上海交通大学学报(医学版) ›› 2022, Vol. 42 ›› Issue (8): 1053-1061.doi: 10.3969/j.issn.1674-8115.2022.08.010
• 论著 · 临床研究 • 上一篇
韩婷1( ), 吕纯鑫2(), 卓萌1(), 夏青1, 刘腾飞1, 吴秀奇1, 林晓琳1(), 肖秀英1()
), 吕纯鑫2(), 卓萌1(), 夏青1, 刘腾飞1, 吴秀奇1, 林晓琳1(), 肖秀英1()
收稿日期:2022-03-11
接受日期:2022-07-03
出版日期:2022-08-12
发布日期:2022-08-12
通讯作者:
林晓琳,肖秀英
E-mail:yyhanwh@163.com;chunxin@fudan.edu.cn;doc.zhuo6@163.com;renjilxl@163.com;xiaoxiuying2002@163.com
作者简介:韩 婷(1988—),女,住院医师,博士;电子信箱:yyhanwh@163.com基金资助:
HAN Ting1(), LÜ Chunxin2(), ZHUO Meng1(), XIA Qing1, LIU Tengfei1, WU Xiuqi1, LIN Xiaolin1(), XIAO Xiuying1()
Received:2022-03-11
Accepted:2022-07-03
Online:2022-08-12
Published:2022-08-12
Contact:
LIN Xiaolin,XIAO Xiuying
E-mail:yyhanwh@163.com;chunxin@fudan.edu.cn;doc.zhuo6@163.com;renjilxl@163.com;xiaoxiuying2002@163.com
Supported by:摘要:
目的·探索应用程序性死亡蛋白-1(programmed death-1,PD-1)抑制剂行免疫治疗的进展期胃癌患者的免疫相关不良反应(immune-related adverse events,irAEs)的特征及预测因素,并分析irAEs与患者预后的相关性。方法·选择2018年6月—2021年10月于上海交通大学医学院附属仁济医院应用PD-1抑制剂治疗的进展期胃癌患者140例。根据患者有无irAEs发生,将其分为irAEs组和非irAEs组。收集并分析2组患者的临床特征、irAEs的表现及预后情况。采用多因素Logistic回归模型分析影响irAEs发生的相关因素,并建立irAEs的预测模型。运用受试者操作特征曲线(receiver operating characteristic curve,ROC curve,ROC曲线)对不同指标预测irAEs发生的能力进行评估。采用Kaplan-Meier生存曲线分析irAEs与预后的相关性。运用Cox比例风险模型分析影响患者预后的相关因素。结果·共计132例患者完成随访,其中有63例(47.7%)患者发生irAEs。比较2组患者的临床特征的结果显示,年龄≥65岁、Ki-67指数、白细胞计数、中性粒细胞计数、调节性T细胞(regulatory T cell,Treg)计数的组间差异具有统计学意义(均P<0.05)。多因素Logistic回归分析显示,Treg计数为影响irAEs发生的保护因素(P=0.030)。ROC曲线提示,Treg+Ki-67+年龄(≥65岁)联合指标可较好地预测irAEs的发生(AUC=0.753,95% CI 0.623~0.848,P=0.000)。Kaplan-Meier生存曲线的结果显示,irAEs组患者的无进展生存期(progression-free survival,PFS)较非irAEs组有所延长(P=0.001)。Cox比例风险回归分析提示,irAEs是患者PFS的独立影响因素(P=0.006)。结论·Treg计数是行PD-1抑制剂免疫治疗的进展期胃癌患者发生irAEs的独立影响因素,且irAEs的发生可延长患者的PFS;Treg+Ki-67+年龄(≥65岁)联合指标可对该不良反应的发生进行较好的预测。
中图分类号:
韩婷, 吕纯鑫, 卓萌, 夏青, 刘腾飞, 吴秀奇, 林晓琳, 肖秀英. 进展期胃癌免疫治疗不良反应的相关因素及预后分析[J]. 上海交通大学学报(医学版), 2022, 42(8): 1053-1061.
HAN Ting, LÜ Chunxin, ZHUO Meng, XIA Qing, LIU Tengfei, WU Xiuqi, LIN Xiaolin, XIAO Xiuying. Related factors and prognostic analysis of adverse events of immunotherapy in advanced gastric cancer[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(8): 1053-1061.
