimension reduction revealed 6 cell subtypes in 6 solid lung cancer (Solid-LC) samples. D. Stacked percentage bar charts for Solid-LC illustrate the cell proportions in each subtype. E. Bubble plots for MPE-LC display the expression of classic marker genes within each cell subtype. F. Bubble plots for Solid-LC depict the expression of classic marker genes within each cell subtype. KLRD1—killer cell lectin-like receptor D1; GNLY—granulysin; NKG7—natural killer cell granule protein 7; NCAM1—neural cell adhesion molecule 1; IGHA2—immunoglobulin heavy constant α2; IGHG3—immunoglobulin heavy constant γ3; IGHM—immunoglobulin heavy constant mu; CD79A—CD79a molecule; TRAC—T cell receptor α constant; CD3G—CD3 γ subunit of T-cell receptor complex; CD3E—CD3 ε subunit of T-cell receptor complex; CD3D—CD3 δ subunit of T-cell receptor complex; COL1A2—collagen type Ⅰ α 2 chain; THY1—thy-1 cell surface antigen; DCN—decorin; CCNE2—cyclin E2; MKI67—marker of proliferation Ki-67; TOP2A—DNA topoisomerase Ⅱ α; FCGR3A—Fc γ receptor Ⅲa; MARCO—macrophage receptor with collagenous structure; LYZ—lysozyme; CDH1—cadherin 1; KRT18—keratin 18; EPCAM—epithelial cell adhesion molecule.
Fig 2
Heterogeneity of cell subpopulations in MPE and solid tumor of lung cancer
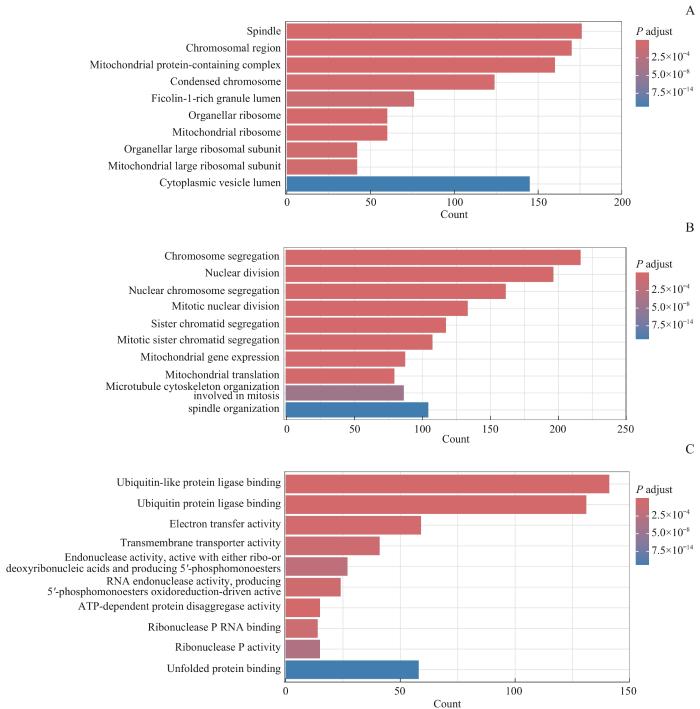
Note: A. Cellular component (CC) terms of GO enrichment analysis. B. Biological process (BP) terms of GO enrichment analysis. C. Molecular function (MF) terms of GO enrichment analysis.
Fig 3
Differential expression GO enrichment analysis of tumor cell subsets of MPE and solid tumors in lung cancer
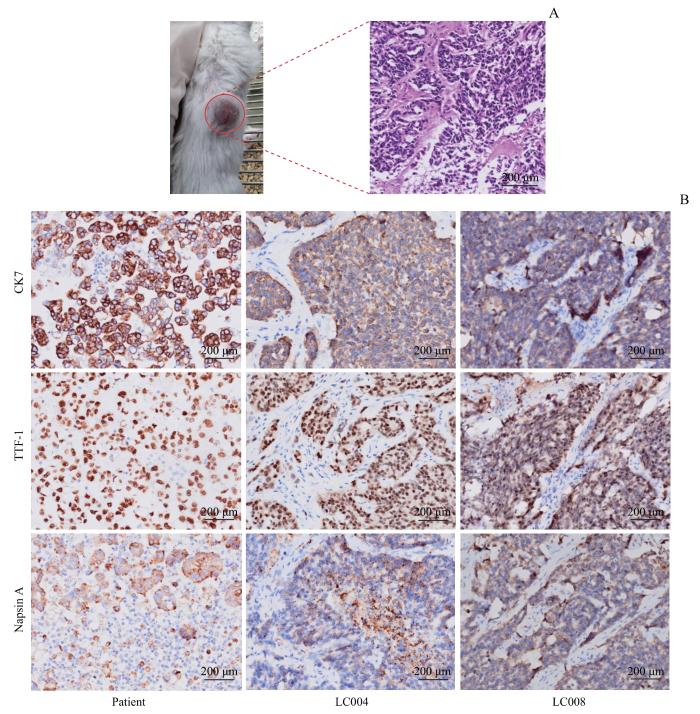
Note: A. The growth of subcutaneous MPE-PDX in NOD/SCID mice (left); P4 generation PDX with H-E staining (×200) (right). B. IHC testing (×200) of transplanted tumors compared with clinical samples of MPE tumor cells from patients.
