嵌合抗原受体T细胞(chimeric antigen receptor T cell,CAR-T细胞)治疗通过基因工程改造T细胞,使其能够特异性识别并高效清除靶细胞,在B细胞淋巴瘤、白血病等血液系统恶性肿瘤的治疗中取得了突破性成就。基于该疗法独特的治疗原理,研究人员积极探索以拓展其在其他疾病领域的应用,其中,CAR-T细胞治疗在自身免疫性疾病(autoimmune disease,AID)的治疗中展现出巨大潜力并备受关注。目前,AID的传统治疗方案(如糖皮质激素、免疫抑制剂和生物制剂等)常面临疗效有限、缓解期短及长期毒性等诸多问题。相比之下,CAR-T细胞治疗凭借其精准靶向和可诱导持续无药物缓解的优势,成为AID极具前景的治疗策略。该文回顾CAR-T细胞治疗在多种AID中的临床前和临床研究进展,阐述该疗法清除致病性B细胞及重建免疫平衡的可行性。同时重点探讨CAR-T细胞治疗面临的主要挑战,包括不良反应、持久性不足及部分患者存在抵抗性等问题,并进一步从优化嵌合抗原受体(chimeric antigen receptor,CAR)结构、探索特异性靶点及开发通用型CAR-T细胞等方面提出应对策略,阐释其未来的发展方向,旨在为CAR-T细胞治疗在AID中的进一步开发和优化提供理论依据。
关键词:嵌合抗原受体T细胞
;
细胞免疫疗法
;
自身免疫性疾病
Abstract
Chimeric antigen receptor T cell (CAR-T) therapy, which involves genetically engineering T cells to specifically recognize and efficiently eliminate target cells, has achieved groundbreaking success in treating hematological malignancies such as B-cell lymphoma and leukemia. Driven by its unique mechanism of action, research into extending its applications to other disease areas is actively underway. In particular, CAR-T therapy has shown significant potential in treating autoimmune diseases (AIDs), attracting considerable attention. Current conventional treatments for AIDs, including glucocorticoids, immunosuppressants, and biologics, are often associated with limitations such as limited efficacy, short duration of remission, and long-term toxicity. In contrast, CAR-T therapy has emerged as a highly promising treatment strategy for AIDs, owing to its advantages of precise targeting and the capacity to induce sustained, drug-free remission. This article reviews recent preclinical and clinical advances in CAR-T therapy for various AIDs, demonstrating its feasibility in eradicating pathogenic B cells and reestablishing immune tolerance. It also examines the major challenges confronting this treatment approach, including adverse effects, limited persistence, and treatment resistance in some patients. Furthermore, strategies to address these challenges are discussed, focusing on the optimization of the chimeric antigen receptor (CAR) structure, the exploration of novel specific targets, and the development of universal CAR-T products. Finally, future research directions are outlined, with the aim of providing a rational foundation for the further development and refinement of CAR-T therapy for AIDs.
WANG Xueyi, LI Benshang. Review of CAR-T cell therapy for autoimmune diseases. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(11): 1432-1442 doi:10.3969/j.issn.1674-8115.2025.11.003
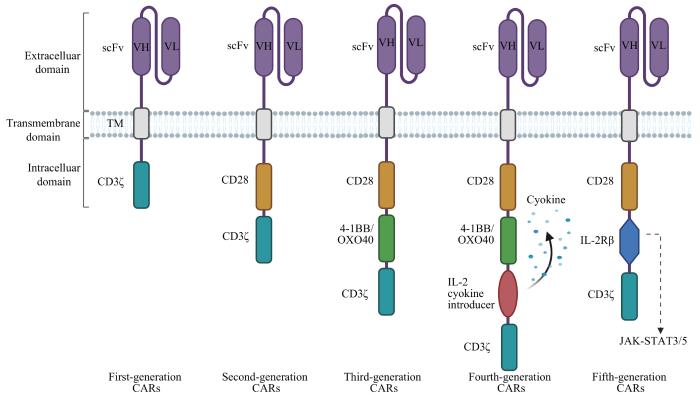
