Journal of Shanghai Jiao Tong University (Medical Science) ›› 2026, Vol. 46 ›› Issue (6): 770-777.doi: 10.3969/j.issn.1674-8115.2026.06.009
• Clinical research • Previous Articles
Zhang Shuting, Yang Xin( )
)
Received:2025-12-08
Accepted:2026-01-30
Online:2026-06-28
Published:2026-06-29
Contact:
Yang Xin
E-mail:yangxin@xinhuamed.com.cn
Supported by:CLC Number:
Zhang Shuting, Yang Xin. Effects of maxillary sinus pneumatization on bone thickness of infrazygomatic crest for miniscrew implant placement[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(6): 770-777.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2026.06.009
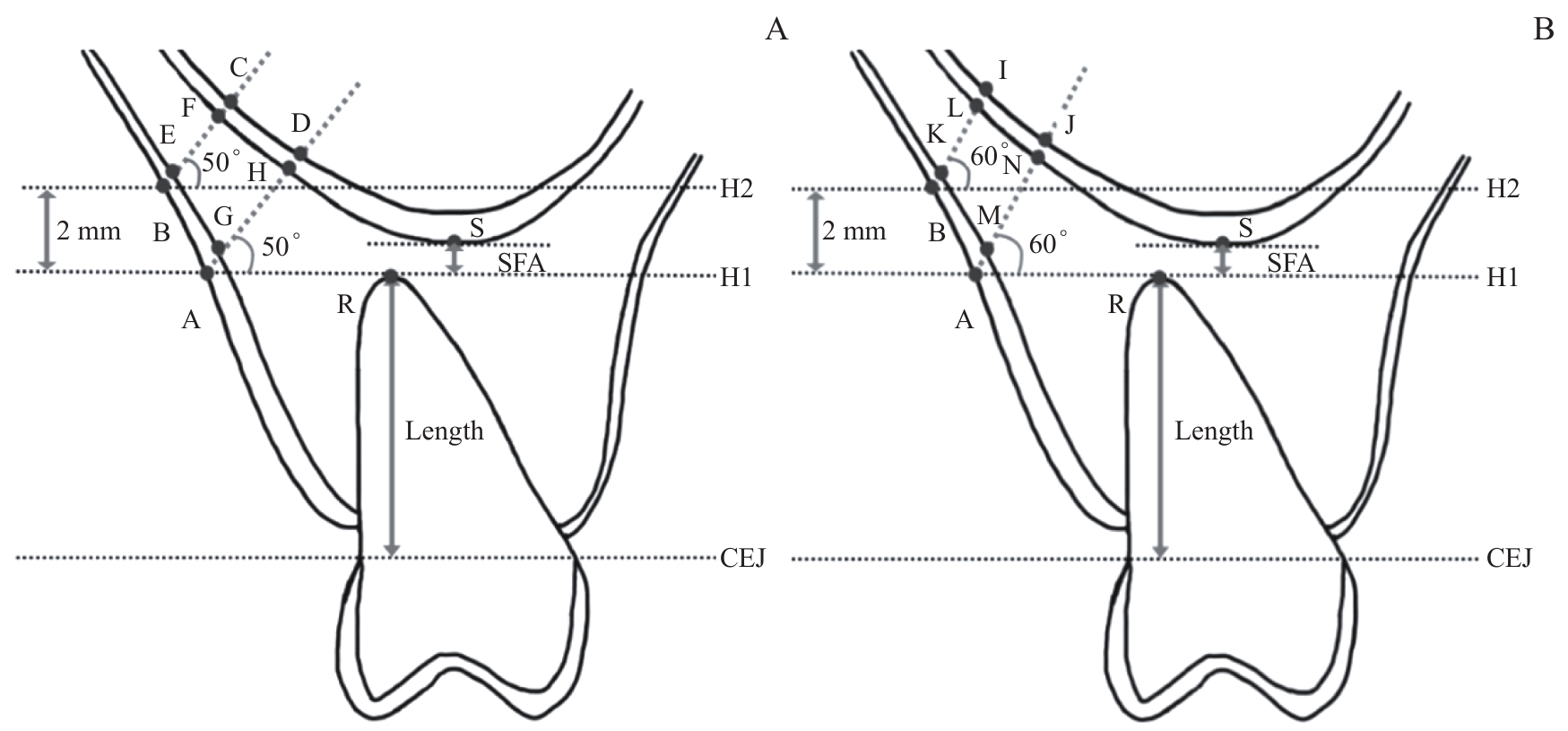
Fig 1 Insertion site measurements
| Insertion path | U6M | U6D | U7M | |||
|---|---|---|---|---|---|---|
| P value | P value | P value | ||||
| A50-BT | <0.001 | <0.001 | 0.012 | |||
| HS | 6.79±2.21 | 5.67±1.71 | 4.05±1.69 | |||
| MS | 4.03±1.02 | 3.96±1.03 | 4.35±0.88 | |||
| LS | 2.28±0.82 | 2.27±0.81 | 2.64±1.54 | |||
| A60-BT | <0.001 | <0.001 | 0.002 | |||
| HS | 6.35±1.97 | 5.42±1.47 | 4.19±1.62 | |||
| MS | 4.13±1.06 | 3.96±1.06 | 4.47±1.00 | |||
| LS | 2.30±0.83 | 2.29±0.87 | 2.54±1.36 | |||
| B50-BT | <0.001 | <0.001 | 0.028 | |||
| HS | 4.91±1.38 | 4.19±1.34 | 3.08±1.29 | |||
| MS | 3.14±0.94 | 2.96±0.98 | 3.21±0.91 | |||
| LS | 1.87±0.64 | 1.84±0.65 | 2.09±1.01 | |||
| B60-BT | <0.001 | <0.001 | 0.017 | |||
| HS | 4.98±1.83 | 4.21±1.35 | 3.22±1.32 | |||
| MS | 3.27±1.04 | 2.99±1.00 | 3.35±1.01 | |||
| LS | 1.94±0.66 | 1.90±0.68 | 2.12±0.98 | |||
| A50-CBT | <0.001 | <0.001 | 0.002 | |||
| HS | 3.49±0.73 | 3.31±0.69 | 3.09±0.95 | |||
| MS | 3.12±0.77 | 2.97±0.67 | 3.43±0.87 | |||
| LS | 2.19±0.65 | 2.08±0.54 | 2.16±0.68 | |||
| A60-CBT | <0.001 | <0.001 | <0.001 | |||
| HS | 3.62±0.88 | 3.52±0.78 | 3.37±0.91 | |||
| MS | 3.42±0.79 | 3.11±0.61 | 3.96±1.08 | |||
| LS | 2.23±0.70 | 2.09±0.59 | 2.28±0.74 | |||
| B50-CBT | <0.001 | <0.001 | 0.002 | |||
| HS | 3.42±0.82 | 2.99±0.65 | 2.73±0.81 | |||