| Clinical characteristic | irAEs group (n=63) | Non-irAEs group (n=69) | P value |
|---|---|---|---|
| Age≥65 years/n | 22 | 37 | 0.030 |
| Gender (male/female)/n | 43/20 | 46/23 | 0.847 |
| Treatment line (first line/posterior line)/n | 46/17 | 40/29 | 0.071 |
| TNM staging (Ⅲ/Ⅳ)/n | 6/57 | 4/65 | 0.421 |
| Ki-67 index/% | 49.4±23.3 | 58.9±20.8 | 0.049 |
| Her-2 expression (positive/negative)/n | 9/54 | 11/58 | 0.791 |
| PD-1/PD-L1 expression (positive/negative)/n | 22/21 | 16/17 | 0.818 |
| MMR (pMMR/dMMR)/n | 28/2 | 32/4 | 0.535 |
| Tumor marker | |||
| AFP/(ng·mL-1) | 3.3 (2.1, 7.0) | 3.3 (2.5, 4.7) | 0.209 |
| CEA/(ng·mL-1) | 6.0 (2.5, 68.5) | 6.3 (2.3, 21.7) | 0.280 |
| CA19-9/(U·mL-1) | 20.6 (8.4, 122.9) | 30.0 (9.9, 301.0) | 0.254 |
| CA125/(U·mL-1) | 31.1 (13.3, 143.5) | 23.3 (10.6, 114.0) | 0.116 |
| CA153/(U·mL-1) | 12.8 (9.4, 21.2) | 10.9 (7.4, 15.8) | 0.165 |
| CA724/(U·mL-1) | 5.7 (2.1, 49.7) | 9.1 (4.7, 48.0) | 0.549 |
| CYFRA21-1/(ng·mL-1) | 5.1 (2.6, 12.4) | 6.7 (3.5, 9.6) | 0.648 |
| CA50/(U·mL-1) | 17.6 (5.2, 115.6) | 24.6 (6.4, 191.6) | 0.153 |
| CA242/(U·mL-1) | 6.4 (3.0, 16.4) | 9.9 (4.4, 96.3) | 0.262 |
| SCC/(ng·mL-1) | 1.0 (0.8, 1.7) | 1.2 (0.8, 1.5) | 0.933 |
| NSE/(ng·mL-1) | 11.4 (9.4, 14.6) | 11.5 (9.3, 15.3) | 0.693 |
| PSA/(ng·mL-1) | 0.7 (0.5, 1.5) | 0.8 (0.5, 1.6) | 0.712 |
| Endocrine indicator | |||
| Sex hormone six | |||
| Neohombreol/(nmol·L-1) | 7.8 (1.2, 12.0) | 8.5 (1.2, 13.6) | 0.942 |
| Progestin/(nmol·L-1) | 2.0 (0.9, 2.8) | 2.1 (1.4, 3.4) | 0.381 |
| Estradiol/(pmol·L-1) | 84.0 (55.1, 105.0) | 92.0 (72.3, 124.8) | 0.274 |
| Drosophila prolactin/(ng·mL-1) | 13.6 (9.7, 19.0) | 13.7 (9.2, 19.7) | 0.812 |
| Folkopoietin/(U·L-1) | 12.8 (7.4, 20.7) | 20.1 (8.1, 39.2) | 0.256 |
| Luteinizing hormone/(U·L-1) | 5.0 (2.8, 11.4) | 6.3 (4.5, 23.3) | 0.456 |
| Cortisol hormone/(nmol·L-1) | 369.5 (313.1, 456.5) | 414.5 (298.6, 465.4) | 0.668 |
| Somatotropic hormone/(ng·mL-1) | 1.5 (0.7, 2.0) | 0.8 (0.2, 2.4) | 0.647 |
| ACTH/(pg·mL-1) | 28.5 (23.5, 39.3) | 29.1 (21.3, 51.7) | 0.269 |
| Amylase/(U·L-1) | 83.5 (63.8, 99.3) | 63.5 (54.8, 75.2) | 0.058 |
| ANA (positive/negative)/n | 22/24 | 11/17 | 0.477 |
| Blood routine index | |||
| Leukocyte count/(×109·L-1) | 5.7 (4.4, 8.3) | 5.4 (4.1, 6.2) | 0.044 |
| Neutrophil count/(×109·L-1) | 3.8 (2.4, 5.4) | 3.3 (2.3, 4.0) | 0.039 |
| Monocyte count/(×109·L-1) | 0.5 (0.4, 0.6) | 0.5 (0.4, 0.7) | 0.656 |
| Lymphocyte count/(×109·L-1) | 1.4 (1.1, 1.6) | 1.3 (1.0, 1.6) | 0.634 |
| CRP/(mg·L-1) | 2.9 (0.5, 11.5) | 1.6 (0.5, 10.3) | 0.569 |
| Neutrophil count/lymphocyte count | 2.8 (2.0, 3.9) | 2.1 (1.6, 3.6) | 0.100 |
| Neutrophil count/CRP | 1.7 (0.4, 4.7) | 2.0 (0.4, 5.0) | 0.712 |
| Leukocyte count/CRP | 2.4 (0.5, 8.5) | 3.3 (0.6, 8.3) | 0.800 |
| Lynphocyte subsets | |||
| CD19/% | 6.5 (4.4, 10.9) | 6.8 (3.9, 9.8) | 0.527 |
