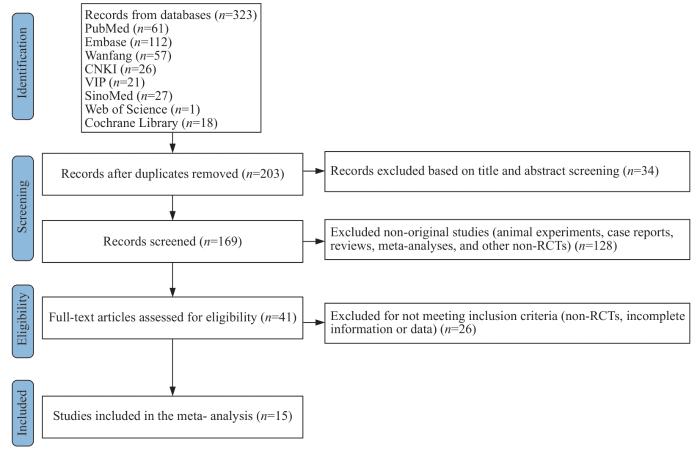
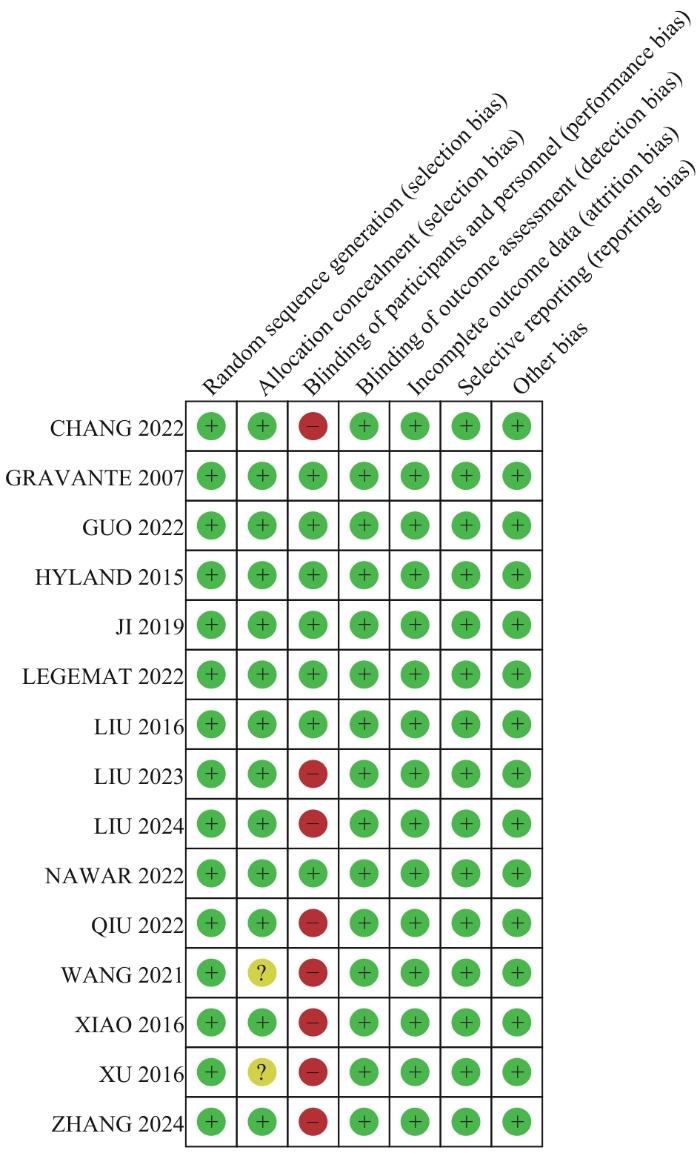
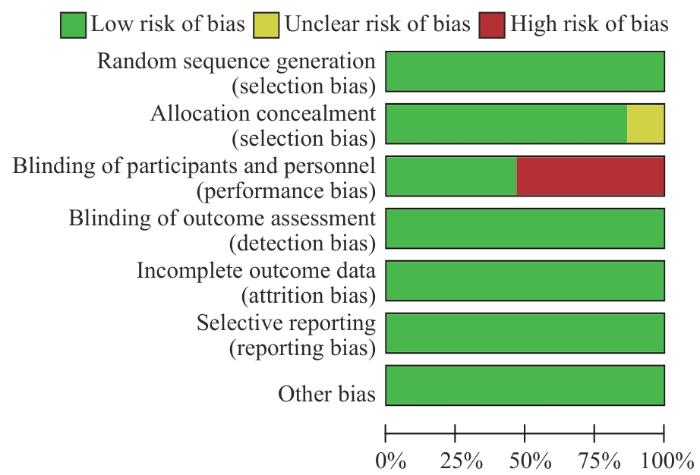
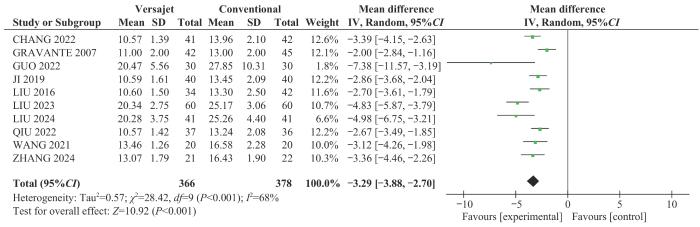
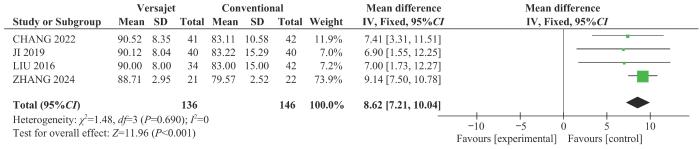
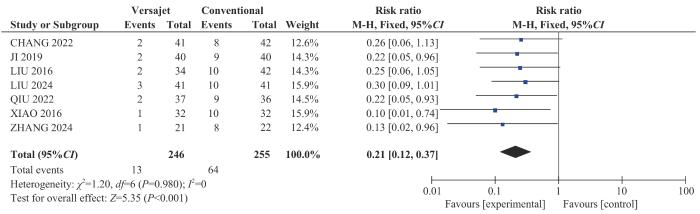
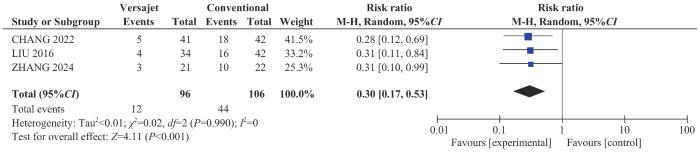
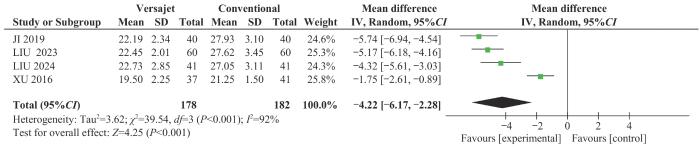
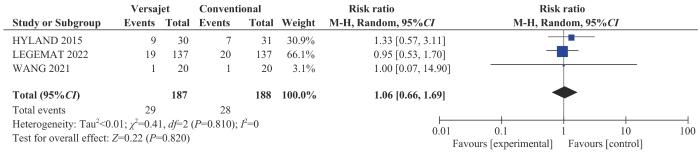
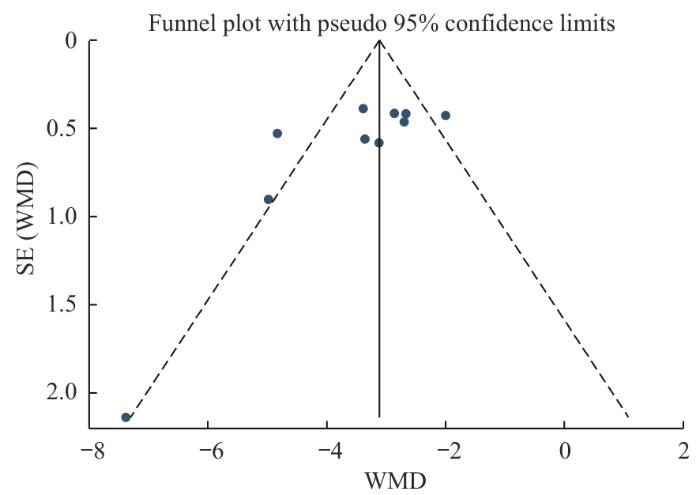
Objective ·To compare the effectiveness of hydrodynamic debridement versus conventional debridement in the treatment of burn wounds through a systematic review, focusing on differences in time to complete healing after graft, time to debride a 1% total body surface area (TBSA) wound, hospitalization duration, skin graft survival rate at 7 d post-surgery, secondary debridement rate, and positive rate of bacterial culture of wound exudate at 3 d post-surgery, aiming to select a more effective debridement method for burn wounds requiring debridement. Methods ·A systematic literature search was conducted in PubMed, Embase, Web of Science, Cochrane Library, CNKI, SinoMed, China Science and Technology Journal Database,and Wanfang Database, for studies comparing hydrodynamic debridement and conventional debridement in the treatment of burns. The search included articles published in Chinese and English, and the search period was from the inception of the databases to October 1, 2024. The study type was randomized controlled trials (RCTs). After literature search and screening, the included studies was evaluated for quality, and relevant