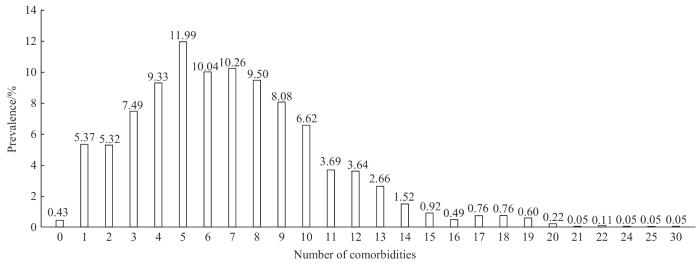
Objective ·To investigate the current situation and distribution characteristics of chronic comorbidities, and to provide reference for further improving the self-management of comorbidities and implementing the whole course and all-round management of comorbidity. Methods ·Two thousand and forty-five inpatients in the Department of Geriatrics,Renji Hospital, Shanghai Jiao Tong University School of Medicine were enrolled in this study from December 2020 to February 2023. The general vital signs, routine laboratory examination and disease status were collected. The epidemiological distribution characteristics of chronic diseases and comorbidities were analyzed. Results ·The incidence of chronic diseases in the surveyed population was 99.6%, and the incidence of comorbidities was 94.2%. The top 5 chronic diseases were hypertension (43.68%), diabetes mellitus (24.81%), malignant tumor (21.48%), hyperlipidemia (18.38%) and coronary heart disease (11.99%). The detection rates of hypertension, diabetes mellitus, coronary heart disease, chronic obstructive pulmonary disease, stoke and chronic kidney disease in males were significantly higher than those in females (P<0.05). The proportion of patients with 5 chronic diseases was the highest (11.99%), followed by 7 chronic diseases (10.26%) and 6 chronic diseases (10.04%). Among the patients of different ages, the comorbidity rate was the highest in the patients aged 50‒59 years (27.78%). In different age groups, patients aged 50 to 59 with 2 chronic diseases had the highest incidence of comorbidity, which was as high as 40.82%. Although the overall proportion of comorbidities among male patients (95.37%) was higher than that among females (93.77%), there was no statistically significant difference (P=0.125). However, the proportions of male patients with 2 and 5 chronic diseases were 70.41% and 60.63%, respectively, which were significantly higher than those of female patients (29.59% and 39.37%). The correlations between coronary heart disease and diabetes mellitus, hypertension and coronary heart disease, hypertension and diabetes mellitus were higher (r=0.24, r=0.27, r=0.35, all P<0.05). Conclusion ·The prevalence of chronic diseases and comorbidities is high in the middle-aged and elderly population, and the number of comorbidities increases significantly with the increase of age.
HAO Mingxiu, CHEN Hongwei, WANG Junlin, TANG Yinhan, WU Yunyun, JIN Yuhua, HU Yaomin. Investigation and epidemiological analysis of chronic diseases and comorbidities in hospitalized patients. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(4): 462-468 doi:10.3969/j.issn.1674-8115.2024.04.006
HAO Mingxiu was responsible for manuscript writing. CHEN Hongwei was responsible for data organization. WANG Junlin, TANG Yinhan, WU Yunyun and JIN Yuhua were responsible for data collection. HU Yaomin was responsible for conception. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
CAO F, WANG Y B, XUE W G, et al. Clinical multi-centers report of chronic diseases among elderly inpatients in China[J]. Chinese Journal of Multiple Organ Diseases in the Elderly, 2018, 17(11): 801-808.
Writing Group of 2018 Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, Chinese Medical Doctor Association Hypertension Committee, Hypertension Branch of China International Exchange and Promotive Association for Medical and Health Care, et al. 2018 Chinese guidelines for the management of hypertension[J].Chinese Journal of Cardiovascular Medicine, 2019, 24(1): 24-56.
Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition)[J]. Chinese Journal of Diabetes, 2021, 13(4): 315-409.
Joint Committee Issued Chinese Guideline for the Management of Dyslipidemia. 2016 Chinese guideline for the management of dyslipidemia in adults[J]. Chinese Journal of Cardiovascular Disease, 2016, 44(10): 833-853.
