目的·探究头颈部木村病患者计算机断层扫描(computed tomography,CT)和磁共振成像(magnetic resonance imaging,MRI)的影像学特征。方法·回顾性收集2009—2023年上海交通大学医学院附属第九人民医院经病理学确诊的头颈部木村病患者64例,所有患者均在术前完成CT和/或MRI增强成像。收集、记录及分析患者临床及影像学特征,其中包括年龄,性别,外周血嗜酸性粒细胞比例,血清IgE水平,病变位置、形态、大小、CT密度及强化程度、MRI信号及强化程度、表观扩散系数(apparent diffusion coefficient,ADC)、时间-信号强度曲线(time-signal intensity curve,TIC)类型、灌注速率及达峰时间(time to peak,TTP)。结果·64例木村病患者平均年龄(40±19)岁,男性占92.2%;73.5%患者嗜酸性粒细胞比例升高,所有检测血清IgE的患者(10例)IgE水平均升高。CT和MRI共发现结外病变(皮下和腺体病变)82个、淋巴结病变144个;结外病变中,80.5%表现为皮下或腺体内边界不清的斑片状病变,其他为边界清晰的结节状病变。所有病变在CT上均呈等密度影,在MRI上均表现为T1加权成像(T1-weighted imaging,T1WI)等信号,T2加权成像(T2-weighted imaging,T2WI)高信号。结外病变增强后多呈不均匀强化,而淋巴结病变增强后多呈均匀强化。结外病变和淋巴结病变的ADC中位数分别为1.04×10 -3 mm 2/s和0.67×10 -3 mm 2/s,差异具有统计学意义( P=0.000)。动态增强磁共振成像结果显示,结外病变的TIC类型主要为Ⅰ型和Ⅱ型,分别占57.5%和42.5%;而淋巴结病变TIC类型主要为Ⅱ型(96.6%)。结外病变和淋巴结病变的TTP和灌注速率,差异均具有统计学意义(均 P=0.000)。结论·木村病结外病变及淋巴结病变在CT上呈等密度影,在MRI上表现为T1WI等信号、T2WI高信号。结外病变ADC较高,TIC类型为Ⅰ或Ⅱ型,增强后多呈不均匀强化;淋巴结病变ADC较低,TIC类型多为Ⅱ型,增强后多呈均匀强化。
关键词:木村病
;
计算机断层扫描
;
磁共振成像
;
扩散加权成像
;
动态增强磁共振成像
Abstract
Objective ·To investigate the imaging features of computed tomography (CT) and magnetic resonance imaging (MRI) in the patients with Kimura disease (KD) in the head and neck. Methods ·Sixty-four cases of KD in the head and neck comfirmed by histopathology were retrospectively collected from 2009 to 2023 in Shanghai Ninth People′s Hospital, Shanghai Jiao Tong University School of Medicine. All patients completed CT and/or MRI enhancement imaging before surgery. Clinical and imaging characteristics were collected, recorded and analyzed, including age, gender, peripheral blood eosinophilic ratio, serum IgE level, the lesion location, shape, size, CT density and degree of enhancement, MRI signal intensity and degree of enhancement, apparent diffusion coefficient (ADC), time-signal intensity curve (TIC) patterns, wash-in rate, and time to peak (TTP). Results ·The average age of the 64 KD patients was (40±19) years, and 92.2% were males. A total of 73.5% of the patients showed an elevated ratio of peripheral blood eosinophil, and all 10 tested patients exhibited increased serum IgE levels. There were 82 extranodal (subcutaneous and glandular) lesions and 144 lymph node lesions detected by CT and MRI. Among the extranodal lesions, 80.5% were subcutaneous or glandular patchy lesions with unclear boundaries, and the rest were nodular lesions with clear boundaries. All lesions exhibited isodensity on CT scans and showed isointensity on T1-weighted imaging (T1WI) and hyperintensity on T2-weighted imaging (T2WI) in MRI. Most extranodal lesions tended to show heterogeneous enhancement, while most lymph node lesions showed homogeneous enhancement. The median ADCs of the extranodal lesions and the lymph node lesions were 1.04×10 -3 mm 2/s and 0.67×10 -3 mm 2/s, respectively, which were significantly different ( P=0.000). The dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) results showed that the TIC patterns of extranodal lesions were predominantly type Ⅰ and Ⅱ, accounting for 57.5% and 42.5%, respectively; while the TIC patterns of lymph node lesions were predominantly type Ⅱ (96.6%). The difference in the TTP and the wash-in rate between the extranodal lesions and the lymph node lesions were both statistically significant ( P=0.000). Conclusion ·Extranodal lesions and lymph node lesions of KD both show isodensity on CT, and isointensity on T1WI and hyperintensity on T2WI in MRI. Extranodal lesions often show high ADC, TIC type Ⅰ or Ⅱ, and mostly heterogeneous enhancement; lymph node lesions often show low ADC, TIC type Ⅱ, and mostly homogenous enhancement.