| CD3/% | 69.9 (60.6, 76.4) | 67.9 (57.8, 72.8) | 0.175 |
| CD4/% | 37.8±9.1 | 36.1±11.9 | 0.384 |
| CD8/% | 26.1±8.9 | 24.7±10.0 | 0.404 |
| CD4/CD8 | 1.4 (1.1, 2.2) | 1.5 (1.2, 2.4) | 0.370 |
| CD56/% | 19.9 (12.9, 27.1) | 21.0 (14.1, 32.4) | 0.183 |
| Cytokine level | |||
| Treg count/% | 8.3±2.5 | 9.8±3.0 | 0.016 |
| IFN-α/(pg·mL-1) | 1.8 (1.2, 2.3) | 1.5 (0.9, 2.4) | 0.783 |
| IL-17/(pg·mL-1) | 6.0 (1.3, 9.4) | 3.5 (1.3, 10.0) | 0.666 |
| TNF-α/(pg·mL-1) | 1.8 (1.3, 2.5) | 1.6 (1.0, 3.0) | 0.806 |
| IL-2/(pg·mL-1) | 1.2 (0.8, 1.5) | 1.2 (0.8, 1.8) | 0.240 |
| IL-4/(pg·mL-1) | 1.8 (1.0, 3.0) | 1.6 (0.9, 2.5) | 0.349 |
| IL-6/(pg·mL-1) | 8.1 (4.4, 16.2) | 6.9 (3.8, 12.2) | 0.083 |
| IL-8/(pg·mL-1) | 46.6 (22.4, 67.3) | 40.0 (19.0, 74.2) | 0.829 |
| IL-10/(pg·mL-1) | 3.4 (2.2, 4.6) | 2.9 (2.0, 3.9) | 0.299 |
表 1 2组患者的临床特征比较
Tab 1 Comparison of clinical characteristics between the two groups
| Clinical characteristic | irAEs group (n=63) | Non-irAEs group (n=69) | P value |
|---|---|---|---|
| Age≥65 years/n | 22 | 37 | 0.030 |
| Gender (male/female)/n | 43/20 | 46/23 | 0.847 |
| Treatment line (first line/posterior line)/n | 46/17 | 40/29 | 0.071 |
| TNM staging (Ⅲ/Ⅳ)/n | 6/57 | 4/65 | 0.421 |
| Ki-67 index/% | 49.4±23.3 | 58.9±20.8 | 0.049 |
| Her-2 expression (positive/negative)/n | 9/54 | 11/58 | 0.791 |
| PD-1/PD-L1 expression (positive/negative)/n | 22/21 | 16/17 | 0.818 |
| MMR (pMMR/dMMR)/n | 28/2 | 32/4 | 0.535 |
| Tumor marker | |||
| AFP/(ng·mL-1) | 3.3 (2.1, 7.0) | 3.3 (2.5, 4.7) | 0.209 |
| CEA/(ng·mL-1) | 6.0 (2.5, 68.5) | 6.3 (2.3, 21.7) | 0.280 |
| CA19-9/(U·mL-1) | 20.6 (8.4, 122.9) | 30.0 (9.9, 301.0) | 0.254 |
| CA125/(U·mL-1) | 31.1 (13.3, 143.5) | 23.3 (10.6, 114.0) | 0.116 |
| CA153/(U·mL-1) | 12.8 (9.4, 21.2) | 10.9 (7.4, 15.8) | 0.165 |
| CA724/(U·mL-1) | 5.7 (2.1, 49.7) | 9.1 (4.7, 48.0) | 0.549 |
| CYFRA21-1/(ng·mL-1) | 5.1 (2.6, 12.4) | 6.7 (3.5, 9.6) | 0.648 |
| CA50/(U·mL-1) | 17.6 (5.2, 115.6) | 24.6 (6.4, 191.6) | 0.153 |
| CA242/(U·mL-1) | 6.4 (3.0, 16.4) | 9.9 (4.4, 96.3) | 0.262 |
| SCC/(ng·mL-1) | 1.0 (0.8, 1.7) | 1.2 (0.8, 1.5) | 0.933 |
| NSE/(ng·mL-1) | 11.4 (9.4, 14.6) | 11.5 (9.3, 15.3) | 0.693 |
| PSA/(ng·mL-1) | 0.7 (0.5, 1.5) | 0.8 (0.5, 1.6) | 0.712 |
| Endocrine indicator | |||
| Sex hormone six | |||
| Neohombreol/(nmol·L-1) | 7.8 (1.2, 12.0) | 8.5 (1.2, 13.6) | 0.942 |
| Progestin/(nmol·L-1) | 2.0 (0.9, 2.8) | 2.1 (1.4, 3.4) | 0.381 |
| Estradiol/(pmol·L-1) | 84.0 (55.1, 105.0) | 92.0 (72.3, 124.8) | 0.274 |
| Drosophila prolactin/(ng·mL-1) | 13.6 (9.7, 19.0) | 13.7 (9.2, 19.7) | 0.812 |
| Folkopoietin/(U·L-1) | 12.8 (7.4, 20.7) | 20.1 (8.1, 39.2) | 0.256 |
| Luteinizing hormone/(U·L-1) | 5.0 (2.8, 11.4) | 6.3 (4.5, 23.3) | 0.456 |
| Cortisol hormone/(nmol·L-1) | 369.5 (313.1, 456.5) | 414.5 (298.6, 465.4) | 0.668 |
| Somatotropic hormone/(ng·mL-1) | 1.5 (0.7, 2.0) | 0.8 (0.2, 2.4) | 0.647 |
