Journal of Shanghai Jiao Tong University (Medical Science) ›› 2024, Vol. 44 ›› Issue (5): 560-566.doi: 10.3969/j.issn.1674-8115.2024.05.003
• High-risk?pregnancy column • Previous Articles Next Articles
LI Yu1,2( ), ZHANG Yu1()
), ZHANG Yu1()
Received:2023-03-21
Accepted:2024-04-18
Online:2024-05-28
Published:2024-05-28
Contact:
ZHANG Yu
E-mail:fyyly2326@126.com;rjzhangyu@163.com
CLC Number:
LI Yu, ZHANG Yu. Analysis of risk factors of adverse pregnancy outcomes in patients with chronic kidney disease[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(5): 560-566.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2024.05.003
| Item | Type of nephritis | |||
|---|---|---|---|---|
| Chronic nephritis | IgA nephropathy | Lupus nephritis | Nephrotic syndrome | |
| Number of delivery/n(%) | 201 (56.94) | 99 (28.05) | 39 (11.05) | 14 (3.97) |
| Maternal outcome/n(%) | ||||
| PE | 43 (21.39) | 14 (14.14) | 11 (28.21) | 1 (7.14) |
| Severe PE | 24 (11.94) | 9 (9.09) | 9 (23.08) | 1 (7.14) |
| Acute kidney injury | 13 (6.50) | 10 (10.10) | 3 (7.69) | 3 (21.43) |
| Fetal outcome/n(%) | ||||
| Fetal loss after 20 weeks | 3 (1.49) | 3 (3.03) | 0 (0) | 1 (7.14) |
| Neonatal death | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Preterm birth | 28 (13.93) | 16 (16.16) | 22 (56.41) | 3 (21.43) |
| Preterm birth before 34weeks | 9 (4.48) | 7 (7.07) | 10 (25.64) | 3 (21.43) |
| LBWI | 18 (8.95) | 9 (9.09) | 17 (43.58) | 2 (14.29) |
| SGA | 16 (7.96) | 8 (8.08) | 8 (20.51) | 2 (14.29) |
| NICU | 19 (9.45) | 9 (9.09) | 11 (28.20) | 2 (14.29) |
Tab 1 Adverse pregnancy outcome and incidence in patients with chronic kidney disease
| Item | Type of nephritis | |||
|---|---|---|---|---|
| Chronic nephritis | IgA nephropathy | Lupus nephritis | Nephrotic syndrome | |
| Number of delivery/n(%) | 201 (56.94) | 99 (28.05) | 39 (11.05) | 14 (3.97) |
| Maternal outcome/n(%) | ||||
| PE | 43 (21.39) | 14 (14.14) | 11 (28.21) | 1 (7.14) |
| Severe PE | 24 (11.94) | 9 (9.09) | 9 (23.08) | 1 (7.14) |
| Acute kidney injury | 13 (6.50) | 10 (10.10) | 3 (7.69) | 3 (21.43) |
| Fetal outcome/n(%) | ||||
| Fetal loss after 20 weeks | 3 (1.49) | 3 (3.03) | 0 (0) | 1 (7.14) |
| Neonatal death | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Preterm birth | 28 (13.93) | 16 (16.16) | 22 (56.41) | 3 (21.43) |
| Preterm birth before 34weeks | 9 (4.48) | 7 (7.07) | 10 (25.64) | 3 (21.43) |
| LBWI | 18 (8.95) | 9 (9.09) | 17 (43.58) | 2 (14.29) |
| SGA | 16 (7.96) | 8 (8.08) | 8 (20.51) | 2 (14.29) |
| NICU | 19 (9.45) | 9 (9.09) | 11 (28.20) | 2 (14.29) |
| Item | Study group (n=123) | Control group (n=230) | P value |
|---|---|---|---|
| Age/year | 31.22±3.74 | 31.37±3.64 | 0.723 |
