上海交通大学学报(医学版) ›› 2021, Vol. 41 ›› Issue (9): 1207-1214.doi: 10.3969/j.issn.1674-8115.2021.09.011
宣贝贝1( ), 龚赛楠2, 刘佳丽2, 全权2, 孟雨2, 牟晓玲1()
), 龚赛楠2, 刘佳丽2, 全权2, 孟雨2, 牟晓玲1()
收稿日期:2021-03-26
出版日期:2021-09-28
发布日期:2021-08-24
通讯作者:
牟晓玲,电子信箱:mxl@hospital.cqmu.edu.cn。作者简介:宣贝贝(1994—),女,硕士生;电子信箱:xuanbeibei0806@163.com。
基金资助:
Bei-bei XUAN1(), Sai-nan GONG2, Jia-li LIU2, Quan QUAN2, Yu MENG2, Xiao-ling MU1()
Received:2021-03-26
Online:2021-09-28
Published:2021-08-24
Contact:
MU Xiao-ling, E-mail: mxl@hospital.cqmu.edu.cn.Supported by:摘要:
目的·探究和验证DNA聚合酶θ(DNA polymerase θ,POLQ)在子宫内膜癌和正常子宫内膜组织中的差异表达,分析其与子宫内膜癌患者临床特征的关系及对预后判断的价值。方法·应用基因表达数据动态分析(Gene Expression Profiling Interactive Analysis,GEPIA)网站检索POLQ基因在人体各部位癌组织和正常组织的表达情况。从癌症基因组图谱(The Cancer Genome Atlas,TCGA)数据库中下载POLQ基因表达谱及临床数据,经Strawberry Perl软件整理后获得基因表达矩阵,使用R软件比较癌和癌旁组织POLQ表达差异及其表达与临床特征的关系,利用基因探针富集分析(Gene Set Enrichment Analysis,GSEA)揭示POLQ在子宫内膜癌中参与的信号通路。收集127例2011年3月—2014年12月在重庆医科大学第一附属医院接受手术且组织病理学诊断为子宫内膜癌的患者的临床信息,分析不同临床特征患者间POLQ表达的差异;取这些患者的肿瘤组织石蜡切片行免疫组织化学染色,判断肿瘤组织中POLQ表达情况,并以22例子宫肌瘤患者的正常子宫内膜组织作为对照。利用Kaplan-Meier法及多因素Cox回归模型分析POLQ表达与子宫内膜癌患者预后的相关性。结果·通过GEPIA网站检索到POLQ除了在睾丸癌中相对低表达,在多数癌症中表达均升高。TCGA数据库中POLQ在子宫内膜癌组织的表达水平显著高于癌旁组织(P=0.000);POLQ在60岁及以上和高分级患者中的表达水平更高(均P<0.05),且POLQ高表达患者总生存期较短(P=0.000)。GSEA结果显示,POLQ基因主要富集在碱基切除修复通路、同源重组通路、P53通路等。POLQ在正常子宫内膜石蜡切片免疫组织化学染色评分≥1分与≥5分的比例均显著低于子宫内膜癌组织(均P<0.05);≥5分的比例在不同肿瘤分期、淋巴结转移情况的患者间差异有统计学意义(均P=0.038);且POLQ高表达患者无病生存期和总生存期均显著短于POLQ低表达组(均P<0.05)。多因素Cox分析提示POLQ评分可作为子宫内膜癌的独立预后因素。结论·相较于正常子宫内膜,POLQ在子宫内膜癌组织中表达显著升高,尤其在晚期、有淋巴结转移的患者中表达水平更高,且POLQ高表达是子宫内膜癌患者预后差的独立预测因素。
中图分类号:
宣贝贝, 龚赛楠, 刘佳丽, 全权, 孟雨, 牟晓玲. DNA聚合酶θ在子宫内膜癌中的表达及其临床意义[J]. 上海交通大学学报(医学版), 2021, 41(9): 1207-1214.
Bei-bei XUAN, Sai-nan GONG, Jia-li LIU, Quan QUAN, Yu MENG, Xiao-ling MU. Expression and clinical significance of DNA polymerase θ in endometrial cancer[J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2021, 41(9): 1207-1214.