LUO Rui, YANG Gongxin, SHI Huimin, HAN Yongshun, HE Yining, TIAN Zhen, WU Yingwei. Study of imaging characteristics of Kimura disease in the head and neck. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2024, 44(9): 1182-1189 doi:10.3969/j.issn.1674-8115.2024.09.013
Tab 2 Imaging characteristics of extra-nodal lesions in 64 patients with Kimura disease ( n=82)
Item
Value
Location/ n(%)
Parotid +subcutaneous tissue
29 (35.4)
Lacrimal gland+subcutaneous tissue
1 (1.2)
Parotid
16 (19.5)
Subcutaneous tissue
36 (43.9)
Border/ n(%)
Well-defined
16 (19.5)
Ill-defined
66 (80.5)
Morphology/ n(%)
Patchy
66 (80.5)
Nodular
16 (19.5)
Maximum diameter/cm
4.3 (3.2, 5.8)
CT
Non-enhanced/ n(%) ①
Isodensity
53 (100.0)
Others
0 (0)
Enhancement ②
Homogenous/ n(%)
Marked
2 (3.9)
Others
0 (0)
Heterogeneous/ n(%)
Mild
7 (13.7)
Middle
24 (47.1)
Marked
18 (35.3)
MRI ③
T1WI/ n(%)
Isointensity
40 (100.0)
Others
0 (0)
T2WI/ n(%)
Hyperintensity
40 (100.0)
Others
0 (0)
Enhancement (fat suppression T1WI)
Homogenous/ n(%)
Marked
2 (5.0)
Others
0 (0)
Heterogeneous/ n(%)
Mild
1 (2.5)
Marked
37 (92.5)
Note:①There were 53 extra-nodal lesions observed in non-enhanced CT. ②There were 51 extra-nodal lesions observed in enhanced CT. ③There were 40 extra-nodal lesions observed in MRI.
Tab 3 Imaging characteristics of lymph node lesions in 64 patients with Kimura disease ( n=144)
Item
Value
Location/ n(%)
Neck
53 (36.8)
Parotid
91 (63.2)
Maximum diameter/cm
1.7 (1.3, 2.1)
CT
Non-enhanced/ n(%) ①
Isodensity
78 (100.0)
Others
0 (0)
Enhancement ②
Homogenous/ n(%)
Mild
7 (9.1)
Middle
35 (45.4)
Marked
35 (45.5)
Heterogeneous/ n(%)
0 (0)
MRI ③
T1WI/ n(%)
Isointensity
87 (100.0)
Others
0 (0)
T2WI/ n(%)
Hyperintensity
87 (100.0)
Others
0 (0)
Enhancement (fat suppression T1WI)
Homogenous/ n(%)
Mild
3 (3.4)
Marked
84 (96.6)
Heterogeneous/ n(%)
0 (0)
Note:①There were 78 lymph node lesions observed in non-enhanced CT. ②There were 77 lymph node lesions observed in enhanced CT. ③There were 87 lymph node lesions observed in MRI.
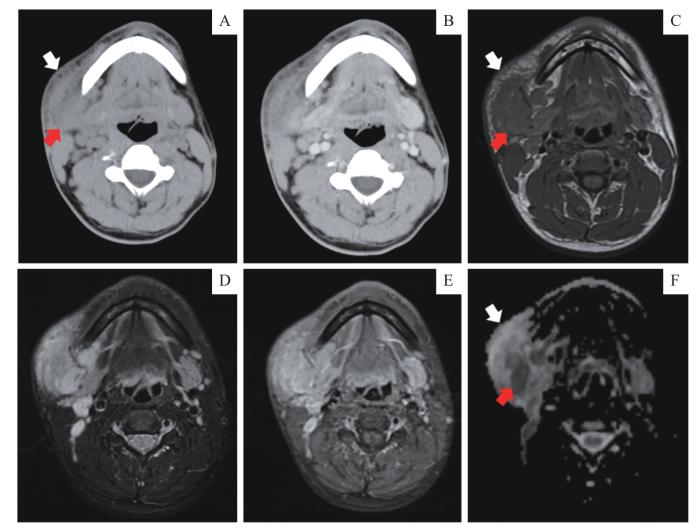
Note: A/B. Non-enhanced (A) and enhanced (B) axial CT scan showing an ill-defined patchy isodense lesion with adjacent skin thickening (white arrow) and an enlarged right cervical lymph node in the Ⅰb level (red arrow). C/D. An ill-defined patchy lesion with adjacent skin thickening (white arrow) and an enlarged lymph node (red arrow) in the axial T1WI (C) and fat-suppressed T2WI (D). E. In the axial fat-suppressed enhanced T1WI, the subcutaneous lesion showed heterogeneous hyperenhancement. F. ADC map showing that the ADC value of the subcutaneous lesion (white arrow) was higher than that of the lymph node lesion (red arrow).
Fig 1
Imaging manifestations of a patchy lesion in the right buccal subcutaneous tissues of a patient
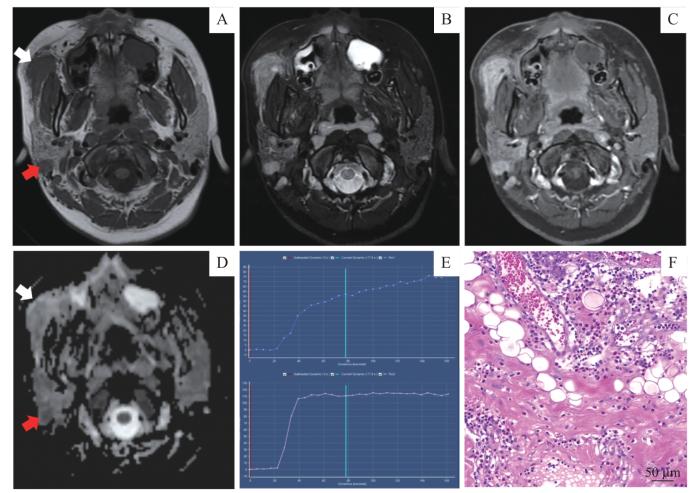
Note: A/B. Axial T1WI (A) and fat-suppressed T2WI (B) showing a well-defined nodular lesion (white arrow) and an enlarged lymph node (red arrow). C. Homogeneous hyperenhancement of the subcutaneous lesion on axial fat-suppressed enhanced T1WI. D. ADC map showing that the ADC value of the subcutaneous lesion (white arrow) was higher than that of the lymph node lesion (red arrow). E. TIC patterns of the subcutaneous lesion (top) and the lymph node lesion (bottom). F. The subcutaneous lesion showing hyperplastic follicles with diffused eosinophilic infiltration (hematoxylin-eosin staining, ×400).
Fig 2
Imaging and histopathological manifestations of a nodular lesion in the right buccal subcutaneous tissues of a patient
MRI功能成像,如DWI和DCE-MRI,可提供定性、定量或半定量的结果,除解剖结构外,还包括组织、细胞成分,血流动力学特征等病理生理过程。HORIKOSHI等 [ 9]在一个样本量7人的回顾性研究中,得到结外病变及淋巴结病变ADC分别为(1.21±0.33)×10 -3 mm 2/s和(0.91±0.25)×10 -3 mm 2/s;且结外病变在DCE-MRI上呈渐进性强化,而淋巴结病变呈现早期强化。本研究的结果大致与该文献结果一致,我们测得的结外病变及淋巴结病变ADC中位数分别为1.04×10 -3 mm 2/s和0.67×10 -3 mm 2/s,且差异具有统计学意义。在DCE-MRI上,57.5%结外病变表现为渐进性强化(Ⅰ型),42.5%表现为早期强化后持续强化(Ⅱ型);而淋巴结病变中均表现为早期强化,96.6%达峰后表现为持续强化(Ⅱ型),3.4%达峰后表现为廓清(Ⅲ型)。木村病患者的结外病变与淋巴结病变在ADC值及TIC类型上的差异,可能是由于结外病变比淋巴结病变包含更多的纤维化组织,这些纤维化组织导致它们在DCE-MRI上表现为逐渐增强,而淋巴结病变的细胞密度更高导致其在DWI上表现为明显高信号(ADC值更低)。此外,我们还发现结外病变的TTP显著长于淋巴结病变,从另一侧面证实结外病变在注射对比剂后渐进性强化的模式。
The manuscript was drafted by LUO Rui. Study implementation was completed by LUO Rui and YANG Gongxin. Data collection was completed by LUO Rui, YANG Gongxin and TIAN Zhen. The data was analyzed by LUO Rui and HE Yining. The manuscript was revised by WU Yingwei, SHI Huimin and HAN Yongshun. The study was designed and supervised by WU Yingwei. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
CHAN J K, HUI P K, NG C S, et al. Epithelioid haemangioma (angiolymphoid hyperplasia with eosinophilia) and Kimura′s disease in Chinese[J]. Histopathology, 1989, 15(6): 557-574.