当前CAR的结构经历了5代变化(图1)。一代CAR-T细胞胞内结构域包含CD3ζ链,但由于缺少共刺激结构域,其扩增能力和持久性欠佳、抗癌活性不足。二代CAR-T细胞在一代基础上增加了1个共刺激结构域(CD28、4-1BB或OXO40等),增殖能力、持久性和细胞毒性均显著提高。三代CAR-T细胞包含2种共刺激结构域以进一步增强其信号激活、靶向毒性并延长增殖,但由于其活性增加且不可控,可能导致细胞因子风暴、多器官衰竭甚至死亡等严重不良反应,临床上与二代CAR-T细胞相比不具优势[8-10]。四代CAR-T细胞添加白细胞介素-2(interleukin-2,IL-12)等免疫调节因子以激活先天性免疫细胞并增强T细胞活化,一定程度上克服肿瘤微环境中的免疫抑制因素,更有力地攻击实体肿瘤。五代CAR-T细胞涉及对传统CAR结构进行改造,如添加IL-2受体β链触发细胞因子Janus激酶-信号转导与转录激活因子3/5(Janus kinase-signal transducer and activator of transcription 3/5,JAK-STAT3/5)信号转导以增强CAR-T细胞活性[11],以及使用CRISPR-Cas9技术敲除T细胞中的人类白细胞抗原Ⅰ类分子(human leukocyte antigen class Ⅰ,HLA-Ⅰ)和内源性T细胞受体制备通用型CAR-T细胞,降低CAR-T细胞被排斥和GVHD的风险[12]。
基于CAR-T细胞的基本原理,目前已经开发出嵌合自身抗体受体T细胞(chimeric autoantibody receptor T cell,CAAR-T细胞)和嵌合抗原受体调节性T细胞(chimeric antigen receptor regulatory T cell,CAR-Treg细胞)治疗,这两者在AID的治疗中各具优势。
调节性T细胞(regulatory T cell,Treg细胞)是具有免疫抑制功能的CD4+ T细胞亚群,对维持免疫耐受至关重要。与传统CAR-T细胞相比,CAR-Treg细胞不仅能诱导靶细胞死亡,还可通过多种机制抑制效应T细胞功能。目前该疗法已经在T1DM[30]、溃疡性结肠炎[34]和多发性硬化[37]等多种AID的临床前研究中取得显著成效(表1)。同时,MACDONALD等[41]发现HLA-A2 CAR-Tregs可以防止免疫缺陷小鼠发生GVHD(表1)。CAR-Treg细胞凭借其抗原特异性强、免疫抑制功能独特及潜在不良反应小等优势,尽管仍需克服体外扩增困难和体内持久性不足等挑战,未来仍有望通过联合疗法维持长期疗效,成为AID治疗领域的重要候选策略。
WANG Xueyi was responsible for writing and revising the paper. LI Benshang was responsible for reviewing and revising the paper. Both authors have read the final version of paper and consented to its submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
Both authors declare no relevant conflict of interests.
SU M, ZHAO C B, LUO S S. Therapeutic potential of chimeric antigen receptor based therapies in autoimmune diseases[J]. Autoimmun Rev, 2022, 21(1): 102931.
PORTER D L, LEVINE B L, KALOS M, et al. Chimeric antigen receptor-modified T cells in chronic lymphoid leukemia[J]. N Engl J Med, 2011, 365(8): 725-733.
JUNE C H, O'CONNOR R S, KAWALEKAR O U, et al. CAR T cell immunotherapy for human cancer[J]. Science, 2018, 359(6382): 1361-1365.
BOYIADZIS M M, DHODAPKAR M V, BRENTJENS R J, et al. Chimeric antigen receptor (CAR) T therapies for the treatment of hematologic malignancies: clinical perspective and significance[J]. J Immunother Cancer, 2018, 6(1): 137.
LI X D, LI W, XU L P, et al. Chimeric antigen receptor-immune cells against solid tumors: structures, mechanisms, recent advances, and future developments[J]. Chin Med J (Engl), 2024, 137(11): 1285-1302.
YEKU O O, BRENTJENS R J. Armored CAR T-cells: utilizing cytokines and pro-inflammatory ligands to enhance CAR T-cell anti-tumour efficacy[J]. Biochem Soc Trans, 2016, 44(2): 412-418.
TANG X Y, SUN Y, ZHANG A, et al. Third-generation CD28/4-1BB chimeric antigen receptor T cells for chemotherapy relapsed or refractory acute lymphoblastic leukaemia: a non-randomised, open-label phase Ⅰ trial protocol[J]. BMJ Open, 2016, 6(12): e013904.
