目的·探讨2型糖尿病患者腹部脂肪面积与胰岛β细胞第一时相分泌功能之间的关系,并建立列线图预测模型。方法·选取2020年10月—2024年2月在复旦大学附属中山医院内分泌科住院并完善精氨酸刺激试验以评估胰岛β细胞第一时相分泌功能的2型糖尿病患者120例。根据试验结果,将患者分为胰岛素分泌功能残存组和功能衰竭组。收集患者的一般资料及实验室指标,通过内脏脂肪检测仪检测患者腹部皮下脂肪面积(subcutaneous fat area,SFA)和内脏脂肪面积(visceral fat area,VFA)。经单因素分析筛选变量,使用多因素Logistic回归确定影响因素,从而建立列线图预测模型。采用受试者操作特征曲线(receiver operating characteristic curve,ROC曲线)分析的曲线下面积(area under the curve,AUC)、一致性指数(concordance index,C-index)评估模型预测效能。结果·纳入的74例患者(61.7%)胰岛功能残存,46例(38.3%)胰岛功能衰竭。胰岛功能衰竭组患者糖尿病病程更长,腰围、臀围、体质量指数(body mass index,BMI)、尿酸、游离三碘甲状腺原氨酸(free triiodothyronine,FT3)、脂肪组织胰岛素抵抗指数(adipose tissue insulin resistance,Adipo-IR)、踝肱指数(ankle brachial index,ABI)、SFA和VFA水平较低,臂踝脉搏波速度(brachial ankle pulse wave velocity,baPWV)较快。多因素Logistic回归分析显示,SFA、VFA、FT3、baPWV和ABI是胰岛功能衰竭的独立危险因素。基于以上因素构建列线图模型,其中纳入VFA、FT3、ABI、baPWV的模型预测能力最佳,C-index为0.81。结论·胰岛β细胞第一时相分泌功能衰竭患者SFA和VFA均较低,纳入SFA或VFA的列线图可用于预测2型糖尿病患者β细胞第一时相分泌功能。
关键词:2型糖尿病
;
腹部脂肪面积
;
胰岛功能
;
列线图
Abstract
Objective ·To explore the relationship between abdominal fat area and the first-phase insulin secretion function of pancreatic β-cells in patients with type 2 diabetes, and to establish predictive models of nomogram. Methods ·From October 2020 to February 2024, a total of 120 patients with type 2 diabetes, who were hospitalized in the Department of Endocrinology, Zhongshan Hospital, Fudan University, and underwent the arginine stimulation test, were recruited for the study. Patients were categorized into an insulin secretion function-preserved group (i.e. preserved group) and a depleted group according to the results of the arginine stimulation test. General information and laboratory parameters were collected. Subcutaneous fat area (SFA) and visceral fat area (VFA) were non-invasively measured by abdominal fat detector. The variables were screened by univariate analysis, and multivariate Logistic regression was used to identify the influencing factors, followed by the establishment of predictive models of nomogram. The area under the receiver operating characteristic curve (ROC curve) and concordance index (C-index) were used to evaluate the predictive performance of the models. Results ·Seventy-four patients (61.7%) were assigned to the preserved group, and 46 patients (38.3%) to the depleted group. Patients in the depleted group had a longer diabetes duration, lower waist circumference, hip circumference, body mass index (BMI), uric acid, free triiodothyronine (FT3), adipose tissue insulin resistance (Adipo-IR), ankle brachial index (ABI), SFA and VFA, and higher brachial ankle pulse wave velocity (baPWV). Multivariate Logistic regression showed that SFA, VFA, FT3, baPWV, and ABI were independent risk factors for the depleted insulin secretion function. Nomogram models were constructed based on the above risk factors. Among them, the model comprising VFA, FT3, ABI, and baPWV showed the best predictive performance with a C-index of 0.81. Conclusion ·SFA and VFA are lower in patients with depleted first-phase insulin secretion function of pancreatic β-cells. The nomogram model, including SFA or VFA, can be used to predict first-phase insulin secretion function of pancreatic β-cells in patients with type 2 diabetes.
