Dentofacial phenotype of non-syndromic tooth agenesis patients with PAX9 mutation
DOU Jiaqi,, GAO Jie, BIAN Xiaoling, WANG Feng, DAI Qinggang,, WU Yiqun,
Department of 2nd Dental Center, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine; College of Stomatology, Shanghai Jiao Tong University; National Center for Stomatology; National Clinical Research Center for Oral Diseases; Shanghai Key Laboratory of Stomatology; Shanghai Research Institute of Stomatology, Shanghai 201999, China
Objective ·To evaluate the dentofacial phenotype in non-syndromic tooth agenesis (NSTA) patients with paired box gene 9 (PAX9) mutation. Methods ·Patients with NSTA who visited the Department of Second Dental Center of Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, between January 2016 and December 2023 received whole-exome sequencing to screen PAX9 mutation. The location and number of missing teeth were evaluated by oral pantomography, and dentofacial deformities were evaluated by X-ray cephalometrics. Results ·Seven patients with PAX9 mutation were included in the study, including 3 males (42.9%) and 4 females (57.1%). The patients were 7‒31 years old at first visit, with a mean age of (19.7±8.0) years old. All the 7 patients were PAX9 heterozygotes, of which 4 were missense and 3 were frameshift. The average number of missing teeth was 15.9±2.9. The number of missing teeth in maxilla (9.6±2.6) was slightly higher than that in mandible (6.3±2.4) (P=0.030). Maxillary second molar (100.0%), maxillary canine (85.7%) and mandibular second premolar (85.7%) were the three most common missing teeth, while mandibular lateral incisor (14.3%) and mandibular canine (14.3%) were the two least missing teeth. Patients with frameshift mutation had more missing teeth (18.3±2.1) than those with missense mutation (14.0±1.8) (P=0.032). X-ray cephalometrics analysis results showed that the angle sella-nasion-subspinale (SNA), angle nasion-subspinale-subspinale-porion (NA-Apo) and sella-nasion (S-N) in adult patients with PAX9 mutation were significantly lower than the normal reference values, suggesting a shorter anterior cranial base and maxillary length. The frankfort horizontal plane-nasion-porion (FH-NPo) was higher than the reference value, and the Y-axis was lower than the reference value, indicating a more prognathic mandible. The angle subspinale-nasion-supramental (ANB) was lower than the reference value, indicating a skeletal angle Ⅲ malocclusion. The angle upper central incisor-nasion-subspinale (angle U1-NA) was higher than the reference value, indicating a lip inclination of maxillary central incisor. The angle lower central incisor-mandibular plane (IMPA) and lower central incisor-nasion-supramental (L1-NB) were lower than the reference values, indicating a retroclination of the mandibular central incisor, and crossbite in the maxillary and mandibular anterior teeth. Conclusion ·The dentofacial phenotype of PAX9-mutated patients with NSTA is reported comprehensively. It is helpful to improve the understanding of the role of PAX9 in human maxillofacial development.
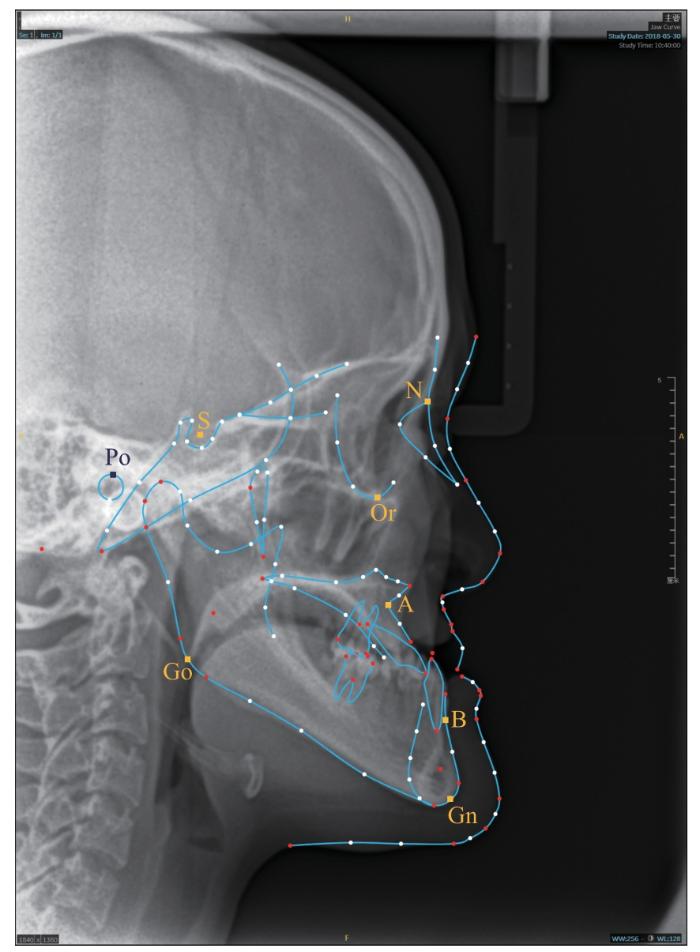