LOCK D, MOCKEL-TENBRINCK N, DRECHSEL K, et al. Automated manufacturing of potent CD20-directed chimeric antigen receptor T cells for clinical use[J]. Hum Gene Ther, 2017, 28(10): 914-925.
UTKARSH K, SRIVASTAVA N, KUMAR S, et al. CAR-T cell therapy: a game-changer in cancer treatment and beyond[J]. Clin Transl Oncol, 2024, 26(6): 1300-1318.
KANSAL R, RICHARDSON N, NEELI I, et al. Sustained B cell depletion by CD19-targeted CAR T cells is a highly effective treatment for murine lupus[J]. Sci Transl Med, 2019, 11(482): eaav1648.
JIN X X, XU Q, PU C F, et al. Therapeutic efficacy of anti-CD19 CAR-T cells in a mouse model of systemic lupus erythematosus[J]. Cell Mol Immunol, 2021, 18(8): 1896-1903.
MACKENSEN A, MÜLLER F, MOUGIAKAKOS D, et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus[J]. Nat Med, 2022, 28(10): 2124-2132.
ZHANG W L, FENG J, CINQUINA A, et al. Treatment of systemic lupus erythematosus using BCMA-CD19 compound CAR[J]. Stem Cell Rev Rep, 2021, 17(6): 2120-2123.
OREN S, MANDELBOIM M, BRAUN-MOSCOVICI Y, et al. Vaccination against influenza in patients with rheumatoid arthritis: the effect of rituximab on the humoral response[J]. Ann Rheum Dis, 2008, 67(7): 937-941.
GOTTENBERG J E, RAVAUD P, BARDIN T, et al. Risk factors for severe infections in patients with rheumatoid arthritis treated with rituximab in the autoimmunity and rituximab registry[J]. Arthritis Rheum, 2010, 62(9): 2625-2632.
ZHANG B, WANG Y, YUAN Y S, et al. In vitro elimination of autoreactive B cells from rheumatoid arthritis patients by universal chimeric antigen receptor T cells[J]. Ann Rheum Dis, 2021, 80(2): 176-184.
WHITTINGTON K B, PRISLOVSKY A, BEATY J, et al. CD8+ T cells expressing an HLA-DR1 chimeric antigen receptor target autoimmune CD4+ T cells in an antigen-specific manner and inhibit the development of autoimmune arthritis[J]. J Immunol, 2022, 208(1): 16-26.
TAUBMANN J, KNITZA J, MÜLLER F, et al. Rescue therapy of antisynthetase syndrome with CD19-targeted CAR-T cells after failure of several B-cell depleting antibodies[J]. Rheumatology (Oxford), 2024, 63(1): e12-e14.
PECHER A C, HENSEN L C, KLEIN R, et al. CD19-targeting CAR T cells for myositis and interstitial lung disease associated with antisynthetase syndrome[J]. JAMA, 2023, 329(24): 2154-2162.
ZHANG L, SOSINOWSKI T, COX A R, et al. Chimeric antigen receptor (CAR) T cells targeting a pathogenic MHC class Ⅱ: peptide complex modulate the progression of autoimmune diabetes[J]. J Autoimmun, 2019, 96: 50-58.
FISHMAN S, LEWIS M D, SIEW L K, et al. Adoptive transfer of mRNA-transfected T cells redirected against diabetogenic CD8 T cells can prevent diabetes[J]. Mol Ther, 2017, 25(2): 456-464.
KOBAYASHI S, THELIN M A, PARRISH H L, et al. A biomimetic five-module chimeric antigen receptor (5MCAR) designed to target and eliminate antigen-specific T cells[J]. Proc Natl Acad Sci USA, 2020, 117(46): 28950-28959.
TENSPOLDE M, ZIMMERMANN K, WEBER L C, et al. Regulatory T cells engineered with a novel insulin-specific chimeric antigen receptor as a candidate immunotherapy for type 1 diabetes[J]. J Autoimmun, 2019, 103: 102289.
RADICHEV I A, YOON J, SCOTT D W, et al. Towards antigen-specific Tregs for type 1 diabetes: construction and functional assessment of pancreatic endocrine marker, HPi2-based chimeric antigen receptor[J]. Cell Immunol, 2020, 358: 104224.
ELLEBRECHT C T, BHOJ V G, NACE A, et al. Reengineering chimeric antigen receptor T cells for targeted therapy of autoimmune disease[J]. Science, 2016, 353(6295): 179-184.