| MS | 3.01±0.80 | 2.63±0.63 | 2.96±0.87 | |||
| LS | 1.84±0.66 | 1.78±0.55 | 1.89±0.50 | |||
| B60-CBT | <0.001 | <0.001 | <0.001 | |||
| HS | 3.53±0.94 | 3.12±0.70 | 2.90±0.89 | |||
| MS | 3.14±0.86 | 2.72±0.68 | 3.13±0.88 | |||
| LS | 1.94±0.66 | 1.86±0.60 | 1.95±0.51 | |||
Tab 1 Comparison of BT and CBT among different sinus floor height groups under various insertion paths (mm)
| Insertion path | U6M | U6D | U7M | |||
|---|---|---|---|---|---|---|
| P value | P value | P value | ||||
| A50-BT | <0.001 | <0.001 | 0.012 | |||
| HS | 6.79±2.21 | 5.67±1.71 | 4.05±1.69 | |||
| MS | 4.03±1.02 | 3.96±1.03 | 4.35±0.88 | |||
| LS | 2.28±0.82 | 2.27±0.81 | 2.64±1.54 | |||
| A60-BT | <0.001 | <0.001 | 0.002 | |||
| HS | 6.35±1.97 | 5.42±1.47 | 4.19±1.62 | |||
| MS | 4.13±1.06 | 3.96±1.06 | 4.47±1.00 | |||
| LS | 2.30±0.83 | 2.29±0.87 | 2.54±1.36 | |||
| B50-BT | <0.001 | <0.001 | 0.028 | |||
| HS | 4.91±1.38 | 4.19±1.34 | 3.08±1.29 | |||
| MS | 3.14±0.94 | 2.96±0.98 | 3.21±0.91 | |||
| LS | 1.87±0.64 | 1.84±0.65 | 2.09±1.01 | |||
| B60-BT | <0.001 | <0.001 | 0.017 | |||
| HS | 4.98±1.83 | 4.21±1.35 | 3.22±1.32 | |||
| MS | 3.27±1.04 | 2.99±1.00 | 3.35±1.01 | |||
| LS | 1.94±0.66 | 1.90±0.68 | 2.12±0.98 | |||
| A50-CBT | <0.001 | <0.001 | 0.002 | |||
| HS | 3.49±0.73 | 3.31±0.69 | 3.09±0.95 | |||
| MS | 3.12±0.77 | 2.97±0.67 | 3.43±0.87 | |||
| LS | 2.19±0.65 | 2.08±0.54 | 2.16±0.68 | |||
| A60-CBT | <0.001 | <0.001 | <0.001 | |||
| HS | 3.62±0.88 | 3.52±0.78 | 3.37±0.91 | |||
| MS | 3.42±0.79 | 3.11±0.61 | 3.96±1.08 | |||
| LS | 2.23±0.70 | 2.09±0.59 | 2.28±0.74 | |||
| B50-CBT | <0.001 | <0.001 | 0.002 | |||
| HS | 3.42±0.82 | 2.99±0.65 | 2.73±0.81 | |||
| MS | 3.01±0.80 | 2.63±0.63 | 2.96±0.87 | |||
| LS | 1.84±0.66 | 1.78±0.55 | 1.89±0.50 | |||
| B60-CBT | <0.001 | <0.001 | <0.001 | |||
| HS | 3.53±0.94 | 3.12±0.70 | 2.90±0.89 | |||
| MS | 3.14±0.86 | 2.72±0.68 | 3.13±0.88 | |||
| LS | 1.94±0.66 | 1.86±0.60 | 1.95±0.51 | |||
| Insertion path | P value | Insertion path | P value | ||||