Keywords:type 2 diabetes
;
abdominal fat area
;
insulin secretion function
;
nomogram
LU Jiaping, LIU Xing, ZHANG Linshan, ZHAO Lin, ZHANG Min, LI Xiaoying, LIU Yuejun. Relationship between abdominal fat area and first-phase insulin secretion function of pancreatic β-cells in patients with type 2 diabetes. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(1): 42-50 doi:10.3969/j.issn.1674-8115.2025.01.005
本研究拟运用内脏脂肪检测仪无创测量的腹部脂肪面积,分析腹部脂肪面积与2型糖尿病患者胰岛β细胞第一时相分泌功能的关系,建立预测模型。并采用受试者操作特征曲线(receiver operating characteristic curve,ROC曲线)的曲线下面积(area under the curve,AUC)和一致性指数(concordance index,C-index)评估模型的预测效能。本研究旨在协助临床医师快速简便评估2型糖尿病患者的胰岛功能,从而及时启动胰岛素治疗。
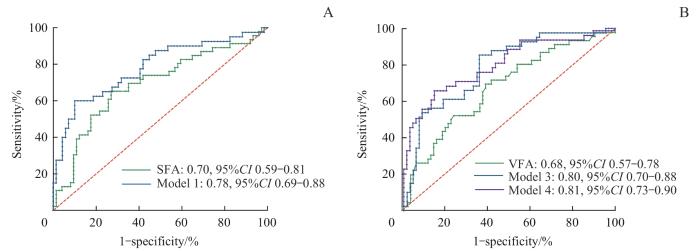
Note: A. Models including SFA for predicting depleted insulin secretion function. B. Models including VFA for predicting depleted insulin secretion function.
Fig 1
ROC curve of models for predicting depleted first-phase insulin secretion function of β-cells
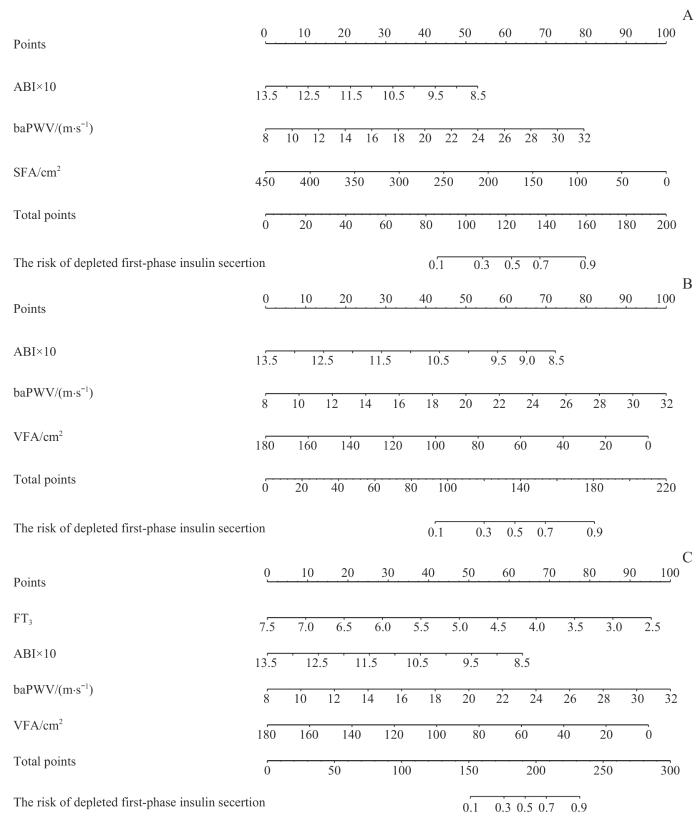
Note: A. SFA-simple model involved SFA and non-invasive markers. B. VFA-simple model involved VFA and non-invasive markers. C. VFA-invasive model involved VFA and biomarkers.
Fig 2
Nomogram models for predicting depleted first-phase insulin secretion function of β-cells
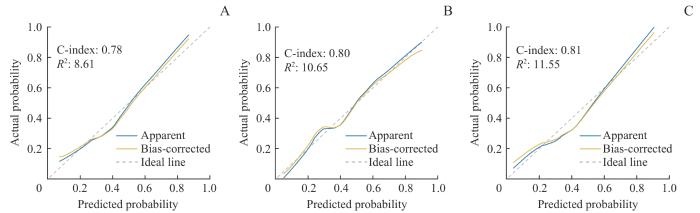
Note: A. SFA-simple model. B. VFA-simple model. C. VFA-invasive model. The dashed grey lines represent perfect prediction (ideal line); the blue lines represent the entire cohort (apparent); the yellow lines, bias-corrected via bootstrapping (with 1 000 replicates), indicate observed nomogram performance (bias-corrected).