data were extracted. Qualitative variables were presented as relative risk (RR), and quantitative variables as mean difference (MD). Forest plots were created by using RevMan 5.4 software with fixed- or random- effects models. Funnel plots were generated and Egger's test was performed by using Stata 14.0 software. Results ·Fifteen high-quality RCTs were included in this study, involving 1 261 patients with burn injuries requiring debridement. The analysis results showed that compared to the conventional debridement group, the hydrodynamic debridement group had significantly shorter time to complete healing after graft (MD=-3.29,95%CI -3.88‒-2.70, P<0.001), shorter time required to debride a 1% TBSA wound (MD=-0.63, 95%CI -0.76‒-0.50, P<0.001), and reduced hospitalization duration (MD=-4.22, 95%CI -6.17‒-2.28, P<0.001). The skin graft survival rate at 7 d post-surgery in the hydrodynamic debridement group (MD=8.62, 95%CI 7.21‒10.04, P<0.001) was significantly higher, while the secondary debridement rate (RR=0.21, 95%CI 0.12‒0.37, P<0.001) and the positive rate of bacterial culture of wound exudate at 3 d post-surgery (RR=0.30, 95%CI 0.17‒0.53, P<0.001) were significantly lower compared with the conventional debridement group. There was no statistically significant difference in the postoperative infections rates between the two groups (RR=1.06, 95%CI 0.66‒1.69, P=0.820). Conclusion ·In the treatment of burn wounds, hydrodynamic debridement outperforms traditional debridement. In the management of burn wounds, hydrodynamic