LEE J M, LUNDGREN D K, MAO X M, et al. Antigen-specific B cell depletion for precision therapy of mucosal pemphigus vulgaris[J]. J Clin Invest, 2020, 130(12): 6317-6324.
BLAT D, ZIGMOND E, ALTEBER Z, et al. Suppression of murine colitis and its associated cancer by carcinoembryonic antigen-specific regulatory T cells[J]. Mol Ther, 2014, 22(5): 1018-1028.
ELINAV E, WAKS T, ESHHAR Z. Redirection of regulatory T cells with predetermined specificity for the treatment of experimental colitis in mice[J]. Gastroenterology, 2008, 134(7): 2014-2024.
FRANSSON M, PIRAS E, BURMAN J, et al. CAR/FoxP3-engineered T regulatory cells target the CNS and suppress EAE upon intranasal delivery[J]. J Neuroinflammation, 2012, 9: 112.
DE PAULA POHL A, SCHMIDT A, ZHANG A H, et al. Engineered regulatory T cells expressing myelin-specific chimeric antigen receptors suppress EAE progression[J]. Cell Immunol, 2020, 358: 104222.
GUPTA S, SIMIC M, SAGAN S A, et al. CAR-T cell-mediated B-cell depletion in central nervous system autoimmunity[J]. Neurol Neuroimmunol Neuroinflamm, 2023, 10(2): e200080.
MITSDOERFFER M, DI LIBERTO G, DÖTSCH S, et al. Formation and immunomodulatory function of meningeal B cell aggregates in progressive CNS autoimmunity[J]. Brain, 2021, 144(6): 1697-1710.
MACDONALD K G, HOEPPLI R E, HUANG Q, et al. Alloantigen-specific regulatory T cells generated with a chimeric antigen receptor[J]. J Clin Invest, 2016, 126(4): 1413-1424.
LODKA D, ZSCHUMMEL M, BUNSE M, et al. CD19-targeting CAR T cells protect from ANCA-induced acute kidney injury[J]. Ann Rheum Dis, 2024, 83(4): 499-507.
OH S, MAO X M, MANFREDO-VIEIRA S, et al. Precision targeting of autoantigen-specific B cells in muscle-specific tyrosine kinase myasthenia gravis with chimeric autoantibody receptor T cells[J]. Nat Biotechnol, 2023, 41(9): 1229-1238.
REINCKE S M, VON WARDENBURG N, HOMEYER M A, et al. Chimeric autoantibody receptor T cells deplete NMDA receptor-specific B cells[J]. Cell, 2023, 186(23): 5084-5097.e18.
WANG D D, WANG X B, TAN B H, et al. Allogeneic CD19-targeted CAR-T therapy in refractory systemic lupus erythematosus achieved durable remission[J]. Med, 2025: 100749.
WANG W J, HE S Z, ZHANG W L, et al. BCMA-CD19 compound CAR T cells for systemic lupus erythematosus: a phase 1 open-label clinical trial[J]. Ann Rheum Dis, 2024, 83(10): 1304-1314.
BERGMANN C, MÜLLER F, DISTLER J H W, et al. Treatment of a patient with severe systemic sclerosis (SSc) using CD19-targeted CAR T cells[J]. Ann Rheum Dis, 2023, 82(8): 1117-1120.
MÜLLER F, TAUBMANN J, BUCCI L, et al. CD19 CAR T-cell therapy in autoimmune disease: a case series with follow-up[J]. N Engl J Med, 2024, 390(8): 687-700.
MERKT W, FREITAG M, CLAUS M, et al. Third-generation CD19.CAR-T cell-containing combination therapy in Scl70+ systemic sclerosis[J]. Ann Rheum Dis, 2024, 83(4): 543-546.
WANG X B, WU X, TAN B H, et al. Allogeneic CD19-targeted CAR-T therapy in patients with severe myositis and systemic sclerosis[J]. Cell, 2024, 187(18): 4890-4904.e9.
FISCHBACH F, RICHTER J, PFEFFER L K, et al. CD19-targeted chimeric antigen receptor T cell therapy in two patients with multiple sclerosis[J]. Med, 2024, 5(6): 550-558.e2.
QIN C, TIAN D S, ZHOU L Q, et al. Anti-BCMA CAR T-cell therapy CT103A in relapsed or refractory AQP4-IgG seropositive neuromyelitis optica spectrum disorders: phase 1 trial interim results[J]. Signal Transduct Target Ther, 2023, 8(1): 5.