| ACTH/(pg·mL-1) | 28.5 (23.5, 39.3) | 29.1 (21.3, 51.7) | 0.269 |
| Amylase/(U·L-1) | 83.5 (63.8, 99.3) | 63.5 (54.8, 75.2) | 0.058 |
| ANA (positive/negative)/n | 22/24 | 11/17 | 0.477 |
| Blood routine index | |||
| Leukocyte count/(×109·L-1) | 5.7 (4.4, 8.3) | 5.4 (4.1, 6.2) | 0.044 |
| Neutrophil count/(×109·L-1) | 3.8 (2.4, 5.4) | 3.3 (2.3, 4.0) | 0.039 |
| Monocyte count/(×109·L-1) | 0.5 (0.4, 0.6) | 0.5 (0.4, 0.7) | 0.656 |
| Lymphocyte count/(×109·L-1) | 1.4 (1.1, 1.6) | 1.3 (1.0, 1.6) | 0.634 |
| CRP/(mg·L-1) | 2.9 (0.5, 11.5) | 1.6 (0.5, 10.3) | 0.569 |
| Neutrophil count/lymphocyte count | 2.8 (2.0, 3.9) | 2.1 (1.6, 3.6) | 0.100 |
| Neutrophil count/CRP | 1.7 (0.4, 4.7) | 2.0 (0.4, 5.0) | 0.712 |
| Leukocyte count/CRP | 2.4 (0.5, 8.5) | 3.3 (0.6, 8.3) | 0.800 |
| Lynphocyte subsets | |||
| CD19/% | 6.5 (4.4, 10.9) | 6.8 (3.9, 9.8) | 0.527 |
| CD3/% | 69.9 (60.6, 76.4) | 67.9 (57.8, 72.8) | 0.175 |
| CD4/% | 37.8±9.1 | 36.1±11.9 | 0.384 |
| CD8/% | 26.1±8.9 | 24.7±10.0 | 0.404 |
| CD4/CD8 | 1.4 (1.1, 2.2) | 1.5 (1.2, 2.4) | 0.370 |
| CD56/% | 19.9 (12.9, 27.1) | 21.0 (14.1, 32.4) | 0.183 |
| Cytokine level | |||
| Treg count/% | 8.3±2.5 | 9.8±3.0 | 0.016 |
| IFN-α/(pg·mL-1) | 1.8 (1.2, 2.3) | 1.5 (0.9, 2.4) | 0.783 |
| IL-17/(pg·mL-1) | 6.0 (1.3, 9.4) | 3.5 (1.3, 10.0) | 0.666 |
| TNF-α/(pg·mL-1) | 1.8 (1.3, 2.5) | 1.6 (1.0, 3.0) | 0.806 |
| IL-2/(pg·mL-1) | 1.2 (0.8, 1.5) | 1.2 (0.8, 1.8) | 0.240 |
| IL-4/(pg·mL-1) | 1.8 (1.0, 3.0) | 1.6 (0.9, 2.5) | 0.349 |
| IL-6/(pg·mL-1) | 8.1 (4.4, 16.2) | 6.9 (3.8, 12.2) | 0.083 |
| IL-8/(pg·mL-1) | 46.6 (22.4, 67.3) | 40.0 (19.0, 74.2) | 0.829 |
| IL-10/(pg·mL-1) | 3.4 (2.2, 4.6) | 2.9 (2.0, 3.9) | 0.299 |
| Variable | OR | 95% CI | P value |
|---|---|---|---|
| Age≥65 years | 0.489 | 0.153‒1.558 | 0.227 |
| Ki-67 index | 0.985 | 0.958‒1.013 | 0.305 |
| Leukocyte count | 0.796 | 0.346‒1.799 | 0.574 |
| Neutrophil count | 1.583 | 0.603‒4.154 | 0.351 |
| Treg count | 0.796 | 0.647‒0.977 | 0.030 |
表 2 影响irAEs发生的多因素Logistic回归分析
Tab 2 Multivariate Logistic regression analysis of the occurrence of irAEs
| Variable | OR | 95% CI | P value |
|---|---|---|---|
| Age≥65 years | 0.489 | 0.153‒1.558 | 0.227 |
| Ki-67 index | 0.985 | 0.958‒1.013 | 0.305 |
| Leukocyte count | 0.796 | 0.346‒1.799 | 0.574 |
| Neutrophil count | 1.583 | 0.603‒4.154 | 0.351 |
| Treg count | 0.796 | 0.647‒0.977 | 0.030 |
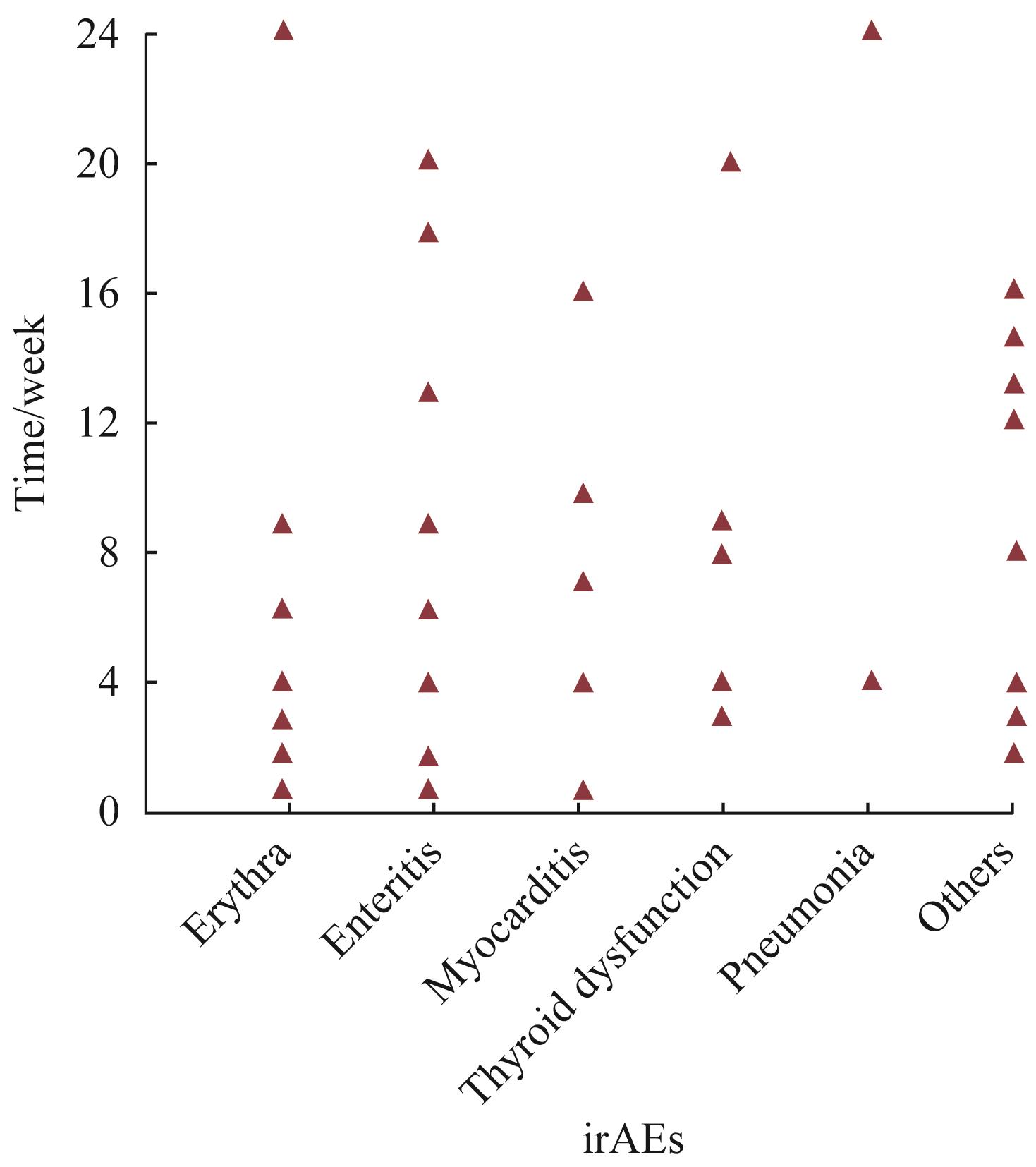
图 1 不同irAEs发生的时间分布
Fig 1 Occurrence time of different irAEs
| irAEs | Incidence/n(%) | Severity/n | |
|---|---|---|---|
| Grade 1‒2 | Grade 3‒4 | ||
| 17 (27.0) | 15 | 2 | |
| 15 (23.8) | 10 | 5 | |
| 8 (12.7) | 4 | 4 | |
| 8 (12.7) | 4 | 4 | |
| 3 (4.8) | 3 | 0 | |
| Others | 12 (19.0) | 7 | 5 |
表 3 irAEs组患者的不良反应谱及分级( n=63)
Tab 3 Adverse reaction spectrum and classification of patients in the irAEs group (n=63)