debridement outperforms conventional debridement by shortening debridement and hospitalization durations, reducing the need for secondary debridement, decreasing early bacterial colonization, and improving skin graft survival. In terms of postoperative infection risk, no significant difference was observed between the two methods, indicating comparable safety profiles.
ZHAO Jianlei, ZHAO Jingqi, LIU Chang, HUANG Jingjun, JIN Shengyuan. Efficacy of hydrodynamic debridement in the treatment of burns: a systematic review of randomized controlled trials. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2025, 45(5): 614-623 doi:10.3969/j.issn.1674-8115.2025.05.010
① 研究对象为需要清创的烧伤患者,伴有不同程度的创面感染,无其他损伤或基础疾病,不限种族、性别和年龄。② 使用水动力清创系统作为清创工具,使用常规手术器械作为清创工具。③ 结果指标包括创面愈合时间、每1%总体表面积(total body surface area,TBSA)创面的清创时间、术后7 d植皮存活率、二次清创率、术后3 d创面分泌物细菌培养阳性率、住院时间、术后感染发生率。④ 研究类型为RCT。
1.1.2 文献排除标准
① 病例对照试验。② 基础研究。③ 综述类或meta分析类文献。④ 研究内容与水动力治疗烧伤治疗无关的文献。⑤ 未提供所需数据(包括样本量大小、均值、标准差、事件发生例数等)的文献。⑥ 写作语言非中文、非英文。⑦ 无法获取全文的文献。
1.2 检索策略
使用计算机检索PubMed、Embase、Web of Science、Cochrane Library、中国知网(CNKI)、中国生物医学文献服务系统(SinoMed)、维普中文期刊数据库(VIP)及万方数据库。检索方式为主题词加自由词组合。中文检索词包括:“烧伤”“水刀(即水动力清创系统)”“水动力清创”。英文检索词包括:“burn”“hydrosurgery”“hydrodebridement”“hyderscalpels”“water jet surgery”“Versajet”等。检索时限为建库至2024年10月1日。
1.3 数据提取
符合纳入标准的文献由2名具有系统评价研究经验的研究生独立进行全文审阅,并交叉核对所提取的研究特征及结局指标数据。所有研究者均接受过PRISMA(Preferred reporting items for systematic reviews and meta-analyses)声明及Cochrane系统评价方法学培训。针对数据提取过程中出现的分歧,2名研究者通过讨论达成共识,必要时交给第三位研究者进行仲裁。
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate.