Fig 4
Histopathological validation on mouse PDX of tumor cells derived from MPE of lung cancer
然而,本研究也存在一定的局限性。首先,我们并未使用短串联重复序列(short tandem repeat,STR)技术对患者肿瘤组织与MPE建模移植瘤进行比对,以加强验证PDX保留患者肿瘤异质性的可信性。在后续实验中,我们将同时应用H-E染色、IHC以及STR技术作为与患者比对的硬性指标。其次,本研究仅收集了35例MPE样本,样本量相对较少。为获得更为可信的成瘤率数据,我们将在后续的研究中持续进行样本收集,扩大样本规模,提高研究的统计效能,以助于更全面地评估MPE来源PDX模型的建模效果,并为未来的研究提供更可靠的数据支持。
WANG Mengting, CHEN Yinan, XUANYUAN Xinyang and YUAN Haihua participated in the design of the entire research project. WANG Mengting contributed to the completion of bioinformatics analysis, modeling, experimental validation of the model, and writing of the manuscript. CHEN Yinan and XUANYUAN Xinyang were involved in bioinformatics analysis and manuscript writing. All authors have read the final manuscript and approved the submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
PORCEL J M, GASOL A, BIELSA S, et al. Clinical features and survival of lung cancer patients with pleural effusions[J]. Respirology, 2015, 20(4): 654-659.
SHIBAKI R, MURAKAMI S, SHINNO Y, et al. Malignant pleural effusion as a predictor of the efficacy of anti-PD-1 antibody in patients with non-small cell lung cancer[J]. Thorac Cancer, 2019, 10(4): 815-822.
SATOH K, MORISAWA S, OKUYAMA M, et al. Severe pleural effusion associated with nilotinib for chronic myeloid leukaemia: cross-intolerance with tyrosine kinase inhibitors[J]. BMJ Case Rep, 2021, 14(9): e243671.
WANG T F, CHU S C, LEE J J, et al. Presence of pleural effusion is associated with a poor prognosis in patients with epidermal growth factor receptor-mutated lung cancer receiving tyrosine kinase inhibitors as first-line treatment[J]. Asia Pac J Clin Oncol, 2017, 13(4): 304-313.
JIN K T, TENG L S, SHEN Y P, et al. Patient-derived human tumour tissue xenografts in immunodeficient mice: a systematic review[J]. Clin Transl Oncol, 2010, 12(7): 473-480.
ROSCILLI G, de VITIS C, FERRARA F F, et al. Human lung adenocarcinoma cell cultures derived from malignant pleural effusions as model system to predict patients chemosensitivity[J]. J Transl Med, 2016, 14: 61.
SUN S Q, ZHU J Q, MA Y, et al. Accuracy, robustness and scalability of dimensionality reduction methods for single-cell RNA-seq analysis[J]. Genome Biol, 2019, 20(1): 269.
ASHBURNER M, BALL C A, BLAKE J A, et al. Gene ontology: tool for the unification of biology. The Gene Ontology Consortium[J]. Nat Genet, 2000, 25(1): 25-29.
WAKEFIELD C E, DOOLAN E L, FARDELL J E, et al. The avatar acceptability study: survivor, parent and community willingness to use patient-derived xenografts to personalize cancer care[J]. EBioMedicine, 2018, 37: 205-213.
HEINRICH M A, MOSTAFA A M R H, MORTON J P, et al. Translating complexity and heterogeneity of pancreatic tumor: 3D in vitro to in vivo models[J]. Adv Drug Deliv Rev, 2021, 174: 265-293.