MOTTE J, SGODZAI M, SCHNEIDER-GOLD C, et al. Treatment of concomitant myasthenia gravis and Lambert-Eaton myasthenic syndrome with autologous CD19-targeted CAR T cells[J]. Neuron, 2024, 112(11): 1757-1763.e2.
JHAVERI K S, SCHLAM I, HOLTZMAN N G, et al. Safety and efficacy of CAR T cells in a patient with lymphoma and a coexisting autoimmune neuropathy[J]. Blood Adv, 2020, 4(23): 6019-6022.
QI Y, ZHAO M, HU Y, et al. Efficacy and safety of CD19-specific CAR T cell-based therapy in B-cell acute lymphoblastic leukemia patients with CNSL[J]. Blood, 2022, 139(23): 3376-3386.
WANG X, QI Y K, LI H J, et al. Impact of glucocorticoids on short-term and long-term outcomes in patients with relapsed/refractory multiple myeloma treated with CAR-T therapy[J]. Front Immunol, 2022, 13: 943004.
HUARTE E, O'CONNOR R S, PEEL M T, et al. Itacitinib (INCB039110), a JAK1 inhibitor, reduces cytokines associated with cytokine release syndrome induced by CAR T-cell therapy[J]. Clin Cancer Res, 2020, 26(23): 6299-6309.
MESTERMANN K, GIAVRIDIS T, WEBER J, et al. The tyrosine kinase inhibitor dasatinib acts as a pharmacologic on/off switch for CAR T cells[J]. Sci Transl Med, 2019, 11(499): eaau5907.
MORRIS E C, NEELAPU S S, GIAVRIDIS T, et al. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy[J]. Nat Rev Immunol, 2022, 22(2): 85-96.
HAROON A, MUHSEN I N, ABID M B, et al. Infectious complications and preventative strategies following chimeric antigen receptor T-cells (CAR-T cells) therapy for B-cell malignancies[J]. Hematol Oncol Stem Cell Ther, 2022, 15(3): 153-158.
ABRAMSON J S, LIA PALOMBA M, GORDON L I, et al. Lisocabtagene maraleucel for patients with relapsed or refractory large B-cell lymphomas (TRANSCEND NHL 001): a multicentre seamless design study[J]. Lancet, 2020, 396(10254): 839-852.
HILL J A, GIRALT S, TORGERSON T R, et al. CAR-T: and a side order of IgG, to go?—Immunoglobulin replacement in patients receiving CAR-T cell therapy[J]. Blood Rev, 2019, 38: 100596.
MAHMOUDJAFARI Z, HAWKS K G, HSIEH A A, et al. American society for blood and marrow transplantation pharmacy special interest group survey on chimeric antigen receptor T cell therapy administrative, logistic, and toxicity management practices in the United States[J]. Biol Blood Marrow Transplant, 2019, 25(1): 26-33.
FLUGEL C L, MAJZNER R G, KRENCIUTE G, et al. Overcoming on-target, off-tumour toxicity of CAR T cell therapy for solid tumours[J]. Nat Rev Clin Oncol, 2023, 20(1): 49-62.
HUDECEK M, SOMMERMEYER D, KOSASIH P L, et al. The nonsignaling extracellular spacer domain of chimeric antigen receptors is decisive for in vivo antitumor activity[J]. Cancer Immunol Res, 2015, 3(2): 125-135.
SUN C, MAHENDRAVADA A, BALLARD B, et al. Safety and efficacy of targeting CD138 with a chimeric antigen receptor for the treatment of multiple myeloma[J]. Oncotarget, 2019, 10(24): 2369-2383.