患者初诊时拍摄曲面体层摄影片及侧位X射线头影测量片。根据曲面体层摄影片确定恒牙胚缺失及缺牙位置和数目,使用iOrtho11.0在线软件进行X射线头影测量分析。X射线头影测量参数包括:上牙槽座角(angle sella-nasion-subspinale,SNA)、颌凸角(angle nasion-subspinale-subspinale-porion,NA-APo)、前颅底长度(sella-nasion,S-N)、面角(frankfort horizontal plane-nasion-porion,FH-NPo)、Y轴角(Y axis)、上/下牙槽座角(angle subspinale-nasion-supramental,ANB)、上中切牙倾斜度(upper central incisor-sella-nasion,U1-SN)、上中切牙角(angle upper central incisor-nasion-subspinale,angle U1-NA)、上中切牙距(distance of upper central incisor-nasion-subspinale,distance U1-NA)、下中切牙-下颌平面角(angle lower central incisor-mandibular plane,IMPA)、下中切牙凸度(lower central incisor-nasion-supramental,L1-NB)。
Note: The prevalence of missing teeth is presented as a heat map. The darker the red, the higher the frequency of missing; the darker the blue, the lower the frequency of missing. White background represent missing frequency close to the average missing frequency of all sites in the dentition (56.6%). Max—maxilla; Mand—mandible; Mo2—the second molar; Mo1—the first molar; PM2—the second premolar; PM1—the first premolar; Ca—canine; LI—lateral incisor; CI—central incisor.
Fig 2
Pattern of missing teeth in PAX9-mutated NSTA patients
Tab 2 Comparison between X-ray cephalometrics analysis parameters of patients with PAX9 mutation and classical norms
Parameter
Adult PAX9-mutated patients
Underage PAX9-mutated patients
Classical norm
Patient 2
Patient 7
SNA/(°)
75.3±4.1
80.5
79.3
82.8±4.1
NA-APo(convexity)/(°)
-17.8±11.0
-25.0
-5.8
6.0±4.4
S-N/mm
62.3±2.4
62.5
60.9
71.0±3.0
FH-NPo/(°)
95.8±3.5
99.9
92.2
85.4±3.7
Y axis/(°)
53.6±2.9
48.7
55.4
64.0±2.3
ANB/(°)
-6.8±4.7
-9.8
-3.4
2.7±2.0
U1-SN/(°)
111.4±14.7
110.9
109.4
105.7±6.3
Angle U1-NA/(°)
36.1±16.9
30.4
30.1
22.8±5.2
Distance U1-NA/mm
6.6±5.1
5.8
3.7
5.1±2.4
IMPA(L1-MP)/(°)
76.6±13.1
76.2
76.0
96.7±6.4
L1-NB/mm
0.3±2.9
0.7
0.7
6.7±2.1
Note: Parameters below the classical norms are shown in green, parameters above the classical norms are shown in red, and parameters within the classical norms are shown in black.
DOU Jiaqi was responsible for conceptualization, investigation, data curation, writing original draft, review and editing; GAO Jie and BIAN Xiaoling participated in clinical case collection; WANG Feng was responsible for review and editing; DAI Qinggang participated in conceptualization, supervision, review and editing; WU Yiqun was responsible for conceptualization, supervision, review and editing. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
POLDER B J, VAN′T HOF M A, VAN DER LINDEN F P, et al. A meta-analysis of the prevalence of dental agenesis of permanent teeth[J]. Community Dent Oral Epidemiol, 2004, 32(3): 217-226.
KHALAF K, MISKELLY J, VOGE E, et al. Prevalence of hypodontia and associated factors: a systematic review and meta-analysis[J]. J Orthod, 2014, 41(4): 299-316.
VASTARDIS H. The genetics of human tooth agenesis: new discoveries for understanding dental anomalies[J]. Am J Orthod Dentofacial Orthop, 2000, 117(6): 650-656.
TUNA E B, MARŞAN G, GENÇAY K, et al. Craniofacial and dental characteristics of Kabuki syndrome: nine years cephalometric follow-up[J]. J Clin Pediatr Dent, 2012, 36(4): 393-400.
GUNASHEKHAR M, HAMEED M S, BOKHARI S K. Oral and dental manifestations in Rubinstein-Taybi syndrome: report of a rare case[J]. Prim Dent Care, 2012, 19(1): 35-38.
VERMA L, PASSI S, GAUBA K. Brachman de Lange syndrome[J]. Contemp Clin Dent, 2010, 1(4): 268-270.
ERCAL D, SAY B. Cerebro-oculo-nasal syndrome: another case and review of the literature[J]. Clin Dysmorphol, 1998, 7(2): 139-141.