/Authors' Contributions:ZHAO Jianlei was responsible for the conception and design of the study, as well as the writing of the manuscript. LIU Chang and ZHAO Jingqi participated in data collection, organization, and statistical processing. JIN Shengyuan and HUANG Jingjun were involved in the revision and review of the article. All authors have read the final version of of paper and consented to its submission.
RADZIKOWSKA-BÜCHNER E, ŁOPUSZYŃSKA I, FLIEGER W, et al. An overview of recent developments in the management of burn injuries[J]. Int J Mol Sci, 2023, 24(22): 16357.
LEGEMATE C M, GOEI H, GOSTELIE O E, et al. Application of hydrosurgery for burn wound debridement: an 8-year cohort analysis[J]. Burns, 2019, 45(1): 88-96.
KAKAGIA D D, KARADIMAS E J. The efficacy of VersajetTM hydrosurgery system in burn surgery. A systematic review[J]. J Burn Care Res, 2018, 39(2): 188-200.
PIEPTU V, MIHAI A, GROZA C, et al. Burns in the emergency department: a one-year single center analysis on 355 cases[J]. Chirurgia (Bucur), 2020, 115(4): 486-492.
LIU G C, KAN Z H, SHENG J J, et al. Efficacy of a hydrosurgery system applied in the debridement of extensive residual wounds of patients with severe burn[J]. Chinese Journal of Burns, 2016, 32(9): 549-554.
KAN Z H, LIU G C, ZHU S H. Application of hydrosurgery system in debridement of burn wound: an overview[J]. Academic Journal of Second Military Medical University, 2017, 38(4): 501-505.
JIANG Y, ZHOU P, LIU A Y, et al. Efficacy of hydrosurgical eschar excision following MEEK microskin grafting in patients with massive burns: a retrospective study of a single center[J]. Burns, 2024, 50(5): 1223-1231.
XU F R, QIAO L, LI X C, et al. Comparative study on the efficacy of water jet scalpel and tangential excision for debriding medium area deep second degree burn wounds[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2016, 36(3): 354-358.
FUENMAYOR P, GOTTENGER R, PUJADAS Z, et al. Successful rhinophyma treatment utilizing the versajet Ⅱ hydrosurgery system: a case report and systematic review of the literature[J]. Cureus, 2024, 16(7): e63921.
LEGEMATE C M, KWA K A A, GOEI H, et al. Hydrosurgical and conventional debridement of burns: randomized clinical trial[J]. Br J Surg, 2022, 109(4): 332-339.
GUO Y F, SONG X G, SONG G R, et al. Application of hydrosurgical debridement and autologous skin cell suspension in the treatment of electric arc injury[J]. Burns Open, 2022, 6(1): 19-22.
CAO Y L, LIU Z C, CHEN X L. Efficacy of hydrosurgical excision combined with skin grafting in the treatment of deep partial-thickness and full-thickness burns: a two-year retrospective study[J]. Burns, 2023, 49(5): 1087-1095.
TANG X D, QIU L, WANG F, et al. Safety and efficacy of waterjet debridement vs. conventional debridement in the treatment of extremely severe burns: a retrospective analysis[J]. Burns, 2023, 49(8): 1926-1934.