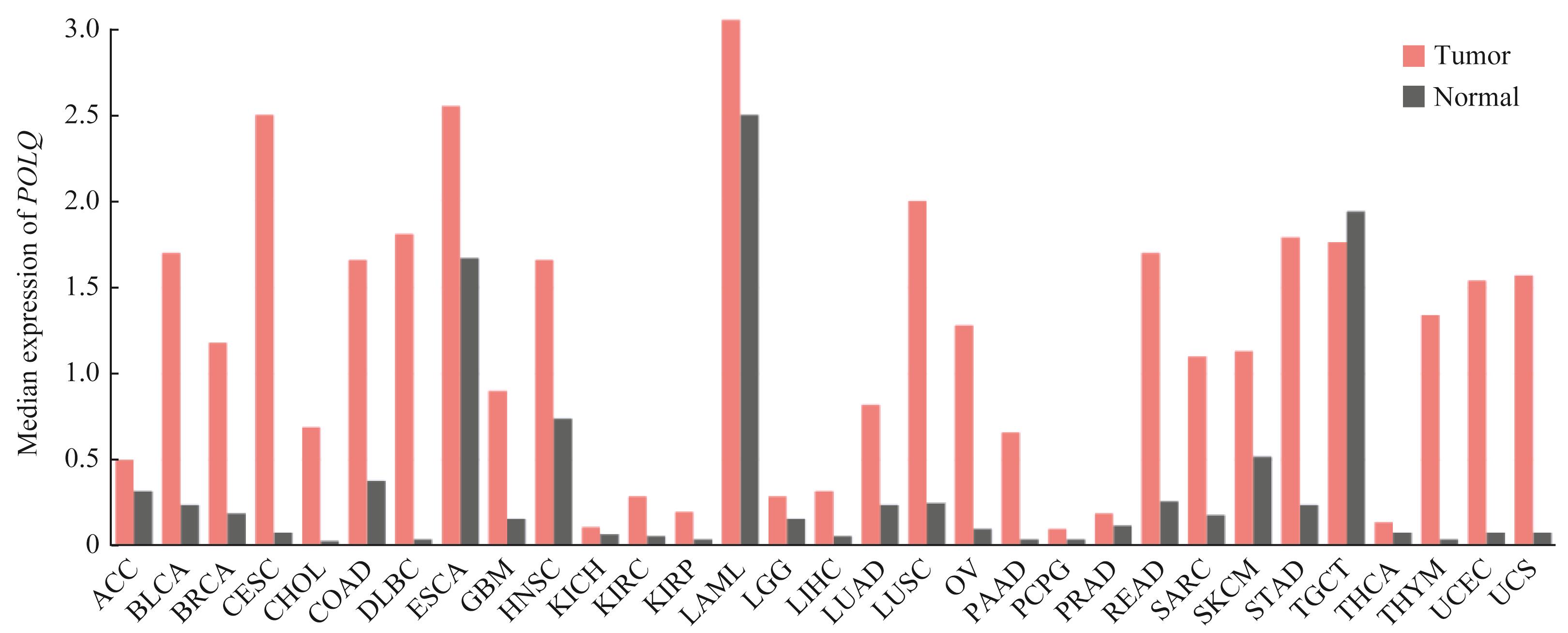
图1 POLQ在人体各系统肿瘤和正常组织中的表达情况Note: ACC—adrenocortical carcinoma; BLCA—bladder urothelial carcinoma; BRCA—breast invasive carcinoma; CESC—cervical squamous cell carcinoma and endocervical adenocarcinoma; CHOL—cholangiocarcinoma; COAD—colon adenocarcinoma; DLBC—diffuse large B-cell lymphoma; ESCA—esophageal carcinoma; GBM—glioblastoma multiforme; HNSC—head and neck squamous cell carcinoma; KICH—kidney chromophobe; KIRC—kidney renal clear cell carcinoma; KIRP—kidney renal papillary cell carcinoma; LAML—acute myeloid leukemia; LGG—brain lower grade glioma; LIHC—liver hepatocellular carcinoma; LUAD—lung adenocarcinoma; LUSC—lung squamous cell carcinoma; OV—ovarian serous cystadenocarcinoma; PAAD—pancreatic adenocarcinoma; PCPG—pheochromocytoma and paraganglioma; PRAD—prostate adenocarcinoma; READ—rectum adenocarcinoma; SARC—sarcoma; SKCM—skin cutaneous melanoma; STAD—stomach adenocarcinoma; THCA—thyroid carcinoma; THYM—thymoma; UCEC—uterine corpus endometrial carcinoma; UCS—uterine carcinosarcoma.
