Current status of neurodevelopmental outcomes and its influencing factors of early-to-moderate preterm infants at corrected age of 18 months
SHEN Li,1,2, HUANG Hengye,1, YU Guangjun,3
1.Shanghai Jiao Tong University School of Public Health, Shanghai 200025, China
2.Clinical Research Center, Shanghai Sixth People's Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200233, China
3.Children's Precision Medicine Engineering Technology Research Center, Shanghai Children's Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai 200040, China
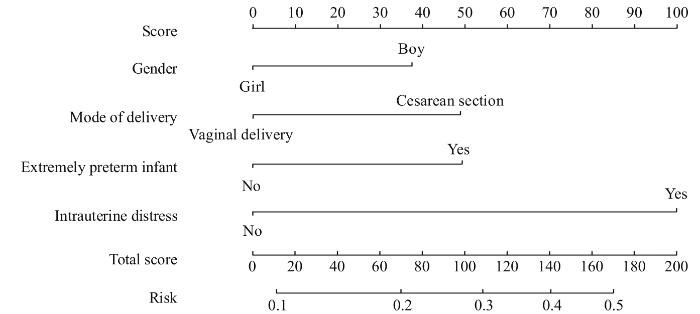
目的·了解出生胎龄≤34周的早中期早产儿在校正月龄18个月时的神经发育状况并分析其影响因素。方法·选取2013年1月—2020年4月在上海市儿童医院重症监护中心住院,并在出院后进行规律随访的早中期产儿作为研究对象。收集早产儿及其父母的人口学特征和临床相关资料。根据校正月龄18个月时的格塞尔发育量表(Gesell Development Schedule,GDS)结果,将早产儿分为神经发育正常组和神经发育迟缓组。比较2组在早产儿基本人口学特征、出生情况、父母亲基本人口学特征和产检情况方面的差异,采用逐步Logistic回归探讨早产儿神经发育迟缓的影响因素。结果·共调查了929例早产儿,其中男童527例(56.7%)、女童402例(43.3%),平均胎龄为(31.06±2.23)周,极早早产儿138例(14.9%)。在校正月龄18个月时,发生神经发育迟缓共147例(15.8%),在粗动作能、细动作能、言语能、应物能和应人能的异常率分别为7.4%、9.7%、17.9%、14.2%和13.7%。对神经发育迟缓组和正常组的临床特征进行比较发现,性别、是否为极早早产儿、出生体质量、分娩方式和是否发生宫内窘迫在2组间的差异有统计学意义(均P<0.05)。逐步Logistic回归分析的结果显示,男童(OR=1.60,95%CI 1.05~2.44,P=0.028)、剖宫产分娩(OR=1.67,95%CI 1.08~2.60,P=0.022)、极早早产儿(OR=2.20,95%CI 1.34~3.62,P=0.002)和发生宫内窘迫(OR=5.03,95%CI 2.11~11.99,P=0.000)是早中期早产儿神经发育迟缓的危险因素。结论·男童、极早早产儿、剖宫产分娩和发生宫内窘迫的早中期早产儿发生神经发育迟缓的可能性较高,应重点关注和加强这类早产儿的随访管理。
关键词:早产儿
;
神经发育
;
神经发育迟缓
;
危险因素
;
格塞尔发育量表
Abstract
Objective ·To analyze the neurodevelopmental outcomes and risk factors of early-to-moderate preterm infants with gestational age≤34 weeks at corrected age of 18 months. Methods ·The early-to-moderate preterm infants hospitalized in Neonatal Intensive Care Unit of Shanghai Children's Hospital from January 2013 to April 2020, and regularly followed up after discharge were included in this study. Demographic and clinically relevant data of preterm infants and their parents were collected. The infants were divided into the neurodevelopmental retardation group and the normal neurodevelopment group according to their Gesell Development Schedule (GDS) scores at corrected age of 18 months. The demographic characteristics of preterm infants, birth status, demographic characteristics of parents and prenatal examinations between the two groups were compared, and stepwise Logistic regression was used to explore the factors influencing neurodevelopmental outcomes in preterm infants. Results ·A total of 929 preterm infants were included in the study, including 527 boys (56.7%) and 402 girls (43.3%), with a mean gestational age of (31.06±2.23) weeks and 138 (14.9%) extremely preterm infants. A total of 147 infants (15.8%) had neurodevelopmental retardation of early-to-moderate preterm infants at corrected age of 18 months, with abnormalities of 7.4%, 9.7%, 17.9%, 14.2% and 13.7% in gross motor, fine motor, language, adaptive behavior and personal-social behavior, respectively. A comparison of the clinical characteristics between the neurodevelopmental retardation group and the normal neurodevelopment group revealed statistically significant differences in terms of gender, whether the baby was an extremely preterm infant, birth weight, mode of delivery, and occurrence of intrauterine distress (all P<0.05). Stepwise Logistic regression analysis showed that boys (OR=1.60, 95%CI 1.05‒2.44, P=0.028), cesarean section (OR=1.67, 95%CI 1.08‒2.60, P=0.022), extremely preterm infants (OR=2.20, 95%CI 1.34‒3.62, P=0.002) and intrauterine distress (OR=5.03, 95%CI 2.11‒11.99, P=0.000) were the risk factors for neurodevelopmental retardation. Conclusion ·Boys, extremely preterm infants, cesarean section and intrauterine distress may increase the neurodevelopmental retardation risk of early-to-moderate preterm infants and improving follow-up management of these preterm infants should be focused on and enhanced.