| irAEs | Incidence/n(%) | Severity/n | |
|---|---|---|---|
| Grade 1‒2 | Grade 3‒4 | ||
| 17 (27.0) | 15 | 2 | |
| 15 (23.8) | 10 | 5 | |
| 8 (12.7) | 4 | 4 | |
| 8 (12.7) | 4 | 4 | |
| 3 (4.8) | 3 | 0 | |
| Others | 12 (19.0) | 7 | 5 |
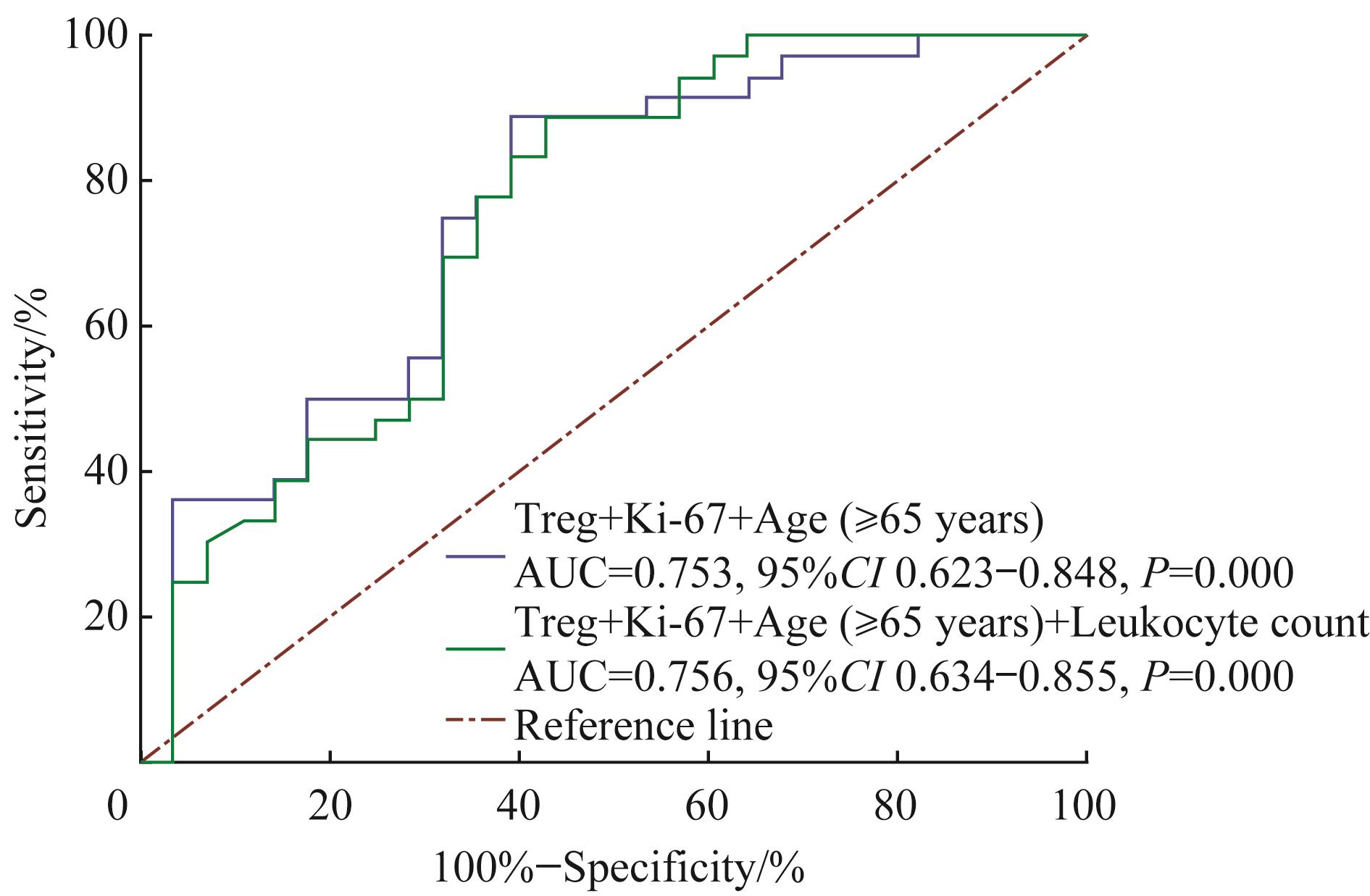
图2 2个联合指标预测irAEs发生的ROC曲线
Fig 2 ROC curve of predicting irAEs with two combined indexes
| Therapeutic effect | irAEs group (n=63)/n(%) | Non-irAEs group (n=69)/n(%) | χ2/t value | P value |
|---|---|---|---|---|
| PR | 19(30.1) | 10(14.5) | 4.679 | 0.031 |
| SD | 35(55.6) | 39(56.5) | 0.012 | 0.913 |
| PD | 9(14.3) | 20(29.0) | 4.120 | 0.042 |
表 4 2组患者的疗效比较
Tab 4 Comparison of therapeutic effects between the two groups
| Therapeutic effect | irAEs group (n=63)/n(%) | Non-irAEs group (n=69)/n(%) | χ2/t value | P value |
|---|---|---|---|---|
| PR | 19(30.1) | 10(14.5) | 4.679 | 0.031 |
| SD | 35(55.6) | 39(56.5) | 0.012 | 0.913 |
| PD | 9(14.3) | 20(29.0) | 4.120 | 0.042 |
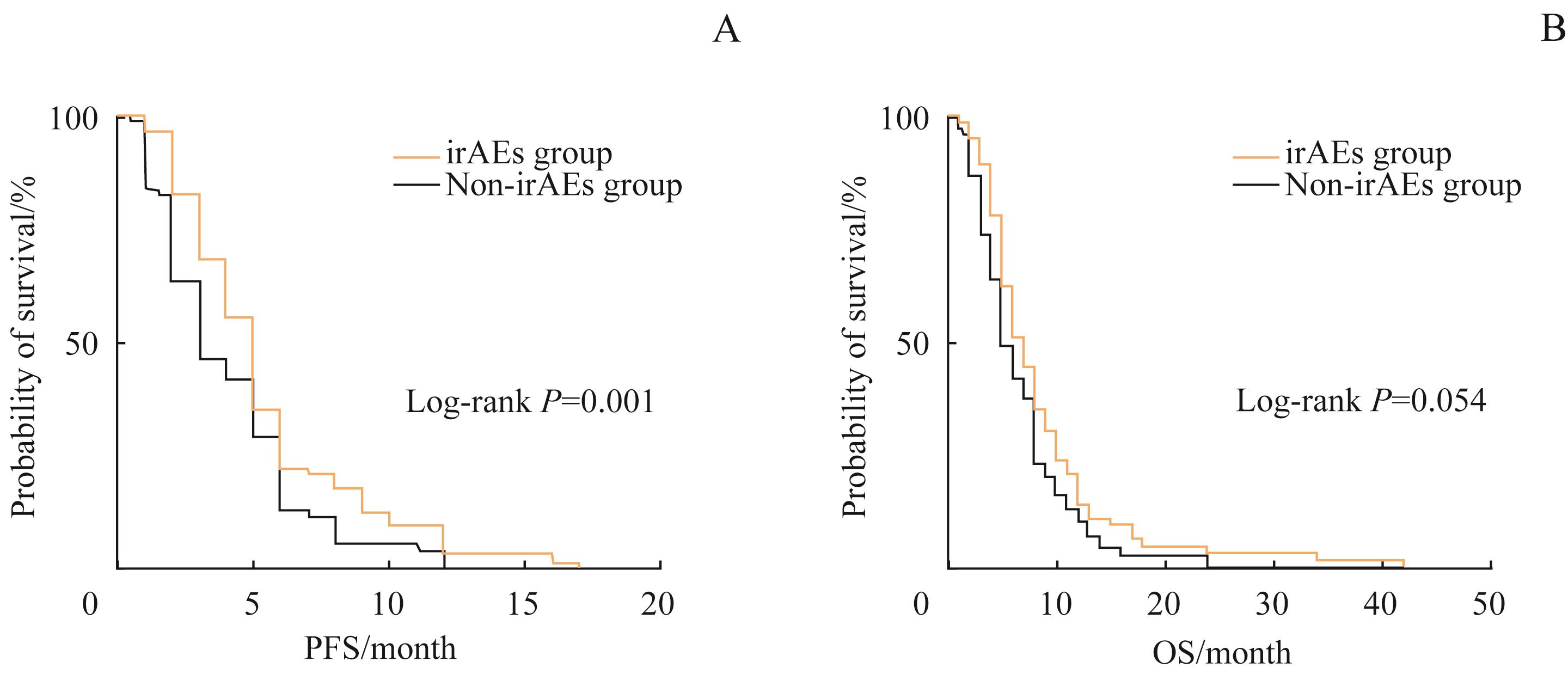
图3 2组患者PFS(A)、OS(B)的Kaplan-Meier曲线分析
Fig 3 Kaplan-Meier analysis of PFS (A) and OS (B) of patients in the two groups
| Variable | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Cox analysis | Multivariate Cox analysis | Univariate Cox analysis | Multivariate Cox analysis | |||||
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |
| Age≥65 years | 0.907 (0.646‒1.286) | 0.586 | 0.805 (0.557‒1.164) | 0.250 | 1.205 (0.852‒1.705) | 0.293 | 1.142 (0.795‒1.640) | 0.473 |
| Gender | 0.977 (0.677‒1.408) | 0.899 | 0.823 (0.560‒1.209) | 0.320 | 0.927 (0.643‒1.338) | 0.687 | 0.869 (0.523‒1.443) | 0.588 |
| TNM staging | 1.371 (0.715‒2.625) | 0.342 | 0.945 (0.651‒1.374) | 0.769 | 1.614 (0.816‒3.194) | 0.169 | 1.372 (0.666‒2.826) | 0.391 |
| Treatment line | 0.794 (0.552‒1.141) | 0.213 | 1.591 (0.794‒3.186) | 0.190 | 0.992 (0.686‒1.433) | 0.965 | 0.924 (0.636‒1.341) | 0.677 |
| Her-2 expression | 1.001 (0.620‒1.617) | 0.996 | 1.045 (0.634‒1.723) | 0.863 | 0.815 (0.495‒1.341) | 0.421 | 0.988 (0.678‒1.439) | 0.949 |
| irAEs | 0.609 (0.431‒0.863) | 0.005 | 0.608 (0.431‒0.863) | 0.006 | 0.735 (0.520‒1.039) | 0.081 | 0.761 (0.535‒1.083) | 0.129 |
表 5 影响肿瘤预后因素的Cox比例风险回归分析
Tab 5 Cox proportional hazards regression analysis of prognostic factors of cancer
| Variable | PFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Cox analysis | Multivariate Cox analysis | Univariate Cox analysis | Multivariate Cox analysis | |||||
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |
| Age≥65 years | 0.907 (0.646‒1.286) | 0.586 | 0.805 (0.557‒1.164) | 0.250 | 1.205 (0.852‒1.705) | 0.293 | 1.142 (0.795‒1.640) | 0.473 |
| Gender | 0.977 (0.677‒1.408) | 0.899 | 0.823 (0.560‒1.209) | 0.320 | 0.927 (0.643‒1.338) | 0.687 | 0.869 (0.523‒1.443) | 0.588 |
| TNM staging | 1.371 (0.715‒2.625) | 0.342 | 0.945 (0.651‒1.374) | 0.769 | 1.614 (0.816‒3.194) | 0.169 | 1.372 (0.666‒2.826) | 0.391 |