MAKIMOTO G, OHASHI K, TOMIDA S, et al. Rapid acquisition of alectinib resistance in ALK-positive lung cancer with high tumor mutation burden[J]. J Thorac Oncol, 2019, 14(11): 2009-2018.
PARK B, JEONG B C, CHOI Y L, et al. Development and characterization of a bladder cancer xenograft model using patient-derived tumor tissue[J]. Cancer Sci, 2013, 104(5): 631-638.
STOCKHAMMER P, HO C S L, HEGEDUS L, et al. HDAC inhibition synergizes with ALK inhibitors to overcome resistance in a novel ALK mutated lung adenocarcinoma model[J]. Lung Cancer, 2020, 144: 20-29.
YANG X L. Establishment and identification of malignant pleural effusion-derived lung cancer primary cell culture and its chemosensitivity[D]. Zhengzhou: Zhengzhou University, 2017.
RUAN H Y, WANG Z, SUN Z W, et al. Single-cell RNA sequencing reveals the characteristics of cerebrospinal fluid tumour environment in breast cancer and lung cancer leptomeningeal metastases[J]. Clin Transl Med, 2022, 12(6): e885.
KIM N, KIM H K, LEE K, et al. Single-cell RNA sequencing demonstrates the molecular and cellular reprogramming of metastatic lung adenocarcinoma[J]. Nat Commun, 2020, 11(1): 2285.
KAO T W, BAI G H, WANG T L, et al. Novel cancer treatment paradigm targeting hypoxia-induced factor in conjunction with current therapies to overcome resistance[J]. J Exp Clin Cancer Res, 2023, 42(1): 171.
KANG H N, CHOI J W, SHIM H S, et al. Establishment of a platform of non-small-cell lung cancer patient-derived xenografts with clinical and genomic annotation[J]. Lung Cancer, 2018, 124: 168-178.
CHEN X M, SHEN C, WEI Z, et al. Patient-derived non-small cell lung cancer xenograft mirrors complex tumor heterogeneity[J]. Cancer Biol Med, 2021, 18(1): 184-198.
CHEN Y, ZHANG R, WANG L, et al. Tumor characteristics associated with engraftment of patient-derived non-small cell lung cancer xenografts in immunocompromised mice[J]. Cancer, 2019, 125(21): 3738-3748.
WANG D, PHAM N A, TONG J F, et al. Molecular heterogeneity of non-small cell lung carcinoma patient-derived xenografts closely reflect their primary tumors[J]. Int J Cancer, 2017, 140(3): 662-673.
KITA K, FUKUDA K, TAKAHASHI H, et al. Patient-derived xenograft models of non-small cell lung cancer for evaluating targeted drug sensitivity and resistance[J]. Cancer Sci, 2019, 110(10): 3215-3224.
STEWART E L, MASCAUX C, PHAM N A, et al. Clinical utility of patient-derived xenografts to determine biomarkers of prognosis and map resistance pathways in EGFR-mutant lung adenocarcinoma[J]. J Clin Oncol, 2015, 33(22): 2472-2480.
FICHTNER I, ROLFF J, SOONG R, et al. Establishment of patient-derived non-small cell lung cancer xenografts as models for the identification of predictive biomarkers[J]. Clin Cancer Res, 2008, 14(20): 6456-6468.
ZHANG X C, ZHANG J C, LI M, et al. Establishment of patient-derived non-small cell lung cancer xenograft models with genetic aberrations within EGFR, KRAS and FGFR1: useful tools for preclinical studies of targeted therapies[J]. J Transl Med, 2013, 11: 168.
LIAO H, ZHOU S X, CHEN S, et al. Establishment and characterization of patient-derived xenograft model of non-small-cell lung cancer derived from malignant pleural effusions[J]. Cancer Manag Res, 2023, 15: 165-174.
XIN Y Q, LI S Y, JIANG Q K, et al. Establishment of a jaw fibrosarcoma patient-derived xenograft and evaluation of the tumor suppression efficacy of plumbagin against jaw fibrosarcoma[J]. Front Oncol, 2020, 10: 1479.
HUANG T L, CHEN B Y, WANG F, et al. Rab1A promotes IL-4R/JAK1/STAT6-dependent metastasis and determines JAK1 inhibitor sensitivity in non-small cell lung cancer[J]. Cancer Lett, 2021, 523: 182-194.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}