Fig 1 Expression of POLQ in human tumors and normal tissues
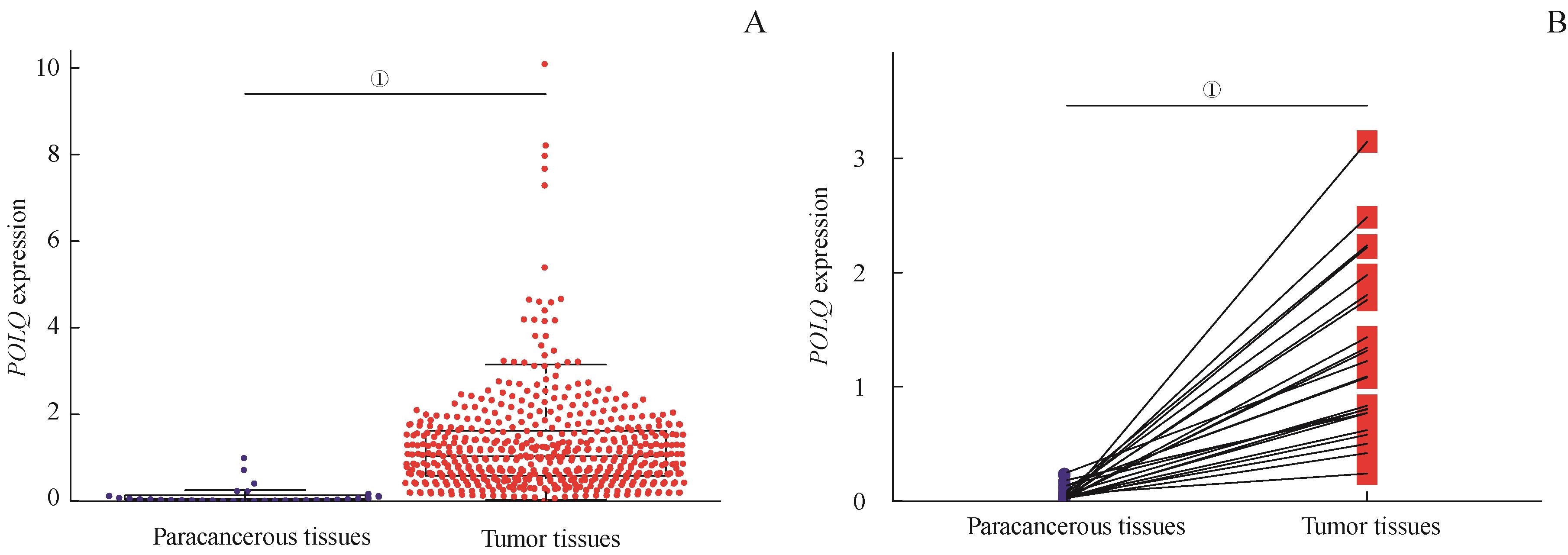
图2 TCGA-UCEC数据库中POLQ在EC组织和癌旁组织的差异表达Note: A. POLQ expression in the paracancerous and tumor tissues. B. POLQ expression in the 35 pairs of tumor and paracancerous tissues. ①P=0.000.
Fig 2 Differential expression of POLQ in the EC and paracancerous tissues in the TCGA-UCEC
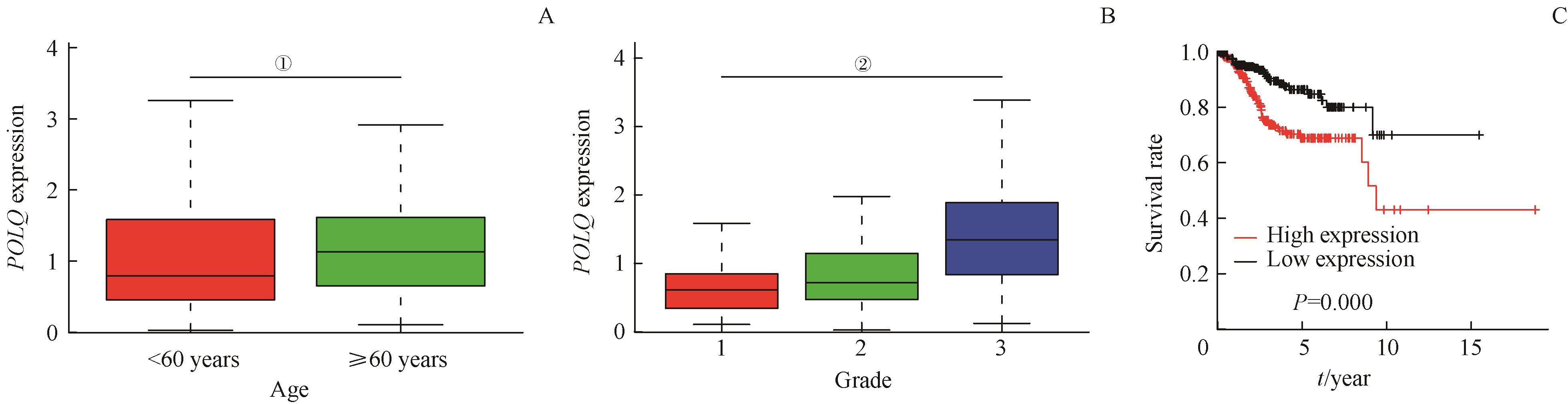
图3 TCGA-UCEC数据库中POLQ表达与患者年龄、分级以及预后的关系
Fig 3 Relationship of the POLQ expression with age, grade and prognosis of the patients in the TCGA-UCECNote:A. Comparison of POLQ expression between different ages of patients. B. Comparison of POLQ expression among different grades of patients. C. Overall survival curves of the POLQ-high expression group and -low expression group. ①P=0.003, ②P=0.000.