| Treatment line | 0.794 (0.552‒1.141) | 0.213 | 1.591 (0.794‒3.186) | 0.190 | 0.992 (0.686‒1.433) | 0.965 | 0.924 (0.636‒1.341) | 0.677 |
| Her-2 expression | 1.001 (0.620‒1.617) | 0.996 | 1.045 (0.634‒1.723) | 0.863 | 0.815 (0.495‒1.341) | 0.421 | 0.988 (0.678‒1.439) | 0.949 |
| irAEs | 0.609 (0.431‒0.863) | 0.005 | 0.608 (0.431‒0.863) | 0.006 | 0.735 (0.520‒1.039) | 0.081 | 0.761 (0.535‒1.083) | 0.129 |
| 1 | CAO W, CHEN H D, YU Y W, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chin Med J (Engl), 2021, 134(7): 783-791. |
| 2 | SIEGEL R L, MILLER K D, FUCHS H E, et al. Cancer statistics, 2022[J]. CA Cancer J Clin, 2022, 72(1): 7-33. |
| 3 | SMYTH E C, NILSSON M, GRABSCH H I, et al. Gastric cancer[J]. Lancet, 2020, 396(10251): 635-648. |
| 4 | AHERN E, SOLOMON B J, HUI R N, et al. Neoadjuvant immunotherapy for non-small cell lung cancer: right drugs, right patient, right time? [J]. J Immunother Cancer, 2021, 9(6): e002248. |
| 5 | COSMAI L, PIROVANO M, RE SARTÒ G V, et al. Immunotherapy in kidney cancer: how it has changed and what are the challenges for the nephrologist - focus on pembrolizumab[J]. G Ital Nefrol, 2021, 38(5): 2021-vol5. |
| 6 | JOSHI S S, BADGWELL B D. Current treatment and recent progress in gastric cancer[J]. CA Cancer J Clin, 2021, 71(3): 264-279. |
| 7 | LI K X, ZHANG A, LI X Y, et al. Advances in clinical immunotherapy for gastric cancer[J]. Biochim Biophys Acta Rev Cancer, 2021, 1876(2): 188615. |
| 8 | KANG Y K, BOKU N, SATOH T, et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): a randomised, double-blind, placebo-controlled, phase 3 trial[J]. Lancet, 2017, 390(10111): 2461-2471. |
| 9 | JANJIGIAN Y Y, SHITARA K, MOEHLER M, et al. First-line nivolumab plus chemotherapy versus chemotherapy alone for advanced gastric, gastro-oesophageal junction, and oesophageal adenocarcinoma (CheckMate 649): a randomised, open-label, phase 3 trial[J]. Lancet, 2021, 398(10294): 27-40. |
| 10 | Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0[EB/OL]. (2009-05-28)[2022-03-10]. https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.0_2009-05-29_QuickReference_8.5x11.pdf. |
| 11 | BORST J, BUSSELAAR J, BOSMA D M T, et al. Mechanism of action of PD-1 receptor/ligand targeted cancer immunotherapy[J]. Eur J Immunol, 2021, 51(8): 1911-1920. |
| 12 | BAJWA R, CHEEMA A, KHAN T, et al. Adverse effects of immune checkpoint inhibitors (programmed death-1 inhibitors and cytotoxic T-lymphocyte-associated protein-4 inhibitors): results of a retrospective study[J]. J Clin Med Res, 2019, 11(4): 225-236. |
| 13 | TOPALIAN S L, HODI F S, BRAHMER J R, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer[J]. N Engl J Med, 2012, 366(26): 2443-2454. |