WILLADSEN T G, SIERSMA V, NICOLAISDÓTTIR D R, et al. Multimorbidity and mortality: a 15-year longitudinal registry-based nationwide Danish population study[J]. J Comorb, 2018, 8(1): 2235042X18804063.
MENOTTI A, MULDER I, NISSINEN A, et al. Prevalence of morbidity and multimorbidity in elderly male populations and their impact on 10-year all-cause mortality: the FINE study (Finland, Italy, Netherlands, Elderly)[J]. J Clin Epidemiol, 2001, 54(7): 680-686.
VOGELI C, SHIELDS A E, LEE T A, et al. Multiple chronic conditions: prevalence, health consequences, and implications for quality, care management, and costs[J]. J Gen Intern Med, 2007, 22(Suppl 3): 391-395.
ARAMRAT C, CHOKSOMNGAM Y, JIRAPORNCHAROEN W, et al. Advancing multimorbidity management in primary care: a narrative review[J]. Prim Health Care Res Dev, 2022, 23: e36.
MCPARLAND C, COOPER M A, LOWE D J, et al. Multimorbidity, disease count, mortality and emergency care use in persons attending the emergency department: a cross-sectional data-linkage study[J]. J Multimorb Comorb, 2022, 12: 26335565221147417.
GARIN N, OLAYA B, PERALES J, et al. Multimorbidity patterns in a national representative sample of the Spanish adult population[J]. PLoS One, 2014, 9(1): e84794.
KIRCHBERGER I, MEISINGER C, HEIER M, et al. Patterns of multimorbidity in the aged population. Results from the KORA-Age study[J]. PLoS One, 2012, 7(1): e30556.
SINHA A, KERKETTA S, GHOSAL S, et al. Multimorbidity and complex multimorbidity in India: findings from the 2017-2018 longitudinal ageing study in India (LASI)[J]. Int J Environ Res Public Health, 2022, 19(15): 9091.
VAN DEN AKKER M, BUNTINX F, METSEMAKERS J F, et al. Multimorbidity in general practice: prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases[J]. J Clin Epidemiol, 1998, 51(5): 367-375.
Endocrinology and Metabolism Branch of Chinese Association of Geriatric Research, Committee of Clinical Toxicology of Chinese Society of Toxicology. Expert consensus on risk management of polypharmacy in elderly[J]. Chinese General Practice, 2018, 21(29): 3533-3544.
ZHANG X H, GU Y M, WANG Z Y, et al.Status investigation of chronic comorbidity status in elderly at tertiary hospitals and community hospitals[J]. Clinical Focus, 2021, 36(1): 39-43.
CHANG J, HOU Y P, WU J L, et al. Multi-morbidity patterns in Chinese elderly patients: an analysis of 5 505 in-hospital cases[J]. Chinese Journal of Multiple Organ Diseases in the Elderly, 2014,13(4): 251-254.
MA K, FENG M, ZHAO R M, et al. Prevalence of comorbidity in inpatientes of department of general practice[J]. Chinese General Practice, 2017, 20(23): 2820-2822.
ZHAO Y, ATUN R, OLDENBURG B, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data[J]. Lancet Glob Health, 2020, 8(6): e840-e849.
WANG H H, WANG J J, WONG S Y, et al. Epidemiology of multimorbidity in China and implications for the healthcare system: cross-sectional survey among 162 464 community household residents in Southern China[J]. BMC Med, 2014, 12: 188.
RONG P, CHEN Y, DANG Y, et al. Geographical specific association between lifestyles and multimorbidity among adults in China[J]. PLoS One, 2023, 18(6): e0286401.
DENG X, DONG P, ZHANG L, et al. Health-related quality of life in residents aged 18 years and older with and without disease: findings from the First Provincial Health Services Survey of Hunan, China[J]. BMJ Open, 2017, 7(9): e015880.
GU J, CHAO J, CHEN W, et al. Multimorbidity and health-related quality of life among the community-dwelling elderly: a longitudinal study[J]. Arch Gerontol Geriatr, 2018, 74: 133-140.



{kind=link}
{kind=link}