| BMI/(kg·m-2) | 22.74±3.57 | 21.92±2.89 | 0.058 |
| Pregnancy/n | 2 (1, 3) | 2 (1, 2) | 0.268 |
| Delivery/n | 0 | 0 | 0.630 |
| Chronic hypertension/n(%) | 20 (16.26) | 19 (8.26) | 0.022 |
| SBP/mmHg | 123 (115, 132) | 115 (108, 123) | 0.000 |
| DBP/mmHg | 79 (71, 86) | 71.5 (66, 80) | 0.000 |
| MAP/mmHg | 94 (86, 101) | 86 (80, 93) | 0.000 |
| Aspirin/n(%) | 109 (88.61) | 200 (86.96) | 0.653 |
| Immunosuppressant/n(%) | 38 (30.89) | 33 (14.35) | 0.000 |
| 24 h proteinuria≥0.3 g/n(%) | 70 (56.91) | 79 (34.35) | 0.000 |
| 24 h proteinuria≥2 g/n(%) | 57 (46.34) | 31 (13.48) | 0.000 |
| Types of nephritis/n(%) | |||
| Chronic nephritis | 68 (55.28) | 133 (57.83) | 0.646 |
| IgA nephropathy | 27 (21.95) | 72 (31.30) | 0.062 |
| Nephrotic syndrome | 4 (3.25) | 10 (4.35) | 0.615 |
| Lupus nephritis | 24 (19.51) | 15 (6.52) | 0.000 |
Tab 2 Comparison of the clinical characteristics before 20 weeks of gestation between the 2 groups
| Item | Study group (n=123) | Control group (n=230) | P value |
|---|---|---|---|
| Age/year | 31.22±3.74 | 31.37±3.64 | 0.723 |
| BMI/(kg·m-2) | 22.74±3.57 | 21.92±2.89 | 0.058 |
| Pregnancy/n | 2 (1, 3) | 2 (1, 2) | 0.268 |
| Delivery/n | 0 | 0 | 0.630 |
| Chronic hypertension/n(%) | 20 (16.26) | 19 (8.26) | 0.022 |
| SBP/mmHg | 123 (115, 132) | 115 (108, 123) | 0.000 |
| DBP/mmHg | 79 (71, 86) | 71.5 (66, 80) | 0.000 |
| MAP/mmHg | 94 (86, 101) | 86 (80, 93) | 0.000 |
| Aspirin/n(%) | 109 (88.61) | 200 (86.96) | 0.653 |
| Immunosuppressant/n(%) | 38 (30.89) | 33 (14.35) | 0.000 |
| 24 h proteinuria≥0.3 g/n(%) | 70 (56.91) | 79 (34.35) | 0.000 |
| 24 h proteinuria≥2 g/n(%) | 57 (46.34) | 31 (13.48) | 0.000 |
| Types of nephritis/n(%) | |||
| Chronic nephritis | 68 (55.28) | 133 (57.83) | 0.646 |
| IgA nephropathy | 27 (21.95) | 72 (31.30) | 0.062 |
| Nephrotic syndrome | 4 (3.25) | 10 (4.35) | 0.615 |
| Lupus nephritis | 24 (19.51) | 15 (6.52) | 0.000 |
| Item | Study group (n=123) | Control group (n=230) | P value |
|---|---|---|---|
| WBC/(×109·L-1) | 9.57±2.62 | 9.19±2.29 | 0.158 |
| HB/(g·L-1) | 120.22±18.49 | 123.69±11.71 | 0.061 |
| PLT/(×109·L-1) | 237.97±66.47 | 238.05±54.92 | 0.990 |
| TSH/(mIU·mL-1) | 1.52 (0.71, 2.74) | 1.31 (0.53, 2.00) | 0.092 |
| Serum creatinine/(μmol·L-1) | 58.00 (44.00, 82.00) | 48.25 (42.77, 53.85) | 0.000 |
| Proteinuria/[mg·(24 h)-1] | 683 (326, 2 121) | 321 (177, 691) | 0.000 |
Tab 3 Comparison of the laboratory indicators before 20 weeks of gestation between the 2 groups
| Item | Study group (n=123) | Control group (n=230) | P value |
|---|---|---|---|
| WBC/(×109·L-1) | 9.57±2.62 | 9.19±2.29 | 0.158 |
| HB/(g·L-1) | 120.22±18.49 | 123.69±11.71 | 0.061 |
| PLT/(×109·L-1) | 237.97±66.47 | 238.05±54.92 | 0.990 |