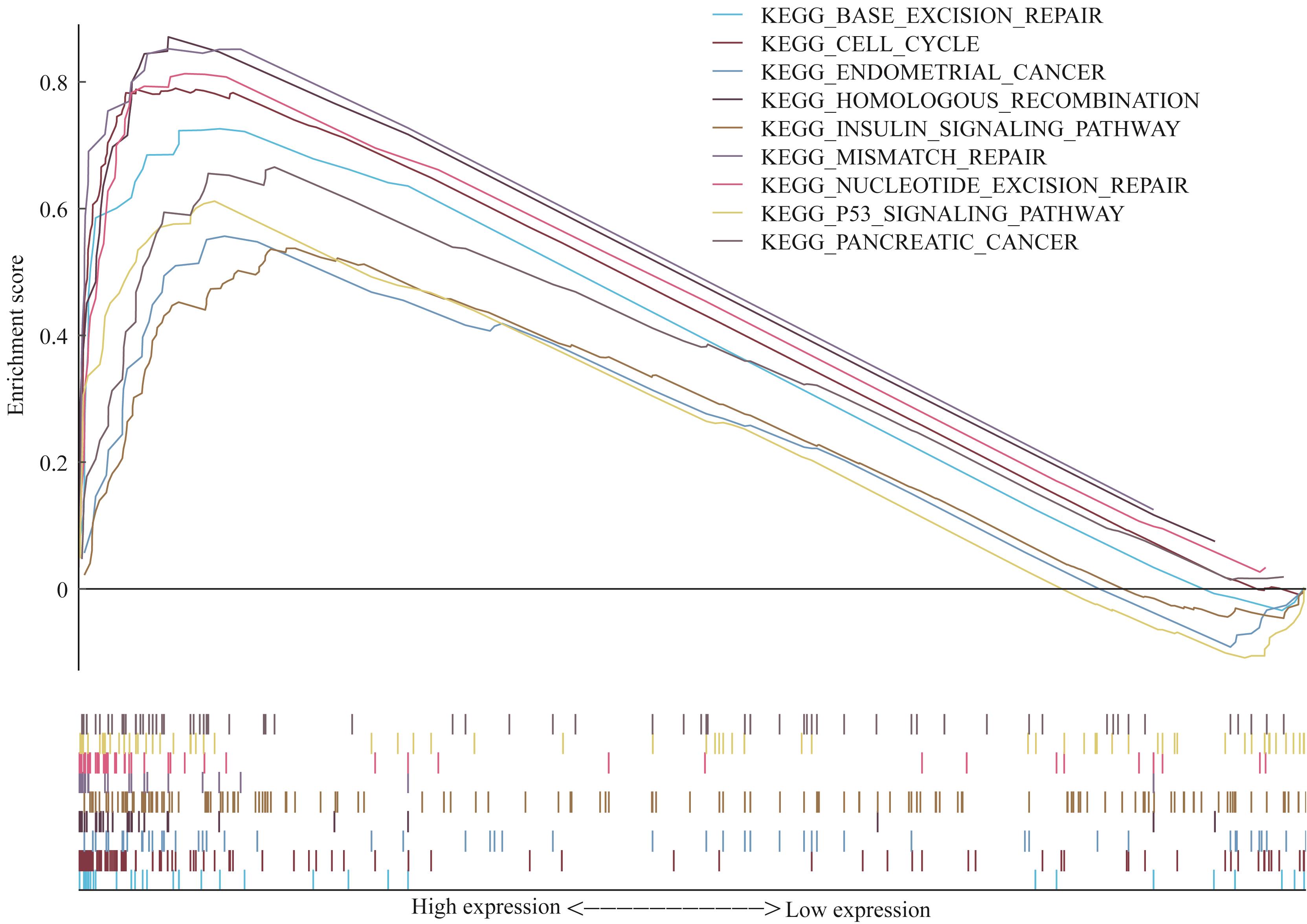
图4 EC中POLQ基因通路富集图
Fig 4 Enrichment analysis of POLQ gene pathway in EC
| Group | Total/n | Expression of POLQ/n | ≥1 score/% | ≥5 score/% | |||
|---|---|---|---|---|---|---|---|
| - | + | ++ | +++ | ||||
| EC | 127 | 9 | 54 | 38 | 26 | 92.9 | 50.4 |
| Normal endometrium | 22 | 8 | 11 | 3 | 0 | 63.6 | 13.6 |
| P value | ‒ | ‒ | ‒ | ‒ | ‒ | 0.000 | 0.001 |
表1 POLQ在正常子宫内膜与EC组织的表达情况
Tab 1 Expression of POLQ in the normal endometrium and EC tissues
| Group | Total/n | Expression of POLQ/n | ≥1 score/% | ≥5 score/% | |||