GHOGOMU E A T, MAXWELL L J, BUCHBINDER R, et al. Updated method guidelines for cochrane musculoskeletal group systematic reviews and metaanalyses[J]. J Rheumatol, 2014, 41(2): 194-205.
LIU C, JIN C H, LUO Y L, et al. Meta-analysis of the efficacy and safety of verapamil and triamcinolone acetonide in the treatment of pathological scar[J]. The Chinese Journal of Dermatovenereology, 2024, 38(1): 50-58.
YIN X X, SHEN T Q, QIN S, et al. Comparison of the safety of remazolam and propofol for pain-free gastroscopy in elderly patients: a meta-analysis[J]. Journal of Clinical Anesthesiology, 2024, 40(4): 393-400.
XIAO H T, TIAN S M, WEI Y, et al. Efficacy and safety of VERSAJET Ⅱ hydrosurgery system in the treatment of deep partial-thickness burn wounds[J]. Clinical Medicine, 2016, 36(11): 78-79.
LIU L P, DENG T, ZHU P. Comparison of clinical effects between scab removal and debridement and water knife debridement treatment for moderate area deep Ⅱ degree burn wounds[J]. Medical Innovation of China, 2024, 21(15): 131-135.
CHANG L. Application effects of hydrodynamic debridement system in wound debridement of burn patients[J]. Medical Journal of Chinese People's Health, 2022, 34(24): 44-47.
张彩云. 水动力清创系统在大面积烧伤残余创面治疗中的临床疗效观察[D]. 石家庄: 河北医科大学, 2024.ZHANG. Clinical efficacy observation of hydrosurgery system in the treatment of residual wounds with extensive burns[D]. Shijiazhuang: Hebei Medical University, 2024.
WANG F. Efficacy study of hydrosurgery debridement combined with punch graft skin transplantation in the treatment of large area burn residual wounds[J]. Chinese Journal of Trauma and Disability Medicine, 2021, 29(1): 44-46.
LIU S Y, ZHAO Y H, LIU T C, et al. Comparative study on the effectiveness of water knife vs. scab debridement for medium area deep Ⅱ degree burn wounds[J]. Chinese Journal of Experimental Surgery, 2023, 40(5): 916.
JI J H, FANG H, QIAN L K, et al. Clinical efficacy of negative pressure wound therapy combined with hydrosurgery debridement in the treatment of deep burns[J]. Clinical Journal of Medical Officers, 2019, 47(12): 1381-1382, 1384.
NAWAR A, NOUH O M, SAAD A S, et al. Versajet™ versus knife excision for burn wound preparation: a randomized controlled trial[J]. Eur J Plast Surg, 2022, 45(5): 793-798.
WANG L, CAI Y H, HU K S, et al. Retrospective study on the clinical effect of hydrosurgery system in the treatment of deep partial-thickness burn wound[J]. Chinese Journal of Injury Repair and Wound Healing (Electronic Edition), 2021, 16(3): 245-250
KWA K A, GOEI H, BREEDERVELD R S, et al. A systematic review on surgical and nonsurgical debridement techniques of burn wounds[J]. J Plast Reconstr Aesthet Surg, 2019, 72(11): 1752-1762.
HIHARA M, TAKEGAWA M, KAKUDO N, et al. A stylized two-stage debridement strategy using an electric dermatome and a Versajet™ hydrosurgery system for deep axillary burns[J]. J Surg Case Rep, 2022, 2022(10): rjac481.
XIANG J, WU H. Effect of hydrodynamic debridement system on residual wound healing and inflammatory factors in large area burns[J]. Chinese Journal of Aesthetic Medicine, 2021, 30(10): 25-28.
WANG Z J, PENG L L, PAN S F, et al. Application of a novel eschar cutter in early treatment of deep second degree burn wounds[J]. Zhejiang Medical Journal, 2022, 44(2): 154-157, 228-229.
PUTZER D, LECHNER R, CORACA-HUBER D, et al. The extent of environmental and body contamination through aerosols by hydro-surgical debridement in the lumbar spine[J]. Arch Orthop Trauma Surg, 2017, 137(6): 743-747.