SHEN Li, HUANG Hengye, YU Guangjun. Current status of neurodevelopmental outcomes and its influencing factors of early-to-moderate preterm infants at corrected age of 18 months. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(4): 445-452 doi:10.3969/j.issn.1674-8115.2023.04.006
在早产儿校正月龄18个月时,采用格塞尔发育量表(Gesell Development Schedule,GDS)[6]进行评估,包括粗动作能、细动作能、应物能、言语能和应人能5个能区。每个能区测试结果以发育商(development quotient,DQ)表示,当DQ≥86分为发育正常,≤85分为发育异常。
Tab 2 Comparison of clinical variables for parents of preterm infants between the normal neurodevelopment group and the neurodevelopmental retardation group
SHEN Li performed the statistical analysis and drafted the manuscript. HUANG Hengye and YU Guangjun were responsible for the study design and revised the manuscript. All the authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
COMPETING INTERESTS
All authors disclose no relevant conflict of interests.
PIERRAT V, MARCHAND-MARTIN L, MARRET S, et al. Neurodevelopmental outcomes at age 5 among children born preterm: EPIPAGE-2 cohort study[J]. BMJ, 2021, 373: n741.
WANG H Q, YAO B Z. Progress of neurodevelopmental characteristics and clinical diagnosis and treatment in premature infants[J]. Chinese Journal of Child Health Care, 2021, 29(8): 877-880.
FERNÁNDEZ DE GAMARRA-OCA L, OJEDA N, GÓMEZ-GASTIASORO A, et al. Long-term neurodevelopmental outcomes after moderate and late preterm birth: a systematic review[J]. J Pediatr, 2021, 237: 168-176.e11.
ZHANG L J, WANG Y L. Clinical analysis of 198 cases of early-to-moderate preterm birth[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2007, 27(7): 850-852.
BAUD O, TROUSSON C, BIRAN V, et al. Association between early low-dose hydrocortisone therapy in extremely preterm neonates and neurodevelopmental outcomes at 2 years of age[J]. JAMA, 2017, 317(13): 1329-1337.
SHEN L, TIAN Y, YU G J, et al. Analysis of the neurodevelopment and its influencing factors of high-risk infants in Shanghai[J]. Chinese Journal of Child Health Care, 2019, 27(4): 366-369.
CHAWLA S, NATARAJAN G, SHANKARAN S, et al. Association of neurodevelopmental outcomes and neonatal morbidities of extremely premature infants with differential exposure to antenatal steroids[J]. JAMA Pediatr, 2016, 170(12): 1164-1172.
XU S S, HUANG H, ZHANG J S. Progress in the study and application of diagnostic developmental scales for infants and toddlers[J]. Chinese Journal of Child Health Care, 2010, 18(11): 859-861.
The Editorial Board of Chinese Journal of Pediatrics, The Group of Neonatology, Society of Pediatrics, Chinese Medical Association. Guidelines for management of premature infants[J]. Chinese Journal of Pediatrics, 2006, 44(3): 188-191.
NINAN K, LIYANAGE S K, MURPHY K E, et al. Evaluation of long-term outcomes associated with preterm exposure to antenatal corticosteroids: a systematic review and meta-analysis[J]. JAMA Pediatr, 2022, 176(6): e220483.
HUANG H Y. Progress in the study of neurological developmental outcomes in preterm infants[J]. Chinese Journal of Child Health Care, 2016, 24(2): 153-155.
BLENCOWE H, LEE A C, COUSENS S, et al. Preterm birth-associated neurodevelopmental impairment estimates at regional and global levels for 2010[J]. Pediatr Res, 2013, 74(Suppl 1): 17-34.
HUANG X N, ZHANG Y, FENG W W, et al. Reliability and validity of warning signs checklist for screening psychological, behavioral and developmental problems of children[J]. Chinese Journal of Pediatrics, 2017, 55(6): 445-450.
SANTOS S, FERREIRA H, MARTINS J, et al. Male sex bias in early and late onset neurodevelopmental disorders: shared aspects and differences in autism spectrum disorder, attention deficit/hyperactivity disorder, and schizophrenia[J]. Neurosci Biobehav Rev, 2022, 135: 104577.
DI ROSA G, PIRONTI E, CUCINOTTA F, et al. Gender affects early psychomotor milestones and long-term neurodevelopment of preterm infants[J]. Inf Child Dev, 2019, 28(1): e2110.
BREACH M R, LENZ K M. Sex differences in neurodevelopmental disorders: a key role for the immune system[J]. Curr Top Behav Neurosci, 2023, 62: 165-206.
PLATT M J, CANS C, JOHNSON A, et al. Trends in cerebral palsy among infants of very low birthweight (<1 500 g) or born prematurely (<32 weeks) in 16 European centres: a database study[J]. Lancet, 2007, 369(9555): 43-50.
CHEONG J L, DOYLE L W, BURNETT A C, et al. Association between moderate and late preterm birth and neurodevelopment and social-emotional development at age 2 years[J]. JAMA Pediatr, 2017, 171(4): e164805.
ZHOU F J, TU S, LIU X, et al. Study on the development of intelligence in preterm infants with different gestational ages[J]. Chinese Journal of Child Health Care, 2019, 27(4): 429-432.
LI B, FENG J J, XU X. Follow-up study on early neurodevelopment of preterm children[J]. Chinese Journal of Child Health Care, 2013, 21(5): 470-472, 476.
BELL E F, HINTZ S R, HANSEN N I, et al. Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013‒2018[J]. JAMA, 2022, 327(3): 248-263.
CHAN E, LEONG P, MALOUF R, et al. Long-term cognitive and school outcomes of late-preterm and early-term births: a systematic review[J]. Child Care Health Dev, 2016, 42(3): 297-312.
KUHLE S, TONG O S, WOOLCOTT C G. Association between caesarean section and childhood obesity: a systematic review and meta-analysis[J]. Obes Rev, 2015, 16(4): 295-303.
ZHAO Y J, CHEN Q, LIU H, et al. The association between mode of delivery and neuropsychological development of children: a birth cohort study[J]. Journal of Clinical Pediatrics, 2021, 39(7): 501-505.
ZHANG T Y, SIDORCHUK A, SEVILLA-CERMEÑO L, et al. Association of cesarean delivery with risk of neurodevelopmental and psychiatric disorders in the offspring: a systematic review and meta-analysis[J]. JAMA Netw Open, 2019, 2(8): e1910236.
SANDALL J, TRIBE R M, AVERY L, et al. Short-term and long-term effects of caesarean section on the health of women and children[J]. Lancet, 2018, 392(10155): 1349-1357.
POLIDANO C, ZHU A N, BORNSTEIN J C. The relation between cesarean birth and child cognitive development[J]. Sci Rep, 2017, 7: 11483.
BELLONO N W, BAYRER J R, LEITCH D B, et al. Enterochromaffin cells are gut chemosensors that couple to sensory neural pathways[J]. Cell, 2017, 170(1): 185-198.e16.
DIGAL K C, SINGH P, SRIVASTAVA Y, et al. Effects of delayed cord clamping in intrauterine growth-restricted neonates: a randomized controlled trial[J]. Eur J Pediatr, 2021, 180(6): 1701-1710.
LI S J, LIU W, WANG J L, et al. The role of TNF-α, IL-6, IL-10, and GDNF in neuronal apoptosis in neonatal rat with hypoxic-ischemic encephalopathy[J]. Eur Rev Med Pharmacol Sci, 2014, 18(6): 905-909.
LI T, LUO Z Q, LIU Y, et al. Excessive activation of NMDA receptors induced neurodevelopmental brain damage and cognitive deficits in rats exposed to intrauterine hypoxia[J]. Neurochem Res, 2018, 43(3): 566-580.
LIU X Q, HUANG D, WANG R Q, et al. Effects of intrauterine distress and mild neonatal asphyxia on early neurological development and physical fitness of infants[J]. Fujian Medical Journal, 2018, 40(6): 49-52.
LIU Z Y. Effect of hyperbaric oxygen therapy on behavioral neurological function and intellectual development in children with neonatal hypoxic-ischemic encephalopathy[J]. Chinese Journal of Practical Nervous Diseases, 2017, 20(4): 98-100.



{kind=link}
{kind=link}