| 14 | YEUNG S J, QDAISAT A, CHAFTARI P, et al. Diagnosis and management of immune-related adverse effects of immune checkpoint therapy in the emergency department[J]. J Am Coll Emerg Physicians Open, 2020, 1(6): 1637-1659. |
| 15 | MARTINS F, SOFIYA L, SYKIOTIS G P, et al. Adverse effects of immune-checkpoint inhibitors: epidemiology, management and surveillance[J]. Nat Rev Clin Oncol, 2019, 16(9): 563-580. |
| 16 | KUMAR V, CHAUDHARY N, GARG M, et al. Current diagnosis and management of immune related adverse events (irAEs) induced by immune checkpoint inhibitor therapy[J]. Front Pharmacol, 2017, 8: 49. |
| 17 | APALLA Z, RAPOPORT B, SIBAUD V. Dermatologic immune-related adverse events: the toxicity spectrum and recommendations for management[J]. Int J Womens Dermatol, 2021, 7(5Part A): 625-635. |
| 18 | PANG W W, PRICE E A, SAHOO D, et al. Human bone marrow hematopoietic stem cells are increased in frequency and myeloid-biased with age[J]. Proc Natl Acad Sci USA, 2011, 108(50): 20012-20017. |
| 19 | KUGEL C H 3rd, DOUGLASS S M, WEBSTER M R, et al. Age correlates with response to anti-PD1, reflecting age-related differences in intratumoral effector and regulatory T-cell populations[J]. Clin Cancer Res, 2018, 24(21): 5347-5356. |
| 20 | WANG Y H, ZONG B G, YU Y, et al. Ki67 index changes and tumor-infiltrating lymphocyte levels impact the prognosis of triple-negative breast cancer patients with residual disease after neoadjuvant chemotherapy[J]. Front Oncol, 2021, 11: 668610. |
| 21 | FUJISAWA Y, YOSHINO K, OTSUKA A, et al. Fluctuations in routine blood count might signal severe immune-related adverse events in melanoma patients treated with nivolumab[J]. J Dermatol Sci, 2017, 88(2): 225-231. |
| 22 | DIEHL A, YARCHOAN M, HOPKINS A, et al. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumors treated with PD-1 checkpoint inhibitors[J]. Oncotarget, 2017, 8(69): 114268-114280. |
| 23 | TANAKA A, SAKAGUCHI S. Targeting Treg cells in cancer immunotherapy[J]. Eur J Immunol, 2019, 49(8): 1140-1146. |
| 24 | LIU X Y, SHI Y Q, ZHANG D M, et al. Risk factors for immune-related adverse events: what have we learned and what lies ahead? [J]. Biomark Res, 2021, 9(1): 79. |
| 25 | GREISEN S R, DELEURAN B. Checkpoint molecules in rheumatology-or the benefits of being exhausted[J]. Curr Rheumatol Rep, 2021, 23(4): 22. |
| 26 | VARGAS F A, FURNESS A J S, LITCHFIELD K, et al. Fc effector function contributes to the activity of human anti-CTLA-4 antibodies[J]. Cancer Cell, 2018, 33(4): 649-663.e4. |
| 27 | 中国临床肿瘤学会指南工作委员会. 中国临床肿瘤学会指南工作委员会(CSCO)免疫检查点抑制剂临床应用指南2021[M]. 北京: 人民卫生出版社, 2021: 1-176. |
| Guidelines Working Committee of Chinese Society of Clinical Oncology. Guidelines of Chinese Society of Clinical Oncology (CSCO) immune checkpoint inhibitor clinical practice[M]. Beijing: People's Medical Publishing House, 2021: 1-176. | |