|---|---|---|---|---|---|---|---|
| A50-BT | A50-CBT | ||||||
| HS | MS | -0.30±0.56 | 0.598 | HS | MS | -0.34±0.32 | 0.305 |
| HS | LS | 1.41±0.53 | 0.012 | HS | LS | 0.93±0.31 | 0.005 |
| MS | LS | 1.71±0.61 | 0.008 | MS | LS | 1.27±0.35 | <0.001 |
| A60-BT | A60-CBT | ||||||
| HS | MS | -0.28±0.53 | 0.605 | HS | MS | -0.60±0.35 | 0.093 |
| HS | LS | 1.66±0.51 | 0.002 | HS | LS | 1.09±0.33 | 0.002 |
| MS | LS | 1.93±0.58 | 0.002 | MS | LS | 1.69±0.37 | <0.001 |
| B50-BT | B50-CBT | ||||||
| HS | MS | -0.12±0.43 | 0.771 | HS | MS | -0.24±0.28 | 0.407 |
| HS | LS | 0.99±0.40 | 0.019 | HS | LS | 0.83±0.27 | 0.004 |
| MS | LS | 1.12±0.46 | 0.020 | MS | LS | 1.07±0.31 | <0.001 |
| B60-BT | B60-CBT | ||||||
| HS | MS | -0.14±0.44 | 0.752 | HS | MS | -0.23±0.30 | 0.454 |
| HS | LS | 1.09±0.41 | 0.012 | HS | LS | 0.95±0.29 | 0.002 |
| MS | LS | 1.23±0.47 | 0.013 | MS | LS | 1.18±0.33 | <0.001 |
Tab 2 Post-hoc tests for BT and CBT among different sinus floor height groups at the U7M site under various insertion paths (mm)
| Insertion path | P value | Insertion path | P value | ||||
|---|---|---|---|---|---|---|---|
| A50-BT | A50-CBT | ||||||
| HS | MS | -0.30±0.56 | 0.598 | HS | MS | -0.34±0.32 | 0.305 |
| HS | LS | 1.41±0.53 | 0.012 | HS | LS | 0.93±0.31 | 0.005 |
| MS | LS | 1.71±0.61 | 0.008 | MS | LS | 1.27±0.35 | <0.001 |
| A60-BT | A60-CBT | ||||||
| HS | MS | -0.28±0.53 | 0.605 | HS | MS | -0.60±0.35 | 0.093 |
| HS | LS | 1.66±0.51 | 0.002 | HS | LS | 1.09±0.33 | 0.002 |
| MS | LS | 1.93±0.58 | 0.002 | MS | LS | 1.69±0.37 | <0.001 |
| B50-BT | B50-CBT | ||||||
| HS | MS | -0.12±0.43 | 0.771 | HS | MS | -0.24±0.28 | 0.407 |
| HS | LS | 0.99±0.40 | 0.019 | HS | LS | 0.83±0.27 | 0.004 |
| MS | LS | 1.12±0.46 | 0.020 | MS | LS | 1.07±0.31 | <0.001 |
| B60-BT | B60-CBT | ||||||
| HS | MS | -0.14±0.44 | 0.752 | HS | MS | -0.23±0.30 | 0.454 |
| HS | LS | 1.09±0.41 | 0.012 | HS | LS | 0.95±0.29 | 0.002 |
| MS | LS | 1.23±0.47 | 0.013 | MS | LS | 1.18±0.33 | <0.001 |