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Meta-analysis results after altering the effect modelTab 3
Outcome
Number of studies/n
Fixed-effects model
Random-effects model
MD/RR (95%CI)
P value
MD/RR (95%CI)
P value
Time to complete healing after graft
10
-3.11 (-3.43, -2.80)
<0.001
-3.29 (-3.88, -2.70)
<0.001
Time to debride 1% TBSA wound
7
-0.65 (-0.71, -0.58)
<0.001
-0.63 (-0.76, -0.50)
<0.001
Percentage of skin graft survival
4
8.62 (7.21, 10.04)
<0.001
8.62 (7.21, 10.04)
<0.001
Secondary debridement rate
7
0.21 (0.12, 0.37)
<0.001
0.22 (0.12, 0.39)
<0.001
Positive rate of bacterial culture of wound exudate at 3 d post-surgery
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Meta-analysis results after altering the effect modelTab 3
Outcome
Number of studies/n
Fixed-effects model
Random-effects model
MD/RR (95%CI)
P value
MD/RR (95%CI)
P value
Time to complete healing after graft
10
-3.11 (-3.43, -2.80)
<0.001
-3.29 (-3.88, -2.70)
<0.001
Time to debride 1% TBSA wound
7
-0.65 (-0.71, -0.58)
<0.001
-0.63 (-0.76, -0.50)
<0.001
Percentage of skin graft survival
4
8.62 (7.21, 10.04)
<0.001
8.62 (7.21, 10.04)
<0.001
Secondary debridement rate
7
0.21 (0.12, 0.37)
<0.001
0.22 (0.12, 0.39)
<0.001
Positive rate of bacterial culture of wound exudate at 3 d post-surgery
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
1
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
1
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
1
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
1
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...
5
... Basic characteristics of the included studies on hydrosurgery debridement and conventional debridementTab 1
Study
Study design
Hydrosurgery debridement group
Conventional debridement group
Outcome
n
Age/year
TBSA/%
n
Age/year
TBSA/%
NAWAR et al, 2022[29]
RCT
20
21.20±11.10
23.30±8.30
20
19.00±9.20
24.50±9.60
②
LEGEMAT et al, 2022[13]
RCT
137
42.89±25.47
8.41±7.49
137
42.89±25.47
8.41±7.49
⑦
HYLAND et al, 2015[14]
RCT
30
‒
‒
31
‒
‒
⑦
GRAVANTE et al, 2007[16]
RCT
42
46.00±26.90
25.00±14.00
45
50.00±28.40
23.00±16.00
①
GUO et al, 2022[15]
RCT
30
‒
‒
30
‒
‒
①
CHANG, 2022[24]
RCT
41
40.32±10.66
‒
42
40.56±10.72
‒
①②③④⑤
JI et al, 2019[28]
RCT
40
44.23±6.23
19.38±5.68
40
44.28±6.24
18.75±6.05
①②③④⑤⑥
LIU et al, 2016[7]
RCT
34
41.00±12.00
73.00±11.00
42
40.00±12.00
74.00±12.00
①②③④⑤
LIU et al, 2024[23]
RCT
41
41.15±6.82
23.06±2.12
41
41.93±6.50
22.78±2.35
①②④⑥
LIU et al, 2023[27]
RCT
60
‒
‒
60
‒
‒
①⑥
QIU et al, 2022[6]
RCT
37
42.93±1.91
52.37±5.79
36
42.91±1.94
52.33±5.81
①②④
WANG, 2021[26]
RCT
20
45.67±2.11
65.21±0.51
20
45.25±2.46
65.25±0.56
①⑦
XIAO et al, 2016[22]
RCT
32
27.10±6.80
‒
32
28.00±7.40
‒
④
XU et al, 2016[11]
RCT
37
44.00±27.00
37.00±14.00
41
50.00±19.00
34.00±16.00
⑥
ZHANG, 2024[25]
RCT
21
44.57±7.70
66.86±9.64
22
43.59±9.89
67.18±8.61
①②③④⑤
Note: ① Time to complete healing after graft; ② Time to debride 1% TBSA wound; ③ Percentage of skin graft survival; ④ Secondary debridement rate; ⑤ Positive rate of bacterial culture of wound exudate at 3 d post-surgery; ⑥ Hospitalization duration; ⑦ Postoperative infection rate. ...




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}