| TSH/(mIU·mL-1) | 1.52 (0.71, 2.74) | 1.31 (0.53, 2.00) | 0.092 |
| Serum creatinine/(μmol·L-1) | 58.00 (44.00, 82.00) | 48.25 (42.77, 53.85) | 0.000 |
| Proteinuria/[mg·(24 h)-1] | 683 (326, 2 121) | 321 (177, 691) | 0.000 |
| Item | OR (95% CI) | P value |
|---|---|---|
| Chronic hypertension | 5.583 (2.124‒14.669) | 0.000 |
| Immunosuppressant | 2.669 (1.569‒4.540) | 0.000 |
| Serum creatinine >60 μmol/L | 5.136 (3.101‒8.507) | 0.000 |
| 24 h proteinuria | ||
| Proteinuria≥0.3 g | 2.656 (1.419‒4.971) | 0.002 |
| Proteinuria≥2 g | 8.033 (3.339‒19.331) | 0.000 |
| Types of nephritis | ||
| Lupus nephritis: chronic nephritis | 3.129 (1.541‒6.354) | 0.002 |
| IgA nephropathy: chronic nephritis | 0.733 (0.432‒1.246) | 0.252 |
| Nephrotic syndrome: chronic nephritis | 0.782 (0.237‒2.587) | 0.687 |
Tab 4 Univariate regression analysis of influencing factors of adverse pregnancy outcomes
| Item | OR (95% CI) | P value |
|---|---|---|
| Chronic hypertension | 5.583 (2.124‒14.669) | 0.000 |
| Immunosuppressant | 2.669 (1.569‒4.540) | 0.000 |
| Serum creatinine >60 μmol/L | 5.136 (3.101‒8.507) | 0.000 |
| 24 h proteinuria | ||
| Proteinuria≥0.3 g | 2.656 (1.419‒4.971) | 0.002 |
| Proteinuria≥2 g | 8.033 (3.339‒19.331) | 0.000 |
| Types of nephritis | ||
| Lupus nephritis: chronic nephritis | 3.129 (1.541‒6.354) | 0.002 |
| IgA nephropathy: chronic nephritis | 0.733 (0.432‒1.246) | 0.252 |
| Nephrotic syndrome: chronic nephritis | 0.782 (0.237‒2.587) | 0.687 |
| Item | OR (95% CI) | P value |
|---|---|---|
| Chronic hypertension | 3.385 (1.115‒10.726) | 0.031 |
| Serum creatinine >60 μmol/L | 2.828 (1.439‒5.557) | 0.003 |
| 24 h proteinuria | ||
| Proteinuria≥0.3 g | 2.234 (1.122‒4.448) | 0.022 |
| Proteinuria≥2 g | 4.904 (1.808‒13.303) | 0.002 |
| Types of nephritis | ||
| Lupus nephritis: chronic nephritis | 4.917 (1.967‒12.290) | 0.001 |
| IgA nephropathy: chronic nephritis | 0.745 (0.375‒1.478) | 0.399 |
| Nephrotic syndrome: chronic nephritis | 0.764 (0.126‒4.624) | 0.769 |
Tab 5 Multivariate regression analysis of independent risk factors of adverse pregnancy outcomes
| Item | OR (95% CI) | P value |
|---|---|---|
| Chronic hypertension | 3.385 (1.115‒10.726) | 0.031 |
| Serum creatinine >60 μmol/L | 2.828 (1.439‒5.557) | 0.003 |
| 24 h proteinuria | ||
| Proteinuria≥0.3 g | 2.234 (1.122‒4.448) | 0.022 |
| Proteinuria≥2 g | 4.904 (1.808‒13.303) | 0.002 |
| Types of nephritis | ||
| Lupus nephritis: chronic nephritis | 4.917 (1.967‒12.290) | 0.001 |
| IgA nephropathy: chronic nephritis | 0.745 (0.375‒1.478) | 0.399 |
| Nephrotic syndrome: chronic nephritis | 0.764 (0.126‒4.624) | 0.769 |
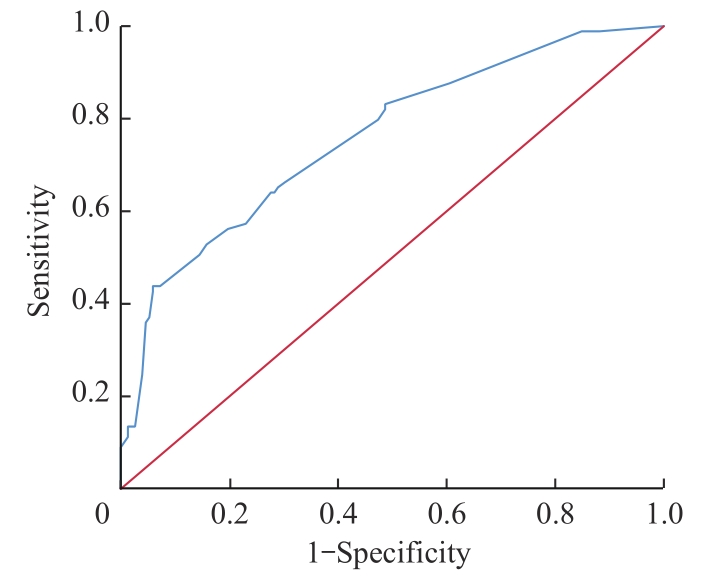
Fig 1 ROC curve of combined indicators for predicting adverse pregnancy outcomes