本研究多因素Logistic回归提示脂肪面积联合baPWV和ABI能预测胰岛分泌功能。BaPWV和ABI是2个评估动脉粥样硬化简单、实用的无创指标,但也与糖代谢密切相关。文献报告,baPWV与空腹和2 h C肽水平正相关,这表明内源性胰岛素分泌与动脉硬化之间存在密切联系[17]。此外,baPWV的增加先于空腹血糖升高,也是糖尿病发生的危险因素[18]。糖尿病患者中,ABI与心血管结局和死亡独立相关,与中层动脉钙化引起的动脉硬度增加有关[19]。机制上,糖尿病时的低度炎症破坏内皮功能,导致动脉壁硬度增加,从而加重毛细血管损伤。动脉硬度增加会损害高流量低阻力器官的功能,例如胰腺,从而影响胰岛分泌功能。毛细血管功能障碍引起的组织灌流减少也会损害肌肉等组织的功能,进一步影响糖代谢。此外,低度炎症和氧化应激是糖尿病和动脉硬度的共同病理特征,彼此相互影响[18]。因此,baPWV和ABI可以作为胰岛分泌功能的良好预测指标。
LIU Yuejun designed the study. LIU Xing, ZHANG Linshan, and ZHAO Lin recruited the participants. LU Jiaping collected the data. LIU Yuejun, LU Jiaping, and LIU Xing analyzed the data and wrote the manuscript. ZHANG Min and LI Xiaoying provided guidance on the article. LU Jiaping and LIU Xing contributed equally to this study. All the authors have read the final version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclare no relevant conflict of interests.
SUN H, SAEEDI P, KARURANGA S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045[J]. Diabetes Res Clin Pract, 2022, 183: 109119.
NAUCK M A, WEFERS J, MEIER J J. Treatment of type 2 diabetes: challenges, hopes, and anticipated successes[J]. Lancet Diabetes Endocrinol, 2021, 9(8): 525-544.
HANNON T S, KAHN S E, UTZSCHNEIDER K M, et al. Review of methods for measuring β-cell function: design considerations from the Restoring Insulin Secretion (RISE) Consortium[J]. Diabetes Obes Metab, 2018, 20(1): 14-24.
KIM E H, KIM H K, LEE M J, et al. Sex differences of visceral fat area and visceral-to-subcutaneous fat ratio for the risk of incident type 2 diabetes mellitus[J]. Diabetes Metab J, 2022, 46(3): 486-498.
GYLLENHAMMER L E, ALDERETE T L, TOLEDO-CORRAL C M, et al. Saturation of subcutaneous adipose tissue expansion and accumulation of ectopic fat associated with metabolic dysfunction during late and post-pubertal growth[J]. Int J Obes (Lond), 2016, 40(4): 601-606.
Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition)[J]. Chinese Journal of Diabetes, 2021, 13(4): 315-409.
TER HORST K W, VAN GALEN K A, GILIJAMSE P W, et al. Methods for quantifying adipose tissue insulin resistance in overweight/obese humans[J]. Int J Obes (Lond), 2017, 41(8): 1288-1294.
ZHU X P, YAN H M, CHANG X X, et al. The value of arginine stimulation test in evaluating the first-phase insulin secretion and its guiding role for the treatment of type 2 diabetes mellitus[J]. Chinese Journal of Clinical Medicine, 2017, 24(4): 548-553.
SASSO M, BEAUGRAND M, DE LEDINGHEN V, et al. Controlled attenuation parameter (CAP): a novel VCTE™ guided ultrasonic attenuation measurement for the evaluation of hepatic steatosis: preliminary study and validation in a cohort of patients with chronic liver disease from various causes[J]. Ultrasound Med Biol, 2010, 36(11): 1825-1835.
SMITH U, KAHN B B. Adipose tissue regulates insulin sensitivity: role of adipogenesis, de novo lipogenesis and novel lipids[J]. J Intern Med, 2016, 280(5): 465-475.
LI R, LU W, JIA J, et al. Relationships between indices of obesity and its cardiovascular comorbidities in a Chinese population[J]. Circ J, 2008, 72(6): 973-978.
NEELAND I J, TURER A T, AYERS C R, et al. Dysfunctional adiposity and the risk of prediabetes and type 2 diabetes in obese adults[J]. JAMA, 2012, 308(11): 1150-1159.
LI H T, WU G Y, FANG Q C, et al. Fibroblast growth factor 21 increases insulin sensitivity through specific expansion of subcutaneous fat[J]. Nat Commun, 2018, 9(1): 272.
CHEN S, CHU A H, BIAN W X, et al. Correlation between skeletal muscle mass and islet function in patients with type 2 diabetes mellitus[J]. Chinese Journal of Clinical Research, 2024, 37(7): 1045-1050.
SUN Y C, ZHU Y Q, ZHANG L, et al. Relationship between insulin secretion and arterial stiffness in essential hypertension[J]. Int J Hypertens, 2021, 2021: 5015797.
NIE F Z, HE J A, CAO H, et al. Predictive value of abnormal ankle-brachial index in patients with diabetes: a meta-analysis[J]. Diabetes Res Clin Pract, 2021, 174: 108723.