| 28 | THOMPSON J A, SCHNEIDER B J, BRAHMER J, et al. Management of immunotherapy-related toxicities, version 1.2019[J]. J Natl Compr Cancer Netw, 2019, 17(3): 255-289. |
| 29 | ALLOUCHERY M, LOMBARD T, MARTIN M, et al. Safety of immune checkpoint inhibitor rechallenge after discontinuation for grade ≥2 immune-related adverse events in patients with cancer[J]. J Immunother Cancer, 2020, 8(2): e001622. |
| 30 | DOWNEY S G, KLAPPER J A, SMITH F O, et al. Prognostic factors related to clinical response in patients with metastatic melanoma treated by CTL-associated antigen-4 blockade[J]. Clin Cancer Res, 2007, 13(22 Pt 1): 6681-6688. |
| 31 | RZEPECKI A K, CHENG H Y, MCLELLAN B N. Cutaneous toxicity as a predictive biomarker for clinical outcome in patients receiving anticancer therapy[J]. J Am Acad Dermatol, 2018, 79(3): 545-555. |
| 32 | NAKAMURA Y, TANAKA R, ASAMI Y, et al. Correlation between vitiligo occurrence and clinical benefit in advanced melanoma patients treated with nivolumab: a multi-institutional retrospective study[J]. J Dermatol, 2017, 44(2): 117-122. |
| 33 | ROGADO J, SÁNCHEZ-TORRES J M, ROMERO-LAORDEN N, et al. Immune-related adverse events predict the therapeutic efficacy of anti-PD-1 antibodies in cancer patients[J]. Eur J Cancer, 2019, 109: 21-27. |
| [1] | 魏豪, 邱家俊, 颜景斌. 不同表达矩阵对筛选差异长链非编码RNA的影响[J]. 上海交通大学学报(医学版), 2022, 42(7): 911-918. |
| [2] | 何烨, 方芳. 非体外循环冠状动脉搭桥患者术前糖化血红蛋白水平与术后谵妄的关系[J]. 上海交通大学学报(医学版), 2022, 42(1): 21-27. |
| [3] | 凌徐心仪, 张瑶, 钟华. 非小细胞肺癌免疫治疗获益人群筛选的研究进展[J]. 上海交通大学学报(医学版), 2021, 41(8): 1114-1119. |
| [4] | 丁继平, 李晓光, 刘忠龙, 邓刚, 姚原, 何悦. 救治性手术联合放疗与化疗序贯免疫检查点抑制剂治疗复发转移舌鳞癌1例报道[J]. 上海交通大学学报(医学版), 2021, 41(12): 1704-1708. |
| [5] | 岳犇, 王高明, 杨鹿笛, 崔然, 郁丰荣. 胃癌患者预后相关微RNA预测模型的构建及其应用价值探讨[J]. 上海交通大学学报(医学版), 2021, 41(11): 1436-1445. |
| [6] | 袁瑞雪, 傅迎美, 禹顺英. 辅助性T细胞17和调节性T细胞在抑郁症中的作用机制研究进展[J]. 上海交通大学学报(医学版), 2021, 41(10): 1384-1388. |
| [7] | 何春明,尹 航,郑佳杰,唐 健,傅于捷,赵晓菁. 肺癌免疫治疗:免疫抑制细胞和肺内免疫[J]. 上海交通大学学报(医学版), 2020, 40(8): 1137-1142. |
| [8] | 袁 芸,张洪铭,黄 慧. 牙周炎对大鼠外周血中辅助性T细胞分群的影响[J]. 上海交通大学学报(医学版), 2020, 40(10): 1360-1364. |
| [9] | 张晓欣,赵爱民. CCL20对CBA/J小鼠CCR6+调节性T细胞及妊娠结局的影响[J]. 上海交通大学学报(医学版), 2016, 36(2): 147-. |
| [10] | 李维宏,牟晓玲. 脂联素对不明原因复发性流产患者外周血Th17/Treg细胞分群及细胞因子水平的影响[J]. 上海交通大学学报(医学版), 2015, 35(7): 1004-. |
| [11] | 孙蔚,朱海超,甘建和,等. 戊型病毒性肝炎患者外周血Th17、Treg、Th17/Treg变化及其临床意义[J]. 上海交通大学学报(医学版), 2015, 35(11): 1647-. |
| [12] | 邱 添,滕银成,徐 亮. 过继性转移TGF-β诱导CD4+CD25+调节性T细胞对自然流产模型小鼠胚胎丢失率的影响[J]. 上海交通大学学报(医学版), 2014, 34(8): 1120-. |
| [13] | 俞翀曌,曹 芸,陈 风,等. 肾小球滤过率估算方程诊断性能评价[J]. 上海交通大学学报(医学版), 2013, 33(11): 1496-. |
| [14] | 柳龙根, 申红玉, 叶春艳, 等. 慢性丙型肝炎患者外周血CD4+CD25high调节性T细胞与抗病毒疗效的关系[J]. , 2012, 32(12): 1610-. |
| [15] | 邵晓轶, 周 芸, 路丽明, 等. p38 MAPK信号通路在B7H1-Ig融合蛋白诱导Tr1细胞分化中的作用[J]. , 2012, 32(11): 1448-. |
| 阅读次数 | ||||||||||||||||||||||||||||||||||||||||||||||||||
|
全文 373
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||
|
摘要 464
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||