|---|---|---|---|---|---|---|---|
| - | + | ++ | +++ | ||||
| EC | 127 | 9 | 54 | 38 | 26 | 92.9 | 50.4 |
| Normal endometrium | 22 | 8 | 11 | 3 | 0 | 63.6 | 13.6 |
| P value | ‒ | ‒ | ‒ | ‒ | ‒ | 0.000 | 0.001 |
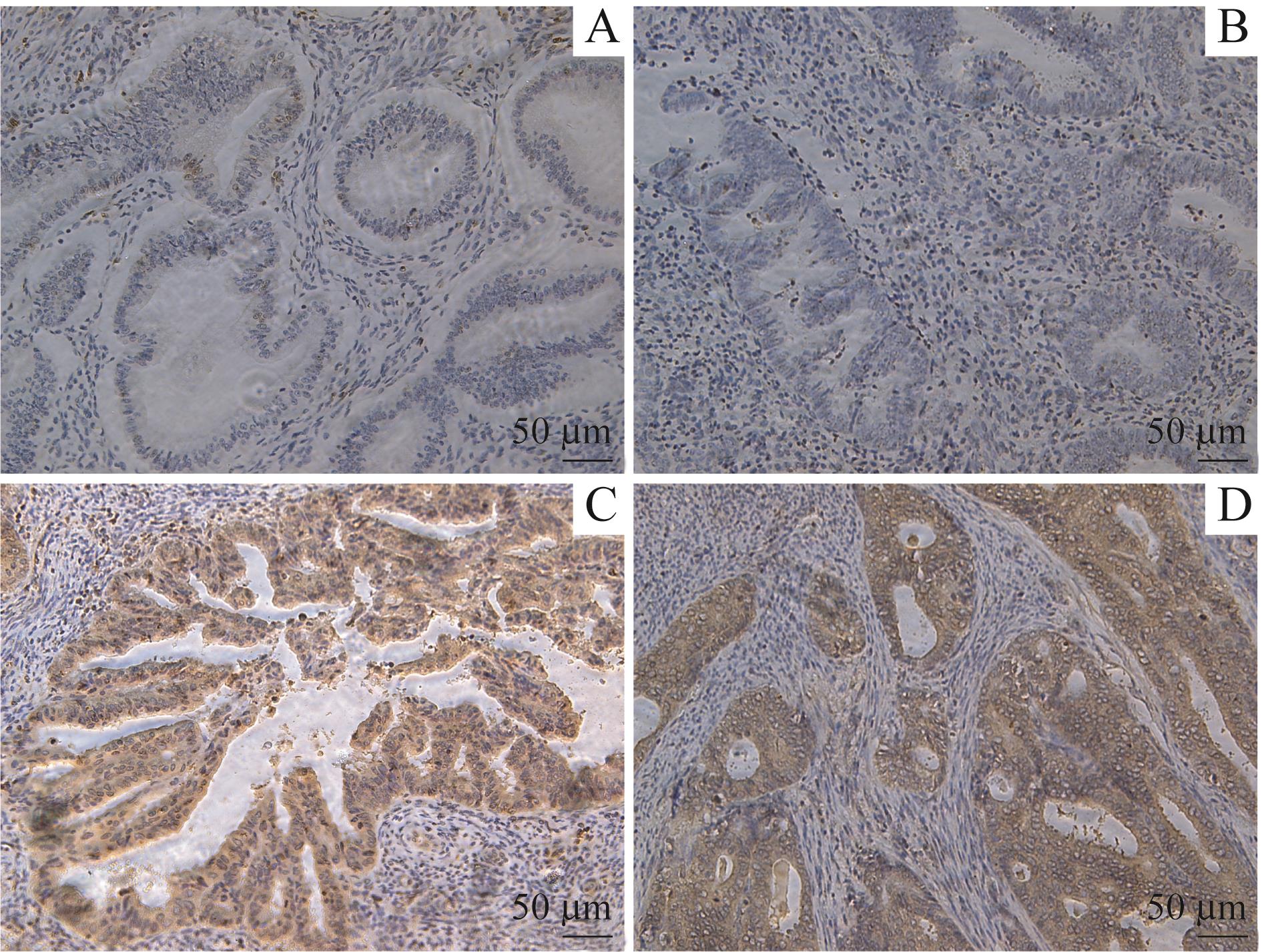
图5 正常子宫内膜和EC组织石蜡切片POLQ免疫组化染色 (×200)
Fig 5 Immunohistochemical staining of POLQ in the paraffin sections of normal endometrium and EC tissues (×200)Note:A/B. Negative or weakly positive in normal endometrium. C/D. Strongly positive in EC.
| ≥5 score/n(%) | P value | |
|---|---|---|
| Age/year | 0.246 | |
| ≥60(n=50) | 22 (44.0) | |
| <60(n=77) | 42 (54.5) | |
| Type | 0.742 | |
| Ⅰ(n=89) | 44 (49.4) | |
| Ⅱ(n=38) | 20 (52.6) | |
| Stage | 0.038 | |
| Ⅰ(n=83) | 35 (42.2) | |
| Ⅱ(n=28) | 18 (64.3) | |
| Ⅲ(n=16) | 11 (68.8) | |
| Grade | 0.533 | |
| 1(n=23) | 14 (60.9) | |
| 2(n=72) | 35 (48.6) | |
| 3(n=32) | 15 (46.9) | |
| Myometrial invasion | 0.954 | |
| Superficial(n=89) | 45 (50.6) | |
| Deep(n=38) | 19 (50.0) | |
| Lymph node metastasis | 0.038 | |
| Negative(n=121) | 49 (40.5) | |
| Positive(n=6) | 5 (83.3) | |
| Tumor size/cm | 0.154 | |
| ≥2(n=90) | 49 (54.4) | |
| <2(n=37) | 15 (40.5) | |
| ER① | 0.478 | |
| Negative(n=19) | 11 (57.9) | |
| Positive(n=104) | 51 (49.0) | |
| PR① | 0.790 | |
| Negative(n=27) | 13 (48.1) | |
| Positive(n=96) | 49 (51.0) |
表2 不同临床特征患者POLQ蛋白在EC组织中的表达情况
Tab 2 Expression of POLQ protein in the EC tissues of patients with different clinical characteristics
| ≥5 score/n(%) | P value | |
|---|---|---|
| Age/year | 0.246 | |
| ≥60(n=50) | 22 (44.0) | |
| <60(n=77) | 42 (54.5) | |
| Type | 0.742 | |
| Ⅰ(n=89) | 44 (49.4) | |
| Ⅱ(n=38) | 20 (52.6) | |
| Stage | 0.038 | |
| Ⅰ(n=83) | 35 (42.2) | |
| Ⅱ(n=28) | 18 (64.3) | |
| Ⅲ(n=16) | 11 (68.8) | |
| Grade | 0.533 | |
| 1(n=23) | 14 (60.9) | |
| 2(n=72) | 35 (48.6) | |
| 3(n=32) | 15 (46.9) | |
| Myometrial invasion | 0.954 | |
| Superficial(n=89) | 45 (50.6) | |
| Deep(n=38) | 19 (50.0) | |
| Lymph node metastasis | 0.038 | |
| Negative(n=121) | 49 (40.5) | |
| Positive(n=6) | 5 (83.3) | |
| Tumor size/cm | 0.154 | |
| ≥2(n=90) | 49 (54.4) | |
| <2(n=37) | 15 (40.5) | |
| ER① | 0.478 | |
| Negative(n=19) | 11 (57.9) | |
| Positive(n=104) | 51 (49.0) | |
| PR① | 0.790 | |
| Negative(n=27) | 13 (48.1) | |
| Positive(n=96) | 49 (51.0) |
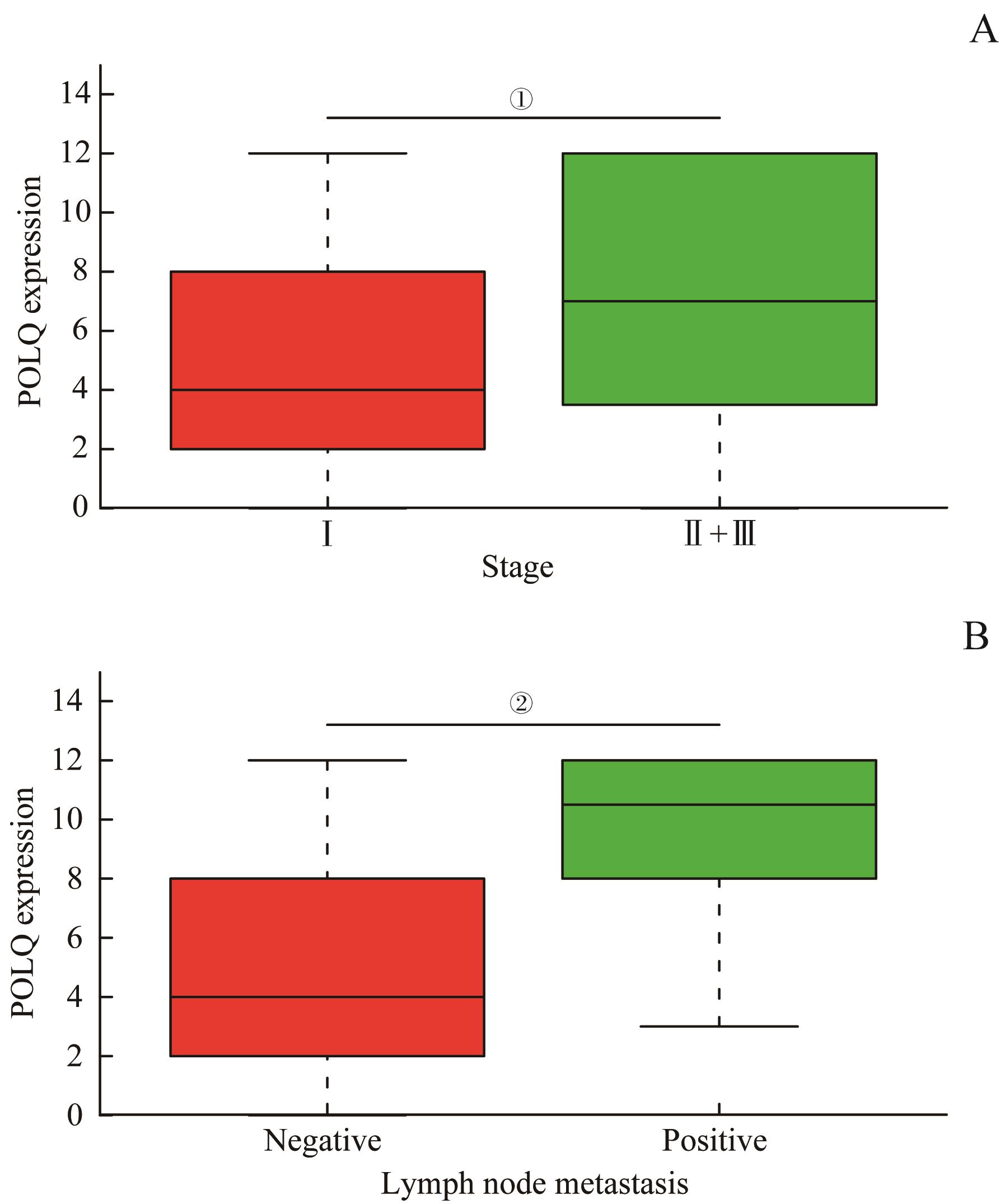
图6 POLQ表达水平在不同分期及淋巴结转移情况患者间的比较
Fig 6 Comparison of POLQ expression in the patients with different stages and lymph node metastasis conditionsNote:A. Expression of POLQ in different stages of EC tissues. B. Expression of POLQ in the patients with and without lymph node metastasis. ①P=0.008, ②P=0.023.
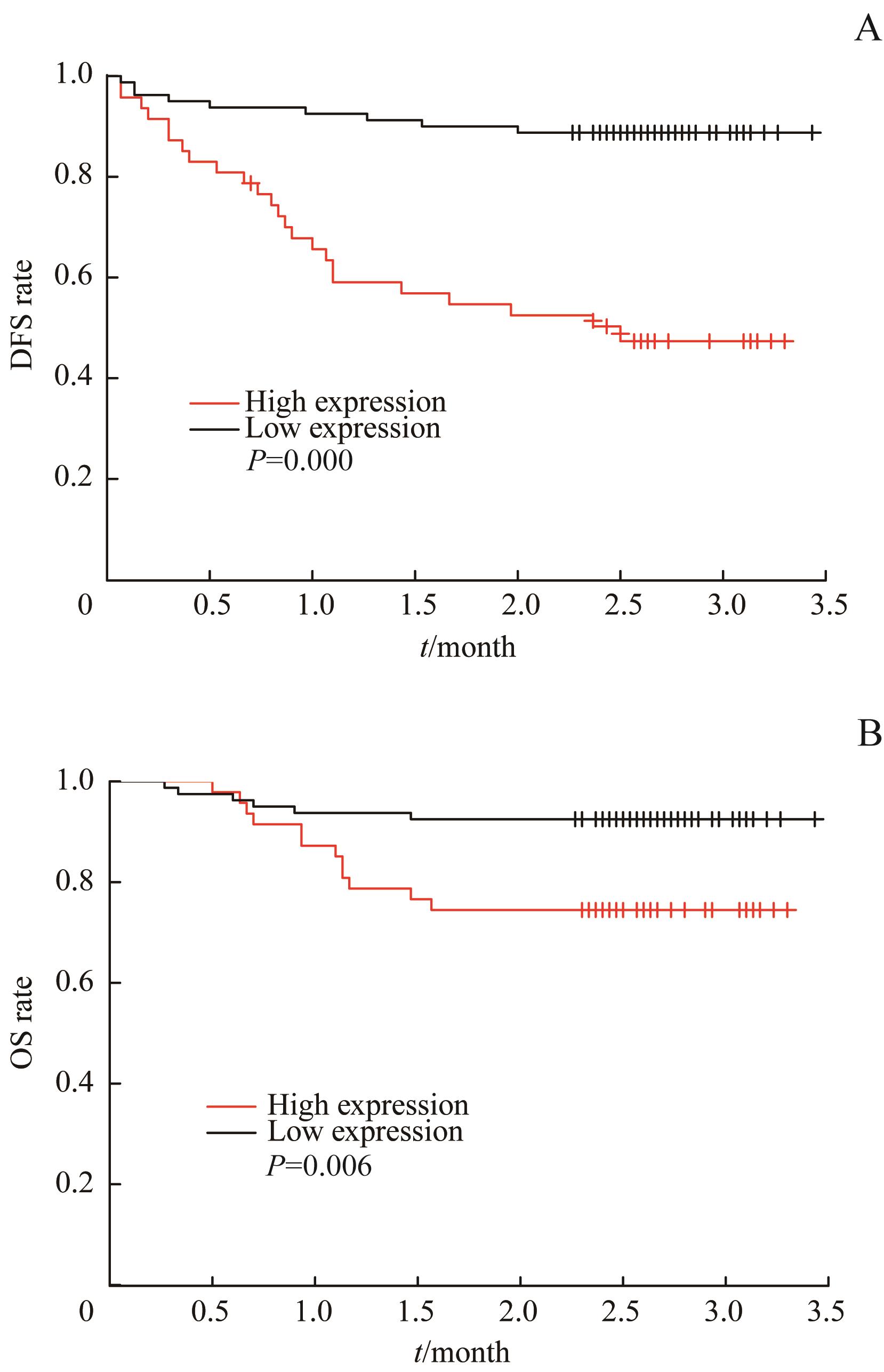
图7 不同POLQ表达水平EC患者的DFS(A)和OS(B)的Kaplan-Meier曲线
Fig 7 Kaplan-Meier curves of DFS (A) and OS (B) for the EC patients with different POLQ expression levels
| Age/year | ‒ | ‒ | ‒ | |
| <60 | ‒ | ‒ | ‒ | |
| ≥60 | ‒ | ‒ | ‒ | |
| Stage | ‒ | ‒ | ‒ | |
| Ⅰ‒Ⅱ | ‒ | ‒ | ‒ | |
| Ⅲ | ‒ | ‒ | ‒ | |
| Grade | ‒ | ‒ | ‒ | |
| 1‒2 | ‒ | ‒ | ‒ | |
| 3 | ‒ | ‒ | ‒ | |
| POLQ score/score | ‒ | ‒ | ||
| 0‒4 | ‒ | ‒ | ||
| 5‒12 | ‒ | ‒ | ||
表3 EC患者DFS和OS的多因素Cox分析
Tab 3 Multivariate Cox analysis of DFS and OS in the EC patients
| Age/year | ‒ | ‒ | ‒ | |
| <60 | ‒ | ‒ | ‒ | |
| ≥60 | ‒ | ‒ | ‒ | |
| Stage | ‒ | ‒ | ‒ | |
| Ⅰ‒Ⅱ | ‒ | ‒ | ‒ | |
| Ⅲ | ‒ | ‒ | ‒ | |
| Grade | ‒ | ‒ | ‒ | |
| 1‒2 | ‒ | ‒ | ‒ | |
| 3 | ‒ | ‒ | ‒ | |
| POLQ score/score | ‒ | ‒ | ||
| 0‒4 | ‒ | ‒ | ||
| 5‒12 | ