

虽然目前的临床指南仍建议使用常规成像(conventional imaging,CI)方法,包括多参数磁共振成像(multiparametric magnetic resonance imaging,mp-MRI)和全身骨显像(bone scintigraphy,BS)对中高危PCa患者进行初始分期,但这些方法在评估PCa病情方面存在局限性。在过去10余年中,前列腺特异性膜抗原(prostate-specific membrane antigen,PSMA)作为PCa成像的优良靶点,已引起越来越多的关注。利用PSMA的正电子发射断层扫描(positron emission tomography,PET)成为了一种有价值的PCa诊断和分期方法。
PSMA是一种几乎完全由前列腺组织和肿瘤相关的新生血管产生的非分泌型Ⅱ型跨膜蛋白[3]。与正常组织相比,其在原发性和转移性PCa细胞中过度表达[4]。经过多年临床前研究,68Ga-PSMA于2012年作为PET示踪剂被引入[5],实现了基于PSMA成像的临床突破。与68Ga相比,18F因更佳的物理特性逐渐取而代之[6]。现有的18F标记的配体包括DCFBC、DCFPyL和PSMA-1007。其中,第二代低相对分子质量探针18F-DCFPyL,较第一代的DCFBC具有更高的亲和力和更高的靶本比,已获得了美国食品药品监督管理局批准[7]。本研究引入了一种在DCFPyL基础上修饰的新型PSMA特异性小分子抑制剂18F-MD-PSMA,旨在评估18F-MD-PSMA PET/CT在中高风险PCa患者的初始分期中的诊断效能。
1 对象与方法
1.1 研究对象及临床资料收集
纳入2017年9月—2022年6月在上海交通大学医学院附属新华医院核医学科就诊并接受18F-MD-PSMA PET/CT初始分期的中高危PCa病例。中高危PCa的诊断根据为美国国家综合癌症网络(National Comprehensive Cancer Network,NCCN)指南(2018版)[8]。患者在18F-MD-PSMA PET/CT检查前2周内接受CI检查,包括mp-MRI和BS;其中25例患者同期进行了18F-FDG PET/CT检查。
纳入标准:① 经穿刺后组织病理学证实的PCa。② 组织病理学Gleason评分≥7或前列腺特异性抗原(prostate-specific antigen,PSA)≥10 ng/mL。③ 在18F-MD-PSMA PET/CT检查前2周内完成mp-MRI和BS检查。排除标准:① 已接受PCa相关治疗。② 存在已知的其他恶性肿瘤。
收集患者的临床资料,包括年龄、血清PSA水平等,以及完成PSMA PET/CT检查后患者后续接受的治疗方案、血清PSA水平变化、术后病理结果(包括Gleason评分)、影像学检查随访资料(包括盆腔MRI及BS)、是否死亡及死亡原因等。
1.2 18F-MD-PSMA显像方法
18F离子在新华医院回旋加速器单元生产。使用商业合成模块FastLab™(GE Healthcare,Waukesha,美国)合成18F-MD-PSMA。检查前无需禁食。静脉注射约3.7 MBq/kg 18F-MD-PSMA,从注射结束到开始扫描的摄取时间均为1~2 h。使用Siemens Biograph-64mCT PET/CT(Siemens Healthcare,美国)在3D断层扫描仪上采集图像,每个床位2 min,视野包括头骨到股骨中部。低剂量CT扫描用于衰减校正和解剖标测,使用OSEM-3D算法对数据进行迭代重建(3次迭代,24个子集及3 mm 3D高斯滤波器)。西门子工作站用于图像读取并显示各种切面(轴向、矢状和冠状)的PET、CT和PET/CT融合图像。
1.3 影像学及病理学解读
PET/CT显像结果由2位核医学科医师双盲阅片。PET/CT阳性的标准为存在不包括生理性摄取区域在内的可见的示踪剂摄取显著增加的病灶区域。通过手动勾画感兴趣区得到最大标准化摄取值(SUVmax)。无论CT是否发现任何潜在病变,半定量标准化摄取值(SUV)比率(病变的SUVmax/周围背景中的SUV均值)用于辅助视觉分析。发现轻度局灶性摄取,则认为比率≥1.5为显著。BS结果由2位核医学科医师双盲阅片。在结合病史或其他检查排除骨良性病变所致的假阳性后,存在放射性计数明显高于或者低于健侧、邻近骨骼放射性计数的病灶,判定为骨转移阳性。在阅片出现分歧时,通过讨论达成共识。mp-MRI由一位放射科医师单独阅片。病理结果由一名病理科医师对完整的组织切片进行解读。所有阅片者对其他检验或检查结果等信息均不知情。
1.4 统计学分析
采用SPSS 27.0软件进行统计分析。正态分布的定量资料以x±s表示,采用t检验进行比较;非正态分布的定量资料以M(Q1,Q3)表示,采用秩和检验进行比较;定性资料以频数和百分比表示。计算18F-MD-PSMA PET/CT、18F-FDG PET/CT、mp-MRI、BS的灵敏度(sensitivity,SEN)、特异度(specificity,SPEC)、阳性预测值(positive predictive value,PPV)、阴性预测值(negative predictive value,NPV)及准确率(accuracy,ACU),并通过Fisher确切概率法比较2种方法诊断效能。以术后病理的T分期、N分期结果及临床随访的骨转移结果为参考标准进行Kappa一致性检验,分析18F-MD-PSMA PET/CT、CI在原发灶累及范围、区域淋巴结转移、骨转移方面与参考标准的一致性,计算Kappa系数,并进行比较。P<0.05表示差异具有统计学意义。
2 结果
2.1 患者临床特征
对67例中高危PCa患者进行了初始分期,5例(7.5%)处于中等风险,27例(40.3%)处于高风险、35例(52.2%)处于极高风险。
患者完成18F-MD-PSMA PET/CT检查后的随访时间最短为3个月,最长为64个月,中位随访时间为49.5个月。在完成18F-MD-PSMA PET/CT检查后的半年内,44例(65.7%)患者接受了根治性前列腺切除术(radical prostatectomy,Rp),经随访后获得了38例患者完整的病理学诊断资料。分别有27例和1例患者在接受了Rp的同时接受了区域淋巴结清扫术(regional lymph node dissection,RLND)和扩大盆腔淋巴结清扫术(extended pelvic lymph node dissection,ePLND),5例(7.5%)患者接受了根治性外放射治疗(external beam radiotherapy,EBRT),13例(19.4%)患者接受了雄激素剥夺治疗(androgen deprivation therapy,ADT),3例(4.5%)患者接受了化学治疗。2例患者在完成18F-MD-PSMA PET/CT检查后失访。
2.2 CI与 18F-MD-PSMA PET/CT在初始分期中的诊断性能比较
2.2.1 T分期
在18F-MD-PSMA PET/CT后半年内接受了Rp并获得了病理结果的38例PCa患者中,pT2、pT3a、pT3b、pT4分别在10、13、8、7例患者中经病理诊断证实。包膜外侵犯(extraprostatic extension,EPE)、精囊腺侵犯(seminal vesicle invasion,SVI)、膀胱颈侵犯(bladder neck invasion,BNI)分别在28、11、7例患者中经病理诊断证实。
mp-MRI、18F-FDG PET/CT、18F-MD-PSMA PET/CT对包膜内病灶的检出率分别为100.0%、57.1%、100.0%。mp-MRI和18F-MD-PSMA PET/CT诊断双侧腺叶内病灶的SEN分别为26.3%和63.2%,SPEC均为75.0%。mp-MRI、18F-MD-PSMA PET/CT诊断EPE、SVI和BNI的SEN、SPEC、PPV、NPV和ACU见表1。
表1 CI与 18F-MD-PSMA PET/CT在PCa初始分期中的诊断效能比较
Tab 1
| Organ/region examined | TP/n | FP/n | TN/n | FN/n | SEN/% | SPEC/% | PPV/% | NPV/% | ACU/% |
|---|---|---|---|---|---|---|---|---|---|
| EPE | |||||||||
| mp-MRI | 13 | 1 | 9 | 15 | 46.4 | 90.0 | 92.9 | 37.5 | 57.9 |
| 18F-MD-PSMA PET/CT | 25 | 6 | 4 | 3 | 89.3 | 40.0 | 80.6 | 57.1 | 76.3 |
| SVI | |||||||||
| mp-MRI | 3 | 2 | 25 | 8 | 27.3 | 92.6 | 60.0 | 75.8 | 73.7 |
| 18F-MD-PSMA PET/CT | 8 | 5 | 22 | 3 | 72.7 | 81.4 | 61.5 | 88.0 | 78.9 |
| BNI | |||||||||
| mp-MRI | 3 | 1 | 30 | 4 | 42.9 | 96.8 | 75.0 | 88.2 | 86.8 |
| 18F-MD-PSMA PET/CT | 3 | 0 | 31 | 4 | 42.9 | 100.0 | 100.0 | 88.6 | 86.8 |
| Regional lymph nodes (N1) | |||||||||
| Per-lesion | |||||||||
| mp-MRI | 5 | 6 | 387 | 42 | 10.6 | 98.5 | 45.5 | 90.2 | 89.1 |
| 18F-MD-PSMA PET/CT | 25 | 11 | 381 | 22 | 53.2 | 96.9 | 70.3 | 94.5 | 92.5 |
| 18F-FDG PET/CT | 12 | 6 | 213 | 32 | 29.2 | 99.5 | 66.7 | 86.7 | 87.6 |
| Per-patient | |||||||||
| mp-MRI | 3 | 0 | 17 | 8 | 27.3 | 100.0 | 100.0 | 68.0 | 71.4 |
| 18F-MD-PSMA PET/CT | 10 | 1 | 16 | 1 | 90.9 | 94.1 | 90.9 | 94.1 | 92.9 |
| 18F-FDG PET/CT | 5 | 3 | 6 | 0 | 62.5 | 96.3 | 66.7 | 100.0 | 78.6 |
| Skeleton (M1b) | |||||||||
| Per-patient | |||||||||
| BS | 13 | 2 | 32 | 3 | 81.3 | 94.1 | 86.7 | 91.4 | 90.0 |
| 18F-MD-PSMA PET/CT | 15 | 0 | 34 | 1 | 93.8 | 100.0 | 100.0 | 97.1 | 98.0 |
| Per-lesion | |||||||||
| BS | 11 | 8 | 366 | 34 | 25.0 | 97.9 | 57.9 | 91.5 | 90.0 |
| 18F-MD-PSMA PET/CT (per lesion) | 24 | 18 | 356 | 21 | 54.5 | 95.2 | 57.1 | 94.4 | 90.7 |
与病理结果进行Kappa一致性检验(表2)。mp-MRI和18F-MD-PSMA PET/CT诊断EPE的P值均为0.040,Kappa系数分别为0.251和0.324;诊断SVI的P值分别为0.100和0.001,Kappa值分别为0.237和0.514;诊断BNI的P值分别为0.002和0.000,Kappa系数分别为0.475和0.550。18F-MD-PSMA PET/CT的一致性均高于mp-MRI。Fisher确切概率法提示,2种检查方法诊断EPE、SVI的SEN(P=0.226,P=0.491)和SPEC(P=1.000,P=0.342),以及诊断BNI的SEN(均P=1.000)比较,差异均无统计学意义。
表2 mp-MRI与 18F-MD-PSMA PET/CT诊断EPE、SVI、BNI与病理结果的一致性(n)
Tab 2
| Imaging method | Pathologic diagnosis of EPE | Pathologic diagnosis of SVI | Pathologic diagnosis of BNI | |||
|---|---|---|---|---|---|---|
| + | - | + | - | + | - | |
| mp-MRI | ||||||
| + | 13 | 1 | 3 | 2 | 3 | 1 |
| - | 15 | 9 | 8 | 25 | 4 | 30 |
| 18F-MD-PSMA PET/CT | ||||||
| + | 25 | 6 | 8 | 5 | 3 | 0 |
| - | 3 | 4 | 3 | 22 | 4 | 31 |
2.2.2 N分期
27例接受RLND和1例接受ePLND的患者,共切除440枚区域淋巴结和10枚非区域淋巴结,其中47枚区域淋巴结和10枚非区域淋巴结经病理诊断证实为转移灶。
图1
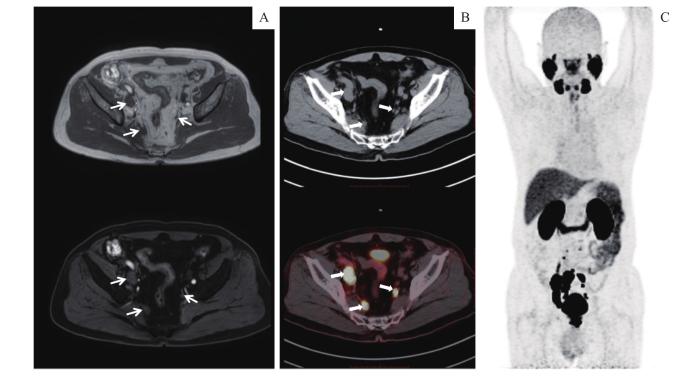
图1
一例患者mp-MRI与 18F-MD-PSMA PET/CT对盆腔淋巴结的评估结果比较
Note: A. Pelvic mp-MRI showed enlargement of the right iliac lymph nodes with abnormal signal which supported the diagnosis of metastasis lymph nodes and a small left iliac lymph node (white thin arrows). B. 18F-MD-PSMA PET/CT demonstrated abnormal 18F-MD-PSMA uptake not only at the right iliac lymph nodes, but also at the left iliac lymph node which was less than 1 cm in diameter (white thick arrows). C. Maximum intensity projection (MIP) image demonstrated more abnormal 18F-MD-PSMA uptake of metastatic lymph nodes in pelvic region.
Fig 1
Comparison of evaluation results of pelvic lymph nodes between mp-MRI and 18F-MD-PSMA PET/CT in a patient
将mp-MRI、18F-MD-PSMA PET/CT的诊断结果与病理结果进行Kappa一致性检验(表3)。基于淋巴结数量分析的P值均为0.000,18F-MD-PSMA PET/CT与病理结果的一致性高于mp-MRI(Kappa系数分别为0.555和0.137);Fisher确切概率法提示2种检查方法的SEN和SPEC比较,差异均无统计学意义(P=0.562,P=0.829)。基于患者分析的P值分别为0.023和0.000,18F-MD-PSMA PET/CT与病理结果一致性高于mp-MRI(Kappa系数分别为0.850和0.313);Fisher确切概率法提示两者的SEN比较,差异无统计学意义(P=1.000)。
表3 mp-MRI与 18F-MD-PSMA PET/CT在诊断区域淋巴结转移方面与病理结果的一致性(n)
Tab 3
| Imaging method | Pathologic diagnosis of lymph node metastasis | |
|---|---|---|
| + | - | |
| Per-patient | ||
| mp-MRI | ||
| + | 3 | 0 |
| - | 8 | 17 |
| 18F-MD-PSMA PET/CT | ||
| + | 10 | 1 |
| - | 1 | 16 |
| Per-lesion | ||
| mp-MRI | ||
| + | 5 | 6 |
| - | 42 | 387 |
| 18F-MD-PSMA PET/CT | ||
| + | 25 | 12 |
| - | 22 | 381 |
2.2.3 M分期
在50例具有完整全身骨扫描资料的PCa患者中,16例患者共419处骨病灶经临床诊断及随访综合判断为转移灶。BS、18F-MD-PSMA PET/CT诊断骨转移的SEN、SPEC、PPV、NPV和ACU见表1。其中,2例BS假阳性均为退变所致。将BS、18F-MD-PSMA PET/CT的诊断结果与临床随访结果进行Kappa一致性检验(表4)。基于骨病灶数量分析的P值均为0.000,18F-MD-PSMA PET/CT与随访结果的一致性高于BS(Kappa系数分别为0.500和0.299);Fisher确切概率法提示2种检查方法的SEN比较,差异无统计学意义(P=0.219)。基于患者分析的P值均为0.000,18F-MD-PSMA PET/CT与随访结果的一致性高于BS(Kappa系数分别为0.953和0.766);Fisher确切概率法提示2种检查方法的SEN差异无统计学意义(P=1.000)。
表4 BS与 18F-MD-PSMA PET/CT在诊断骨转移方面与临床随访结果的一致性(n)
Tab 4
| Imaging method | Clinical diagnosis of bone metastasis | |
|---|---|---|
| + | - | |
| BS | ||
| + | 11 | 8 |
| - | 34 | 366 |
| 18F-MD-PSMA PET/CT | ||
| + | 24 | 18 |
| - | 21 | 356 |
2.3 18F-MD-PSMA PET/CT在评估病情中的价值
2.3.1 18F-MD-PSMA PET/CT对风险分层的评估
67例中高危患者,经18F-MD-PSMA PET/CT检查,21例(31.3%)患者的风险分层上升,其中有9例(13.4%)和12例(17.9%)患者分别从中危升级为高危、从高危升级为极高危;另有1例(1.5%)患者的风险分层下降(MRI误诊了SVI)。
2.3.2 18F-MD-PSMA PET/CT对初始分期的评估
67例中高危患者,经18F-MD-PSMA PET/CT检查,38例(56.7%)患者T期上调,15例(22.4%)患者N期上调,13例(19.4%)患者M期上调。32例患者(47.8%)患者的初始分期发生了改变,其中27例(40.3%)上调,5例(7.5%)下调。分期下调是因为经临床判断,3例患者的MRI或BS对骨转移的判断结果呈假阳性,2例患者18F-MD-PSMA PET/CT对骨转移的结果判断呈假阴性。其余35例(52.2%)患者的初始分期没有发生改变。9例(13.4%)患者新发现了区域淋巴结转移,4例(6.0%)新发现了非区域淋巴结转移,9例(13.4%)新发现了骨转移,13例(19.4%)骨转移的患者发现其他骨转移灶(其中5例由寡转移变为多发骨转移,见图2),1例(1.5%)新发现了肺转移。
图2
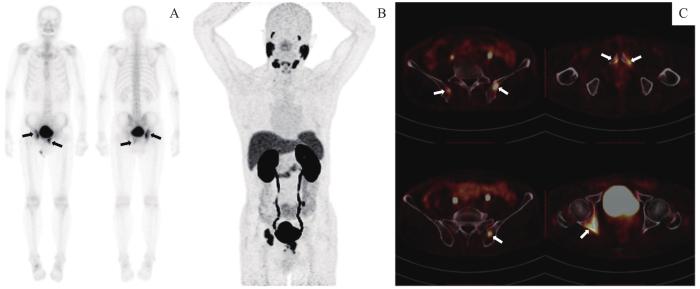
图2
一例患者BS与 18F-MD-PSMA PET/CT评估结果比较
Note: A. BS image demonstrated oligometastasis status with 2 lesions in right hip joint and left pubic bone (black arrows). B. MIP image of 18F-MD-PSMA PET/CT demonstrated 6 lesions with high 18F-MD-PSMA uptake. C. Fusion images of PET and CT showed abnormal high uptake of 18F-MD-PSMA at bilateral ilium, right acetabulum and bilateral pubis (white arrows).
Fig 2
Comparison of evaluation results of BS and 18F-MD-PSMA PET/CT in a patient
对67例患者在完成18F-MD-PSMA PET/CT初始分期后进行了预后随访,其中4例(6.0%)发生了生化复发,6例(9.0%)发生了影像学进展,5例(7.5%)因PCa并发症死亡。在27例初始分期上调的患者中,仅1例(3.7%)患者在随访过程中发生了生化复发、影像学进展及死亡事件。
3 讨论
PCa的术前分期对病情的评估、治疗方案的选择具有重要的参考价值。目前,mp-MRI和BS作为术前分期的常规成像方法在临床应用中仍具有局限性,各研究变异性较大,SEN及ACU也普遍偏低。
METSER等[9]从病变水平对55例怀疑PCa的男性患者进行分析,发现mp-MRI对于原发灶检测的SEN为67%。SONNI等[10]的研究对425个PCa病灶节段进行分析,发现mp-MRI对包膜内病灶的检出率仅为35%。DONATO等[11]对58例男性的回顾性队列研究发现,mp-MRI在诊断前列腺内病灶的ACU为69%,检测单灶病变的SEN为90%,而诊断双侧和多灶性病变的SEN仅为21%和19%。在检测EPE方面,mp-MRI的SEN为35.0%~66.2%,SPEC为89.0%~92.0%[12-13]。而另一项对50例PCa患者的前瞻性研究[14]显示,mp-MRI检测EPE的SEN、SPEC、PPV、NPV及ACU分别为76.5%~94.1%、45.5%~84.9%、43.8%~76.2%、83.3%~96.6%和58.0%~88.0%,在检测SVI方面分别为57.1%~85.7%、86.1%~97.7%、40.0%~85.7%、92.5%~97.7%和82.0%~96.0%。
近年来,PSMA PET/CT在PCa中的应用越来越受到重视。本研究报道了在中高危PCa中使用18F-MD-PSMA PET/CT进行初始分期的单中心初步经验。精确的T分期有助于为PCa患者选择合适的治疗方案。本研究结果显示,18F-MD-PSMA PET/CT对双侧疾病的诊断较mp-MRI具有更高的SEN(分别为63.2%和26.3%),该结果与较多相关研究结果基本吻合[9,11,15]。然而,在诊断EPE、SVI方面,多项研究[10,15-16]提示mp-MRI较PSMA PET/CT具有更大的优势,与本研究的结果相反。可能的原因包括:① 研究人群的风险分层存在差异。本研究中高危人群高达92.5%,而部分报道中的研究对象以低中危为主[15,17]。② 与更高物理空间分辨率的18F及更高亲和力和靶本比的新型小分子抑制剂18F-MD-PSMA的使用有关。③ 本研究中,为显示更大的盆腔范围,部分患者以普通盆腔MRI代替前列腺mp-MRI,这也是本研究的缺陷之一。在诊断BNI方面,mp-MRI及18F-MD-PSMA PET/CT在本研究中的表现相近,与其他研究的结论相符[15,18]。
术前准确检测淋巴结转移,有助于N1期患者清除转移性淋巴结而减少肿瘤负荷,同时也可以减少不必要的ePLND,降低因侵入性操作带来的并发症风险。据研究,PSMA PET/CT诊断区域淋巴结转移的SEN为33.3%~84.0%,SPEC为82.0%~100.0%,ACU为88.5%~95.2%,MRI分别为27.3%~43.9%、85.4%~97.1%和72.3%~87.6%[19-23]。总体上,2种方法检测区域淋巴结转移时都表现出较低的SEN及较高的SPEC,但PSMA PET/CT更具优势[15,21]。本研究得出了相似的结果,18F-FDG PET/CT则介于两者之间。这可能是由于传统的影像学检查具有一定的局限性,通常以淋巴结的大小作为评估转移的标准。当病理性淋巴结表现出异常的解剖特征,如形态呈非椭圆形或短轴直径超过1 cm时,MRI通常可以识别。对于直径小于1 cm的淋巴结,MRI较难作出有效诊断。尽管大小及形态未见异常,PSMA PET/CT示踪剂对转移性淋巴结的特异性亲和力使之可视化。这种特点使18F-MD-PSMA PET/CT检测转移性淋巴结的SEN显著高于MRI,但其假阳性率也更高。这可能是由示踪剂经肾脏排泄,在输尿管走形区的浓聚造成的。另外,本研究中有部分患者经18F-MD-PSMA PET/CT检查发现非区域淋巴结转移,并经ePLND得到病理学证实,而18F-FDG PET/CT表现为阴性。18F-MD-PSMA PET/CT使这类患者获得了进一步减少肿瘤负荷的机会。
远处转移状态对PCa患者治疗方案的确定至关重要。对于骨病灶来说,较难通过活检明确,因此检查准确率的提高有助于临床对可疑骨病灶的诊断。本研究结果显示,18F-MD-PSMA PET/CT在诊断骨转移方面,较传统成像方法具有明显的优势,其SEN、SPEC、PPV、NPV和ACU均高于BS,这一结果与大部分研究结果相吻合[24-26]。在我国,由于PSA筛查尚未全面普及,初诊即诊断为局部晚期或存在转移性病变的比例较高,预后也普遍较差。传统上,包括Rp和根治性放疗在内的局部治疗仅用于治疗局限性PCa;而对于有转移证据的患者,即使是单个盆腔淋巴结阳性,也意味着失去了积极治疗机会,大多接受ADT联合化学治疗进行系统性、姑息性的治疗。然而,近年来的研究提出了寡转移PCa(oligometastatic prostate cancer,OPC)的概念。骨或淋巴结转移灶数量≤5个(即寡转移)的患者,通过对其原发灶及转移灶进行局部治疗,能使寡转移状态在较长时间内维持稳定[27-29]。本研究中的2例BS呈假阳性后,经随访证实均由退变造成。另外,还有5例由CI评估为寡转移的患者,经PSMA PET/CT评估为多发骨转移。本研究认为,18F-MD-PSMA PET/CT的应用有利于寡转移患者得到局部治疗的机会,也避免了无意义的手术或局部治疗给多发转移的患者带来的损伤。
18F-MD-PSMA PET/CT的局限性表现在以下几个方面。第一,阳性PSMA成像是基于转移灶中PSMA的表达,但事实上并不是所有的转移灶都有PSMA表达,因此存在假阴性的可能性。第二,如果转移灶过小,尽管有PSMA摄取,但分辨率的限制使病变不可见。第三,由于尿液放射性的影响,PSMA PET/CT成像较难清晰地判断膀胱颈、输尿管或其他邻近组织的累及,而在软组织分辨率方面又不及MRI。
本研究还存在以下潜在缺陷。由于实际和伦理问题,某些淋巴结及骨转移灶的病理学证实不可行,骨转移只能通过对每个病灶的纵向随访而得到证实,无法将病理证实的转移性淋巴结与影像结果一一对应;研究中未能严格执行予患者前列腺mp-MRI检查,而是予以盆腔MRI检查;未能分析除骨转移(M1b)以外的其他远处转移等。
作者贡献声明
严叶青、傅宏亮参与研究设计、数据收集及整理;严叶青负责统计分析、论文撰写;梁胜、马玉飞、蔡利生参与了18F-MD-PSMA的制备;杨斌、傅宏亮、王辉参与患者招募;邹仁健负责图像采集及处理。所有作者均阅读并同意了最终稿件的提交。
YAN Yeqing and FU Hongliang contributed to the design of the study, collection and organization of the data. YAN Yeqing contributed to statistical analysis and manuscript writing. LIANG Sheng, MA Yufei and CAI Lisheng contributed to the production of 18F-MD-PSMA. YANG Bin, FU Hongliang and WANG Hui were responsible for recruiting patients. Images were collected and processed by ZOU Renjian. All authors have read the last version of paper and consented for submission.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
参考文献

{kind=link}
{kind=link}
{kind=link}
{kind=link}