LI T J, CHEN X M, WANG S Z, et al. Kimura′s disease: a clinicopathologic study of 54 Chinese patients[J]. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1996, 82(5): 549-555.
KELLY H R, CURTIN H D. Chapter 2 squamous cell carcinoma of the head and neck-imaging evaluation of regional lymph nodes and implications for management[J]. Semin Ultrasound CT MR, 2017, 38(5): 466-478.
HASHIDA Y, HIGUCHI T, NAKAJIMA K, et al. Human polyomavirus 6 with the Asian-Japanese genotype in cases of Kimura disease and angiolymphoid hyperplasia with eosinophilia[J]. J Invest Dermatol, 2020, 140(8): 1650-1653.e4.
KING R L, TAN B, CRAIG F E, et al. Reactive eosinophil proliferations in tissue and the lymphocytic variant of hypereosinophilic syndrome[J]. Am J Clin Pathol, 2021, 155(2): 211-238.
SATO R, BANDOH N, GOTO T, et al. Kimura disease presenting with buccal mass: a case report and literature review[J]. Head Neck Pathol, 2021, 15(2): 657-662.
SANGWAN A, GOYAL A, BHALLA A S, et al. Kimura disease: a case series and systematic review of clinico-radiological features[J]. Curr Probl Diagn Radiol, 2022, 51(1): 130-142.
ZHU W X, ZHANG Y Y, SUN Z P, et al. Differential diagnosis of immunoglobulin G4-related sialadenitis and Kimura′s disease of the salivary gland: a comparative case series[J]. Int J Oral Maxillofac Surg, 2021, 50(7): 895-905.
WANG J, TANG Z H, FENG X Y, et al. Preliminary study of diffusion-weighted imaging and magnetic resonance spectroscopy imaging in Kimura disease[J]. J Craniofac Surg, 2014, 25(6): 2147-2151.
SUROV A, MEYER H J, WIENKE A. Apparent diffusion coefficient for distinguishing between malignant and benign lesions in the head and neck region: a systematic review and meta-analysis[J]. Front Oncol, 2020, 9: 1362.
BAIK J, BAEK H J, RYU K H, et al. MALT lymphoma of the tongue in a patient with Sjögren′s syndrome: a case report and literature review[J]. Diagnostics, 2021, 11(9): 1715.
... MRI功能成像,如DWI和DCE-MRI,可提供定性、定量或半定量的结果,除解剖结构外,还包括组织、细胞成分,血流动力学特征等病理生理过程.HORIKOSHI等 [ 9]在一个样本量7人的回顾性研究中,得到结外病变及淋巴结病变ADC分别为(1.21±0.33)×10 -3 mm 2/s和(0.91±0.25)×10 -3 mm 2/s;且结外病变在DCE-MRI上呈渐进性强化,而淋巴结病变呈现早期强化.本研究的结果大致与该文献结果一致,我们测得的结外病变及淋巴结病变ADC中位数分别为1.04×10 -3 mm 2/s和0.67×10 -3 mm 2/s,且差异具有统计学意义.在DCE-MRI上,57.5%结外病变表现为渐进性强化(Ⅰ型),42.5%表现为早期强化后持续强化(Ⅱ型);而淋巴结病变中均表现为早期强化,96.6%达峰后表现为持续强化(Ⅱ型),3.4%达峰后表现为廓清(Ⅲ型).木村病患者的结外病变与淋巴结病变在ADC值及TIC类型上的差异,可能是由于结外病变比淋巴结病变包含更多的纤维化组织,这些纤维化组织导致它们在DCE-MRI上表现为逐渐增强,而淋巴结病变的细胞密度更高导致其在DWI上表现为明显高信号(ADC值更低).此外,我们还发现结外病变的TTP显著长于淋巴结病变,从另一侧面证实结外病变在注射对比剂后渐进性强化的模式. ...



{kind=link}
{kind=link}
{kind=link}
{kind=link}