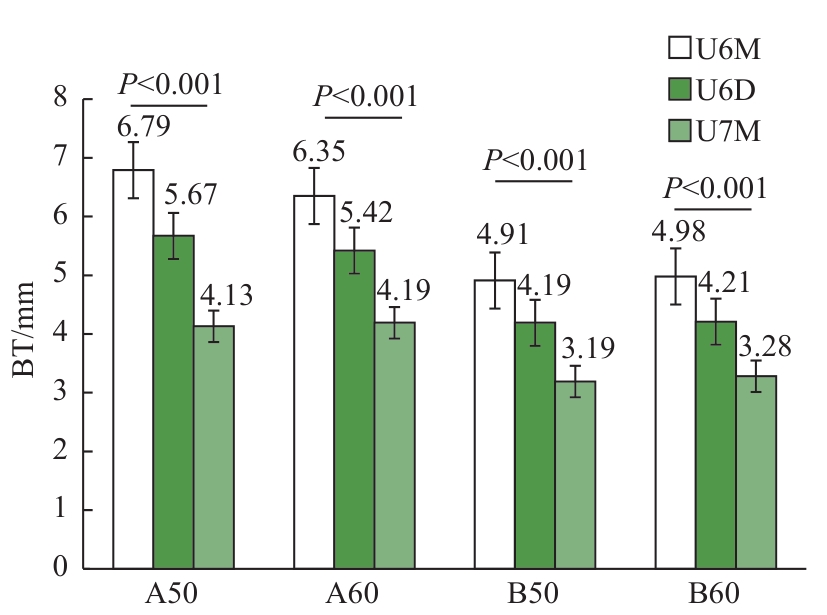
Fig 2 Comparison of BT among sagittal insertion sites in the HS Group under the same insertion height and angulation
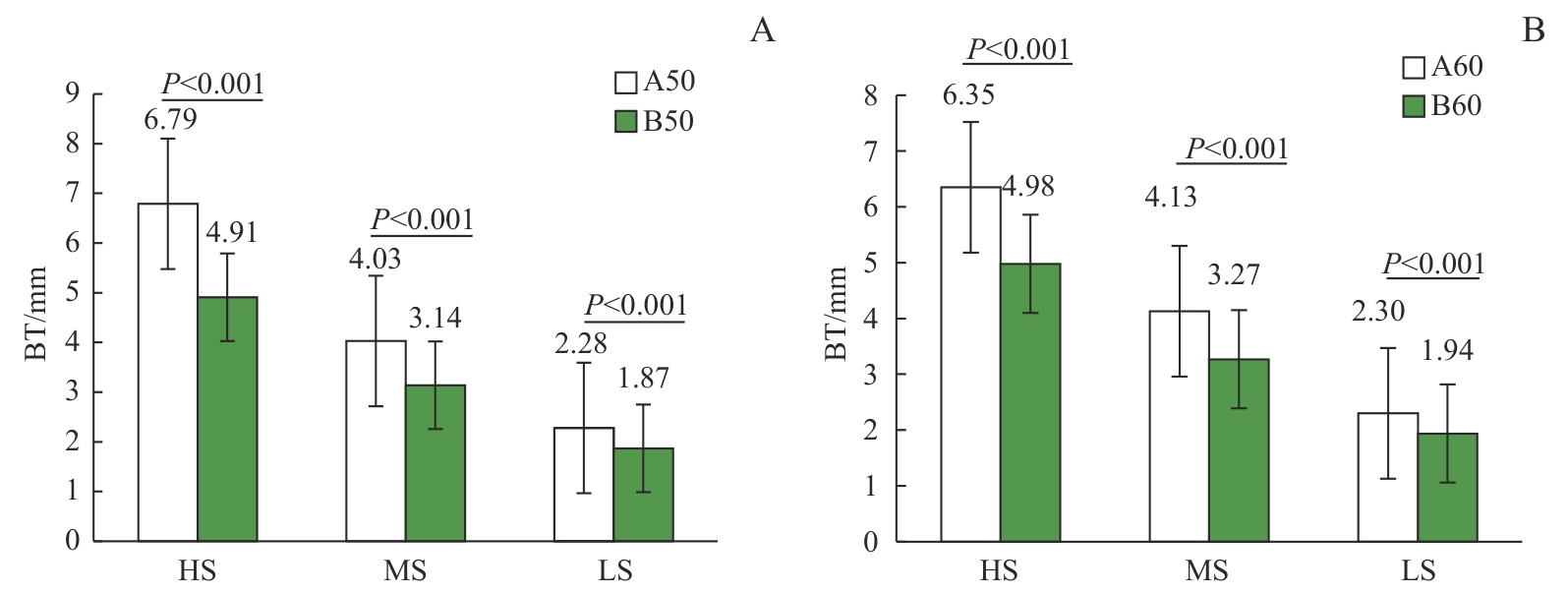
Fig 3 Comparison of BT between two insertion heights at 50°or 60° insertion angles
| Insertion height | HS | MS | LS | |||
|---|---|---|---|---|---|---|
| P value | P value | P value | ||||
| A50-BT | 6.79±2.21 | 0.036 | 4.03±1.02 | 0.037 | 2.28±0.82 | 0.244 |
| A60-BT | 6.35±1.97 | 4.13±1.06 | 2.30±0.83 | |||
| B50-BT | 4.91±1.38 | 0.749 | 3.14±0.94 | <0.001 | 1.87±0.64 | <0.001 |
| B60-BT | 4.98±1.83 | 3.27±1.04 | 1.94±0.66 | |||
Tab 3 Comparison of BT between 50° and 60° insertion angles at two insertion heights (mm)
| Insertion height | HS | MS | LS | |||
|---|---|---|---|---|---|---|
| P value | P value | P value | ||||
| A50-BT | 6.79±2.21 | 0.036 | 4.03±1.02 | 0.037 | 2.28±0.82 | 0.244 |
| A60-BT | 6.35±1.97 | 4.13±1.06 | 2.30±0.83 | |||
| B50-BT | 4.91±1.38 | 0.749 | 3.14±0.94 | <0.001 | 1.87±0.64 | <0.001 |
| B60-BT | 4.98±1.83 | 3.27±1.04 | 1.94±0.66 | |||
| [1] | Khan J, Goyal M, Kumar M, et al. Comparative evaluation of displacement and stress distribution pattern during maxillary arch distalization with Infra Zygomatic Screw: a three dimensional finite element study[J]. Int Orthod, 2021, 19(2): 291-300. |
| [2] | Shaikh A, Jamdar A F, Galgali S A, et al. Efficacy of infrazygomatic crest implants for full-arch distalization of maxilla and reduction of gummy smile in class II malocclusion[J]. J Contemp Dent Pract, 2021, 22(10): 1135-1143. |
| [3] | Wu X X, Liu H B, Luo C, et al. Three-dimensional evaluation on the effect of maxillary dentition distalization with miniscrews implanted in the infrazygomatic crest[J]. Implant Dent, 2018, 27(1): 22-27. |
| [4] | Lima A Jr, Domingos R G, Cunha Ribeiro A N, et al. Safe sites for orthodontic miniscrew insertion in the infrazygomatic crest area in different facial types: a tomographic study[J]. Am J Orthod Dentofacial Orthop, 2022, 161(1): 37-45. |
| [5] | Liu H B, Wu X X, Yang L, et al. Safe zones for miniscrews in maxillary dentition distalization assessed with cone-beam computed tomography[J]. Am J Orthod Dentofacial Orthop, 2017, 151(3): 500-506. |
| [6] | Elsayed S A, Alolayan A B, Alahmadi A, et al. Revisited maxillary sinus pneumatization narrative of observation in Al-Madinah Al-Munawwarah, Saudi Arabia: a retrospective cross-sectional study[J]. Saudi Dent J, 2019, 31(2): 212-218. |
| [7] | Chang C H, Lin J H, Roberts W E. Success of infrazygomatic crest bone screws: patient age, insertion angle, sinus penetration, and terminal insertion torque[J]. Am J Orthod Dentofacial Orthop, 2022, 161(6): 783-790. |
| [8] | Wu X S, Cai Q D, Huang D, et al. Cone-beam computed tomography-based analysis of maxillary sinus pneumatization extended into the alveolar process in different age groups[J]. BMC Oral Health, 2022, 22(1): 393. |
| [9] | Tavares A, Crusoé-Rebello I M, Neves F S. Tomographic evaluation of infrazygomatic crest for orthodontic anchorage in different vertical and sagittal skeletal patterns[J]. J Clin Exp Dent, 2020, 12(11): e1015-e1020. |
| [10] | Vargas E O A, Lopes de Lima R, Nojima L I. Mandibular buccal shelf and infrazygomatic crest thicknesses in patients with different vertical facial heights[J]. Am J Orthod Dentofac Orthop, 2020, 158(3): 349-356. |
| [11] | 陈立艳, 刘志杰, 苑芳连, 等. 颧牙槽嵴区骨宽度及皮质骨厚度的CBCT测量分析[J]. 口腔医学研究, 2017, 33(6): 637-641. |
| Chen L Y, Liu Z J, Yuan F L, et al. Bone width and cortical bone thickness of infrazygomatic crest analysed with cone-beam computed tomography[J]. Journal of Oral Science Research, 2017, 33(6):637-641. | |
| [12] | Farnsworth D, Rossouw P E, Ceen R F, et al. Cortical bone thickness at common miniscrew implant placement sites[J]. Am J Orthod Dentofacial Orthop, 2011, 139(4): 495-503. |
| [13] | Chang C C H, Lin J S Y, Yeh H Y. Extra-alveolar bone screws for conservative correction of severe malocclusion without extractions or orthognathic surgery[J]. Curr Osteoporos Rep, 2018, 16(4): 387-394. |