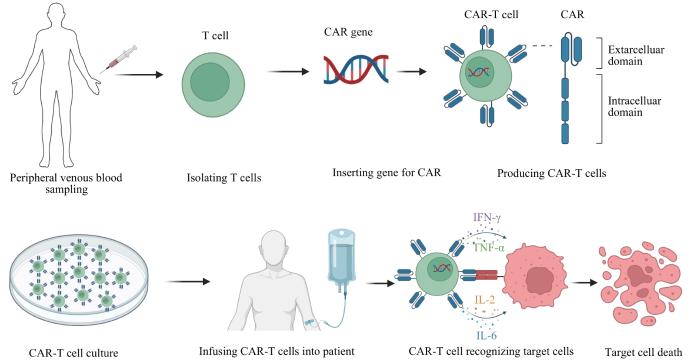
... 嵌合抗原受体T细胞(chimeric antigen receptor T cell,CAR-T细胞)治疗通过改造T细胞使其表达嵌合抗原受体(chimeric antigen receptor,CAR),以主要组织相容性复合体非依赖的方式发挥靶向毒性.目前该疗法主要应用于复发难治性白血病、淋巴瘤和多发性骨髓瘤等疾病[4-6],展现出持续应答及具有治愈性的优势,对实体瘤亦具初步疗效[7].近年来,CAR-T细胞治疗已被引入多种AID中,在临床前和临床试验中均取得显著成效.与现有疗法相比,CAR-T细胞诱导循环自身反应性B细胞的快速耗竭及在体内持续扩增的能力使其在治疗AID中更有前景. ...
0
1
... 嵌合抗原受体T细胞(chimeric antigen receptor T cell,CAR-T细胞)治疗通过改造T细胞使其表达嵌合抗原受体(chimeric antigen receptor,CAR),以主要组织相容性复合体非依赖的方式发挥靶向毒性.目前该疗法主要应用于复发难治性白血病、淋巴瘤和多发性骨髓瘤等疾病[4-6],展现出持续应答及具有治愈性的优势,对实体瘤亦具初步疗效[7].近年来,CAR-T细胞治疗已被引入多种AID中,在临床前和临床试验中均取得显著成效.与现有疗法相比,CAR-T细胞诱导循环自身反应性B细胞的快速耗竭及在体内持续扩增的能力使其在治疗AID中更有前景. ...
1
... 嵌合抗原受体T细胞(chimeric antigen receptor T cell,CAR-T细胞)治疗通过改造T细胞使其表达嵌合抗原受体(chimeric antigen receptor,CAR),以主要组织相容性复合体非依赖的方式发挥靶向毒性.目前该疗法主要应用于复发难治性白血病、淋巴瘤和多发性骨髓瘤等疾病[4-6],展现出持续应答及具有治愈性的优势,对实体瘤亦具初步疗效[7].近年来,CAR-T细胞治疗已被引入多种AID中,在临床前和临床试验中均取得显著成效.与现有疗法相比,CAR-T细胞诱导循环自身反应性B细胞的快速耗竭及在体内持续扩增的能力使其在治疗AID中更有前景. ...
1
... 当前CAR的结构经历了5代变化(图1).一代CAR-T细胞胞内结构域包含CD3ζ链,但由于缺少共刺激结构域,其扩增能力和持久性欠佳、抗癌活性不足.二代CAR-T细胞在一代基础上增加了1个共刺激结构域(CD28、4-1BB或OXO40等),增殖能力、持久性和细胞毒性均显著提高.三代CAR-T细胞包含2种共刺激结构域以进一步增强其信号激活、靶向毒性并延长增殖,但由于其活性增加且不可控,可能导致细胞因子风暴、多器官衰竭甚至死亡等严重不良反应,临床上与二代CAR-T细胞相比不具优势[8-10].四代CAR-T细胞添加白细胞介素-2(interleukin-2,IL-12)等免疫调节因子以激活先天性免疫细胞并增强T细胞活化,一定程度上克服肿瘤微环境中的免疫抑制因素,更有力地攻击实体肿瘤.五代CAR-T细胞涉及对传统CAR结构进行改造,如添加IL-2受体β链触发细胞因子Janus激酶-信号转导与转录激活因子3/5(Janus kinase-signal transducer and activator of transcription 3/5,JAK-STAT3/5)信号转导以增强CAR-T细胞活性[11],以及使用CRISPR-Cas9技术敲除T细胞中的人类白细胞抗原Ⅰ类分子(human leukocyte antigen class Ⅰ,HLA-Ⅰ)和内源性T细胞受体制备通用型CAR-T细胞,降低CAR-T细胞被排斥和GVHD的风险[12]. ...
0
1
... 当前CAR的结构经历了5代变化(图1).一代CAR-T细胞胞内结构域包含CD3ζ链,但由于缺少共刺激结构域,其扩增能力和持久性欠佳、抗癌活性不足.二代CAR-T细胞在一代基础上增加了1个共刺激结构域(CD28、4-1BB或OXO40等),增殖能力、持久性和细胞毒性均显著提高.三代CAR-T细胞包含2种共刺激结构域以进一步增强其信号激活、靶向毒性并延长增殖,但由于其活性增加且不可控,可能导致细胞因子风暴、多器官衰竭甚至死亡等严重不良反应,临床上与二代CAR-T细胞相比不具优势[8-10].四代CAR-T细胞添加白细胞介素-2(interleukin-2,IL-12)等免疫调节因子以激活先天性免疫细胞并增强T细胞活化,一定程度上克服肿瘤微环境中的免疫抑制因素,更有力地攻击实体肿瘤.五代CAR-T细胞涉及对传统CAR结构进行改造,如添加IL-2受体β链触发细胞因子Janus激酶-信号转导与转录激活因子3/5(Janus kinase-signal transducer and activator of transcription 3/5,JAK-STAT3/5)信号转导以增强CAR-T细胞活性[11],以及使用CRISPR-Cas9技术敲除T细胞中的人类白细胞抗原Ⅰ类分子(human leukocyte antigen class Ⅰ,HLA-Ⅰ)和内源性T细胞受体制备通用型CAR-T细胞,降低CAR-T细胞被排斥和GVHD的风险[12]. ...
1
... 当前CAR的结构经历了5代变化(图1).一代CAR-T细胞胞内结构域包含CD3ζ链,但由于缺少共刺激结构域,其扩增能力和持久性欠佳、抗癌活性不足.二代CAR-T细胞在一代基础上增加了1个共刺激结构域(CD28、4-1BB或OXO40等),增殖能力、持久性和细胞毒性均显著提高.三代CAR-T细胞包含2种共刺激结构域以进一步增强其信号激活、靶向毒性并延长增殖,但由于其活性增加且不可控,可能导致细胞因子风暴、多器官衰竭甚至死亡等严重不良反应,临床上与二代CAR-T细胞相比不具优势[8-10].四代CAR-T细胞添加白细胞介素-2(interleukin-2,IL-12)等免疫调节因子以激活先天性免疫细胞并增强T细胞活化,一定程度上克服肿瘤微环境中的免疫抑制因素,更有力地攻击实体肿瘤.五代CAR-T细胞涉及对传统CAR结构进行改造,如添加IL-2受体β链触发细胞因子Janus激酶-信号转导与转录激活因子3/5(Janus kinase-signal transducer and activator of transcription 3/5,JAK-STAT3/5)信号转导以增强CAR-T细胞活性[11],以及使用CRISPR-Cas9技术敲除T细胞中的人类白细胞抗原Ⅰ类分子(human leukocyte antigen class Ⅰ,HLA-Ⅰ)和内源性T细胞受体制备通用型CAR-T细胞,降低CAR-T细胞被排斥和GVHD的风险[12]. ...
1
... 当前CAR的结构经历了5代变化(图1).一代CAR-T细胞胞内结构域包含CD3ζ链,但由于缺少共刺激结构域,其扩增能力和持久性欠佳、抗癌活性不足.二代CAR-T细胞在一代基础上增加了1个共刺激结构域(CD28、4-1BB或OXO40等),增殖能力、持久性和细胞毒性均显著提高.三代CAR-T细胞包含2种共刺激结构域以进一步增强其信号激活、靶向毒性并延长增殖,但由于其活性增加且不可控,可能导致细胞因子风暴、多器官衰竭甚至死亡等严重不良反应,临床上与二代CAR-T细胞相比不具优势[8-10].四代CAR-T细胞添加白细胞介素-2(interleukin-2,IL-12)等免疫调节因子以激活先天性免疫细胞并增强T细胞活化,一定程度上克服肿瘤微环境中的免疫抑制因素,更有力地攻击实体肿瘤.五代CAR-T细胞涉及对传统CAR结构进行改造,如添加IL-2受体β链触发细胞因子Janus激酶-信号转导与转录激活因子3/5(Janus kinase-signal transducer and activator of transcription 3/5,JAK-STAT3/5)信号转导以增强CAR-T细胞活性[11],以及使用CRISPR-Cas9技术敲除T细胞中的人类白细胞抗原Ⅰ类分子(human leukocyte antigen class Ⅰ,HLA-Ⅰ)和内源性T细胞受体制备通用型CAR-T细胞,降低CAR-T细胞被排斥和GVHD的风险[12]. ...



{kind=link}
{kind=link}
{kind=link}
{kind=link}