WU Z Y, YUE H T, LI J, et al. Two novel and de novoKMT2D mutations on the same allele cause Kabuki syndrome[J]. Chinese Journal of Stomatology, 2023, 58(8): 809-814.
FOURNIER B P, BRUNEAU M H, TOUPENAY S, et al. Patterns of dental agenesis highlight the nature of the causative mutated genes[J]. J Dent Res, 2018, 97(12): 1306-1316.
SARKAR T, RANJAN P, KANATHUR S, et al. An in vitro and computational validation of a novel loss-of-functional mutation in PAX9 associated with non-syndromic tooth agenesis[J]. Mol Genet Genomics, 2023, 298(1): 183-199.
BHOL C S, PATIL S, SAHU B B, et al. The clinical significance and correlative signaling pathways of paired box gene 9 in development and carcinogenesis[J]. Biochim Biophys Acta Rev Cancer, 2021, 1876(1): 188561.
CHU K Y, WANG Y L, CHEN J T, et al. PAX9 mutations and genetic synergism in familial tooth agenesis[J]. Ann N Y Acad Sci, 2023, 1524(1): 87-96.
LI R, CHEN Z, YU Q, et al. The function and regulatory network of Pax9 gene in palate development[J]. J Dent Res, 2019, 98(3): 277-287.
NAKATOMI M, LUDWIG K U, KNAPP M, et al. Msx1 deficiency interacts with hypoxia and induces a morphogenetic regulation during mouse lip development[J]. Development, 2020, 147(21): dev189175.
BONCZEK O, KREJCI P, IZAKOVICOVA-HOLLA L, et al. Tooth agenesis: what do we know and is there a connection to cancer?[J]. Clin Genet, 2021, 99(4): 493-502.
KAUSHAL K, KIM E J, TYAGI A, et al. Genome-wide screening for deubiquitinase subfamily identifies ubiquitin-specific protease 49 as a novel regulator of odontogenesis[J]. Cell Death Differ, 2022, 29(9): 1689-1704.
RAHMAN M M, LAI Y C, HUSNA A A, et al. Micro RNA transcriptome profile in canine oral melanoma[J]. Int J Mol Sci, 2019, 20(19): 4832.
WANG Y, GROPPE J C, WU J F, et al. Pathogenic mechanisms of tooth agenesis linked to paired domain mutations in human PAX9[J]. Hum Mol Genet, 2009, 18(15): 2863-2874.
INTARAK N, TONGCHAIRATI K, TERMTEERAPORNPIMOL K, et al. Tooth agenesis patterns and variants in PAX9: a systematic review[J]. Jpn Dent Sci Rev, 2023, 59: 129-137.
LIU H C, LIU H B, SU L X, et al. Four novel PAX9 variants and the PAX9-related non-syndromic tooth agenesis patterns[J]. Int J Mol Sci, 2022, 23(15): 8142.
WONG S W, HAN D, ZHANG H, et al. Nine novel PAX9 mutations and a distinct tooth agenesis genotype-phenotype[J]. J Dent Res, 2018, 97(2): 155-162.
FAUZI N H, ARDINI Y D, ZAINUDDIN Z, et al. A review on non-syndromic tooth agenesis associated with PAX9 mutations[J]. Jpn Dent Sci Rev, 2018, 54(1): 30-36.
LEE Y J, LEE Y J, KIM Y J, et al. Novel PAX9 mutations causing isolated oligodontia[J]. J Pers Med, 2024, 14(2): 191.
LEI R, QIU X L, HAN Y, et al. Identification and functional study of a novel variant of PAX9 causing tooth agenesis[J]. Oral Dis, 2024. DOI: 10.1111/odi.14937.
ZHOU M Q, ZHANG H, CAMHI H, et al. Analyses of oligodontia phenotypes and genetic etiologies[J]. Int J Oral Sci, 2021, 13(1): 32.
JARA-ESPEJO M, HAWKINS M T R, FOGALLI G B, et al. Folding stability of Pax9 intronic G-quadruplex correlates with relative molar size in eutherians[J]. Mol Biol Evol, 2021, 38(5): 1860-1873.
ROALD K L, WISTH P J, BØE O E. Changes in cranio-facial morphology of individuals with hypodontia between the ages of 9 and 16[J]. Acta Odontol Scand, 1982, 40(2): 65-74.
OGAARD B, KROGSTAD O. Craniofacial structure and soft tissue profile in patients with severe hypodontia[J]. Am J Orthod Dentofacial Orthop, 1995, 108(5): 472-477.
BEN-BASSAT Y, BRIN I. Skeletodental patterns in patients with multiple congenitally missing teeth[J]. Am J Orthod Dentofacial Orthop, 2003, 124(5): 521-525.
ENDO T, YOSHINO S, OZOE R, et al. Association of advanced hypodontia and craniofacial morphology in Japanese orthodontic patients[J]. Odontology, 2004, 92(1): 48-53.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}