| 1 | 上海市肾内科临床质量控制中心专家组. 慢性肾脏病早期筛查、诊断及防治指南(2022年版)[J]. 中华肾脏病杂志, 2022, 38(5): 453-464. |
| Expert Group on Kidney Clinical Quality Control Center in Shanghai. Guidelines for early screening, diagnosis, prevention and treatment of chronic kidney disease (2022 edition)[J]. Chinese Journal of Nephrology, 2022, 38(5): 453-464. | |
| 2 | REYNOLDS M L, HERRERA C A. Chronic kidney disease and pregnancy[J]. Adv Chronic Kidney Dis, 2020, 27(6): 461-468. |
| 3 | HUI D N, HLADUNEWICH M A. Chronic kidney disease and pregnancy[J]. Obstet Gynecol, 2019, 133(6): 1182-1194. |
| 4 | PICCOLI G B, ZAKHAROVA E, ATTINI R, et al. Pregnancy in chronic kidney disease: need for higher awareness. A pragmatic review focused on what could be improved in the different CKD stages and phases[J]. J Clin Med, 2018, 7(11): 415. |
| 5 | WILES K, CHAPPELL L, CLARK K, et al. Clinical practice guideline on pregnancy and renal disease[J]. BMC Nephrol, 2019, 20(1): 401. |
| 6 | 中华医学会妇产科学分会妊娠期高血压疾病学组. 妊娠期高血压疾病诊治指南(2020)[J]. 中华妇产科杂志, 2020, 55(4): 227-238. |
| Hypertensive Disorders in Pregnancy Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association. Diagnosis and treatment of hypertension and pre-eclampsia in pregnancy: a clinical practice guideline in China(2020)[J]. Chinese Journal of Obstetrics and Gynecology, 2020, 55(4): 227-238. | |
| 7 | 国家慢性肾病临床医学研究中心, 中国医师协会肾脏内科医师分会, 中国急性肾损伤临床实践指南专家组. 中国急性肾损伤临床实践指南[J]. 中华医学杂志, 2023, 103(42): 3332-3366. |
| National Clinical Research Center for Kidney Diseases, Chinese Nephrologist Association, Expert Group on AKI Guidelines. Chinese clinical practice guideline for acute kidney injury[J]. Chinese Medical Journal, 2023, 103(42): 3332-3366. | |
| 8 | 中华医学会妇产科学分会产科学组. 早产临床防治指南(2024版)[J]. 中华妇产科杂志, 2024, 59(4): 257-269. |
| Subgroup of Obstetrics, Society of Obstetrics and Gynecology, Chinese Medical Association. Clinical guidelines for the prevention and treatment of preterm birth (version 2024)[J]. Chinese Journal of Obstetrics and Gynecology, 2024, 59(4): 257-269. | |
| 9 | NAKANO Y. Adult-onset diseases in low birth weight infants: association with adipose tissue maldevelopment[J]. J Atheroscler Thromb, 2020, 27(5): 397-405. |
| 10 | Fetal Growth Restriction: ACOG Practice Bulletin, Number 227[J]. Obstet Gynecol, 2021, 137(2): e16-e28. |
| 11 | PICCOLI G B, CABIDDU G, ATTINI R, et al. Risk of adverse pregnancy outcomes in women with CKD[J]. J Am Soc Nephrol, 2015, 26(8): 2011-2022. |
| 12 | IMBASCIATI E, GREGORINI G, CABIDDU G, et al. Pregnancy in CKD stages 3 to 5: fetal and maternal outcomes[J]. Am J Kidney Dis, 2007, 49(6): 753-762. |
| 13 | 南京总医院, 国家肾脏疾病临床医学研究中心. 慢性肾脏病患者妊娠管理指南[J]. 中华医学杂志, 2017, 97(46): 3604-3611. |
| National Clinical Research Center for Kidney Diseases, Nanjing General Hospital. Guidelines for the management of pregnancy in patients with chronic kidney disease[J]. Chinese Medical Journal, 2017, 97(46): 3604-3611. | |
| 14 | HE Y D, LI Z, CHEN S, et al. Pregnancy in patients with stage 3-5 CKD: maternal and fetal outcomes[J]. Pregnancy Hypertens, 2022, 29: 86-91. |
| 15 | CHANG C Y, CHIEN Y J, KAO M C, et al. Pre-operative proteinuria, postoperative acute kidney injury and mortality: a systematic review and meta-analysis[J]. Eur J Anaesthesiol, 2021, 38(7): 702-714. |
| 16 | WILES K, BRAMHAM K, SEED P T, et al. Serum creatinine in pregnancy: a systematic review[J]. Kidney Int Rep, 2019, 4(3): 408-419. |
| 17 | HAREL Z, MCARTHUR E, HLADUNEWICH M, et al. Serum creatinine levels before, during, and after pregnancy[J]. JAMA, 2019, 321(2): 205-207. |
| 18 | KUPER S G, TITA A T, YOUNGSTROM M L, et al. Baseline renal function tests and adverse outcomes in pregnant patients with chronic hypertension[J]. Obstet Gynecol, 2016, 128(1): 93-103. |
| 19 | DVOŘÁK J, KOUCKÝ M, JANČOVÁ E, et al. Chronic kidney disease and pregnancy outcomes[J]. Sci Rep, 2021, 11(1): 21299. |
| 20 | PICCOLI G B, ATTINI R, CABIDDU G, et al. Maternal-foetal outcomes in pregnant women with glomerulonephritides. Are all glomerulonephritides alike in pregnancy?[J]. J Autoimmun, 2017, 79: 91-98. |
| [1] | Du Xin, Li Xuebing, Li Yongwei. Research progress of macrophage metabolic reprogramming in recurrent spontaneous abortion [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(4): 537-544. |
| [2] | Ying Yiwen, Li Shu, Zhang Zhen, Yu Jingran, Zhang Ning, Mou Shan. Analysis of clinical characteristics and pregnancy outcomes of pregnancy-related acute kidney injury among high-risk pregnancy populations [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(1): 60-65. |
| [3] | MI Xiaoyang, DING Ying, CHEN Yijing, JIA Jie. Research progress in the relationship between ultra-processed food intake and pregnancy outcomes [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(1): 113-121. |
| [4] | LI Jingling, XU Xiaoyan, LI Jing, ZHOU Qian, GAO Yi, ZHOU Xuan, SHUAI Ying, LIU Hanmei. Correlation study of pregnancy stress, pre-pregnancy health care behavior and coping style of pregnant women [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(8): 968-974. |
| [5] | LU Xingyu, XU Yidan, LIU Yiqin, ZHANG Qianren, DONG Yan. Effect of high-fat diet on adipose tissues structure and inflammatory characteristics during pregnancy in mice [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(8): 981-990. |