| [14] | Holmes P B, Wolf B J, Zhou J. A CBCT atlas of buccal cortical bone thickness in interradicular spaces[J]. Angle Orthod, 2015, 85(6): 911-919. |
| [15] | Whyte A, Boeddinghaus R. The maxillary sinus: physiology, development and imaging anatomy[J]. Dentomaxillofacial Radiol, 2019, 48(8): 20190205. |
| [16] | Göçmen G, Borahan M O, Aktop S, et al. Effect of septal deviation, concha bullosa and haller's cell on maxillary sinus's inferior pneumatization: a retrospective study[J]. Open Dent J, 2015, 9: 282-286. |
| [17] | Santos A R, Castellucci M, Crusoé-Rebello I M, et al. Assessing bone thickness in the infrazygomatic crest area aiming the orthodontic miniplates positioning: a tomographic study[J]. Dental Press J Orthod, 2017, 22(4): 70-76. |
| [18] | 王鹏, 陈铮晰, 吴军, 等. 颧牙槽嵴微种植体植入与上颌窦底位置关系的解剖研究[J]. 上海口腔医学, 2017, 26(6): 623-627. |
| Wang P, Chen Z X, Wu J, et al. Study of three-dimensional anatomical relationship between infrazygomatic crest and maxillary sinus for miniscrew insertion[J]. Shanghai Journal of Stomatology, 2017, 26(6): 623-627. | |
| [19] | Hirai Y, Watanabe K, Deguchi T, et al. Influence of insertion depth on stress distribution in orthodontic miniscrew and the surrounding bone by finite element analysis[J]. Dent Mater J, 2021, 40(5): 1270-1276. |
| [20] | Murugesan A, Sivakumar A. Comparison of bone thickness in infrazygomatic crest area at various miniscrew insertion angles in Dravidian population-A cone beam computed tomography study[J]. Int Orthod, 2020, 18(1): 105-114. |
| [21] | 仲伟洁,叶俊杰,王华,等. 不同垂直骨面型成年患者颧牙槽嵴有效骨量的CBCT研究[J]. 口腔医学, 2021, 41 (12): 1077-1080. |
| Zhong W J, Ye J J, Wang H, et al. CBCT analysis of bone thickness of vgomatic crest in adults with different vertical skeletal patterns[J]. Stomatology, 2021,41(12):1077-1080. | |
| [22] | Tavares A, Montanha-Andrade K, Cury P R, et al. Tomographic assessment of infrazygomatic crest bone depth for extra-alveolar miniscrew insertion in subjects with different vertical and sagittal skeletal patterns[J]. Orthod Craniofac Res, 2022, 25(1): 49-54. |
| [23] | Matias M, Flores-Mir C, Almeida M R, et al. Miniscrew insertion sites of infrazygomatic crest and mandibular buccal shelf in different vertical craniofacial patterns: a cone-beam computed tomography study[J]. Korean J Orthod, 2021, 51(6): 387-396. |
| [24] | Du B R, Zhu J Y, Li L T, et al. Bone depth and thickness of different infrazygomatic crest miniscrew insertion paths between the first and second maxillary molars for distal tooth movement: a 3-dimensional assessment[J]. Am J Orthod Dentofacial Orthop, 2021, 160(1): 113-123. |
| [25] | Reiser G M, Rabinovitz Z, Bruno J, et al. Evaluation of maxillary sinus membrane response following elevation with the crestal osteotome technique in human cadavers[J]. Int J Oral Maxillofac Implants, 2001, 16(6): 833-840. |
| [1] | Xie Yixia, Wang Fan, Liu Xirui, Chen Ningning, Zhang Wenxuan, Wu Jialin, Ma Ting, Hong Wu. Overview of mechanisms of adult major depressive disorder comorbid attention deficit hyperactivity disorder and the prospects of transcranial direct current stimulation [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(1): 107-114. |
| [2] | CHEN Siyue, LI Sitong, GU Kaijun, DU Changxin, ZHU Yanfei, ZHENG Chao, ZHOU Jing, HE Ying, ZHU Min. Analysis of dentofacial characteristics in Han Chinese adults with facial harmony [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(3): 317-323. |
| [3] | LI Lulu, WU Jianyong. A cone-beam computed tomographic study comparing characteristics of maxillary anterior regional alveolar bone remodeling under two reference systems [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(11): 1507-1514. |
| [4] | MA Zhuoran, YUAN Ancai, JIANG Huiru, CHEN Xiaoyu, ZHANG Wei, PU Jun. Meta analysis of correlation between lipid accumulation product and hypertension in Chinese adults [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(4): 466-473. |
| [5] | ZENG Ling-peng, ZHANG Qing, GUAN Yan-xing, LIU Shao-zheng, CHEN Qing-jie, ZHANG Qing. Diagnosis and surgical treatment of adult Merkel diverticulum with complications [J]. , 2020, 40(2): 242-. |
| [6] | JIANG Cai-xia1, ZOU Min2, JIANG Li-ping2. Characteristic analysis of 590 older adults with geriatric syndromes in Shanghai based on cluster analysis [J]. , 2018, 38(9): 1072-. |
| [7] | YU Jin-feng, HU Yun, HUANG Ming-na, CHEN Jun, MING Ye, ZHENG Lei-lei. Three-dimensional study on symmetry of the first molar and its peripheric alveolar bone in skeletal class Ⅲ patients with mandibular deviation [J]. , 2018, 38(3): 288-. |
| [8] | ZHOU Di, WU Yan, WANG Yun-ji, FAN Xiao-ping. Comparison of alveolar bone changes in maxillary anterior area secondary to different kinds of retraction method of anterior teeth: a cone-beam computed tomography study [J]. , 2018, 38(11): 1375-. |
| [9] | SHI Yong-heng, LONG Man-mei, LIU Qiang, CHEN Xiao-yu. Clinicopathologic features of 9 cases of adult rhabdomyosarcoma#br# [J]. , 2017, 37(7): 1015-. |
| [10] | TU Yang*, WANG Ran*, GUO Ru-ru, WANG Su-li, FU Qiong, Lü Liang-jing. Clinical characteristics of patients with macrophage activation syndrome secondary to adult-onset Still’s disease [J]. , 2017, 37(6): 780-. |
| [11] | CHEN Jie, WANG Hao-ran, FANG Chao, LIU Min . Study of pituitary glands in normal adults by high-resolution MRI [J]. , 2017, 37(5): 670-. |
| [12] | GAO Mei-chun, LU Qin-chi. Systematic analysis of adults with hemophagocytic lymphohistiocytosis and combined with central nervous system #br# involvement [J]. , 2015, 35(11): 1671-. |
| [13] | LU Jun, HOU Xu-hong, JIA Wei-ping. Advances of pathogenesis of latent autoimmune diabetes in adults [J]. , 2014, 34(4): 546-. |
| [14] | ZHOU Li-jia, WU Jian-yong. Effects of stem cells on kidney repair after acute kidney injury [J]. , 2014, 34(3): 393-. |
| [15] | ZHANG Zhen-chao, ZENG An, HAN Xiao-shuai, et al. HDAC1 determines adult stem cell maintenance in planarian [J]. , 2013, 33(9): 1202-. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||