TEIXEIRA P F D S, DOS SANTOS P B, PAZOS-MOURA C C. The role of thyroid hormone in metabolism and metabolic syndrome[J]. Ther Adv Endocrinol Metab, 2020, 11: 2042018820917869.
MORAN C, MCENIERY C M, SCHOENMAKERS N, et al. Dyslipidemia, insulin resistance, ectopic lipid accumulation, and vascular function in resistance to thyroid hormone β[J]. J Clin Endocrinol Metab, 2021, 106(5): e2005-e2014.
YAN Y, NIU Z M, SUN C, et al. Hepatic thyroid hormone signalling modulates glucose homeostasis through the regulation of GLP-1 production via bile acid-mediated FXR antagonism[J]. Nat Commun, 2022, 13(1): 6408.
VERGA FALZACAPPA C, PATRIARCA V, BUCCI B, et al. The TRβ1 is essential in mediating T3 action on Akt pathway in human pancreatic insulinoma cells[J]. J Cell Biochem, 2009, 106(5): 835-848.
... 本研究多因素Logistic回归提示脂肪面积联合baPWV和ABI能预测胰岛分泌功能.BaPWV和ABI是2个评估动脉粥样硬化简单、实用的无创指标,但也与糖代谢密切相关.文献报告,baPWV与空腹和2 h C肽水平正相关,这表明内源性胰岛素分泌与动脉硬化之间存在密切联系[17].此外,baPWV的增加先于空腹血糖升高,也是糖尿病发生的危险因素[18].糖尿病患者中,ABI与心血管结局和死亡独立相关,与中层动脉钙化引起的动脉硬度增加有关[19].机制上,糖尿病时的低度炎症破坏内皮功能,导致动脉壁硬度增加,从而加重毛细血管损伤.动脉硬度增加会损害高流量低阻力器官的功能,例如胰腺,从而影响胰岛分泌功能.毛细血管功能障碍引起的组织灌流减少也会损害肌肉等组织的功能,进一步影响糖代谢.此外,低度炎症和氧化应激是糖尿病和动脉硬度的共同病理特征,彼此相互影响[18].因此,baPWV和ABI可以作为胰岛分泌功能的良好预测指标. ...
2
... 本研究多因素Logistic回归提示脂肪面积联合baPWV和ABI能预测胰岛分泌功能.BaPWV和ABI是2个评估动脉粥样硬化简单、实用的无创指标,但也与糖代谢密切相关.文献报告,baPWV与空腹和2 h C肽水平正相关,这表明内源性胰岛素分泌与动脉硬化之间存在密切联系[17].此外,baPWV的增加先于空腹血糖升高,也是糖尿病发生的危险因素[18].糖尿病患者中,ABI与心血管结局和死亡独立相关,与中层动脉钙化引起的动脉硬度增加有关[19].机制上,糖尿病时的低度炎症破坏内皮功能,导致动脉壁硬度增加,从而加重毛细血管损伤.动脉硬度增加会损害高流量低阻力器官的功能,例如胰腺,从而影响胰岛分泌功能.毛细血管功能障碍引起的组织灌流减少也会损害肌肉等组织的功能,进一步影响糖代谢.此外,低度炎症和氧化应激是糖尿病和动脉硬度的共同病理特征,彼此相互影响[18].因此,baPWV和ABI可以作为胰岛分泌功能的良好预测指标. ...
... [18].因此,baPWV和ABI可以作为胰岛分泌功能的良好预测指标. ...
1
... 本研究多因素Logistic回归提示脂肪面积联合baPWV和ABI能预测胰岛分泌功能.BaPWV和ABI是2个评估动脉粥样硬化简单、实用的无创指标,但也与糖代谢密切相关.文献报告,baPWV与空腹和2 h C肽水平正相关,这表明内源性胰岛素分泌与动脉硬化之间存在密切联系[17].此外,baPWV的增加先于空腹血糖升高,也是糖尿病发生的危险因素[18].糖尿病患者中,ABI与心血管结局和死亡独立相关,与中层动脉钙化引起的动脉硬度增加有关[19].机制上,糖尿病时的低度炎症破坏内皮功能,导致动脉壁硬度增加,从而加重毛细血管损伤.动脉硬度增加会损害高流量低阻力器官的功能,例如胰腺,从而影响胰岛分泌功能.毛细血管功能障碍引起的组织灌流减少也会损害肌肉等组织的功能,进一步影响糖代谢.此外,低度炎症和氧化应激是糖尿病和动脉硬度的共同病理特征,彼此相互影响[18].因此,baPWV和ABI可以作为胰岛分泌功能的良好预测指标. ...



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}