| [6] | LU Yongjie, HOU Shuchen, CHANG Liang, LIU Ping. Impact of folic acid and active folate supplementation on red blood cell folate levels in patients with unexplained recurrent pregnancy loss and MTHFR 677TT genotype [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(6): 741-745. |
| [7] | MA Ruilin, LIU Yu, XU Guixiang, SHI Haoran, CUI Jianjian, YANG Zejun, MAO Yan, ZHAO Yin. Relationship between Doppler ultrasound parameters of uterine artery, umbilical artery, middle cerebral artery and placental vasculopathology and pregnancy outcome in preeclampsia rat model [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(5): 543-551. |
| [8] | LI Ping, JIANG Huiru, YE Mengyue, WANG Yayu, CHEN Xiaoyu, YUAN Ancai, XU Wenjie, DAI Huimin, CHEN Xi, YAN Xiaoxiang, TU Shengxian, ZHENG Yuanqi, ZHANG Wei, PU Jun. Analysis of epidemiological characteristics of risk factors for cardiovascular diseases and malignant tumors based on the Shanghai community elderly cohort [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(5): 617-625. |
| [9] | WU Lirong, CHEN Ruihua, CHAO Xiaowen, GUO Yuhuai, SUN Tao, LI Mengci, CHEN Tianlu. Study of metabolic association between elevated fasting blood glucose and cognitive deterioration [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(2): 212-222. |
| [10] | HUANG Qin, HUANG Ying, LI Wen. Timing of ultrasonography in the diagnosis of fallopian tubal heterotopic pregnancy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(12): 1545-1551. |
| [11] | SHEN Li, HUANG Hengye, YU Guangjun. Current status of neurodevelopmental outcomes and its influencing factors of early-to-moderate preterm infants at corrected age of 18 months [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(4): 445-452. |
| [12] | JIANG Jing, BIAN Yong, ZHENG Jijian, HUANG Yue. Factors influencing the amount of blood loss in pediatric patients during craniosynostosis surgery [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(4): 453-458. |
| [13] | HE Ping, SHAO Feixue, GUO Lili, LI Keting, MAO Xiaoyuan, BAO Yirong, WANG Lei. Preliminary study of pelvic floor structural changes in early and middle pregnant women with cervical incompetence [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(4): 459-465. |
| [14] | LU Ruoyu, KANG Wenhui, ZHAO Anda, LU Zhaohui, LI Shenghui. Research progress on the association between melatonin and hypertensive disorder complicating pregnancy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(10): 1297-1303. |
| [15] | XUE Linlin, LI Binghan, CHANG Lixian, LI Weikun, LIU Chunyun, LIU Li. Construction and evaluation of a nomogram prediction model for bacterial infection in patients with decompensated hepatitis C cirrhosis [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(1): 52-60. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||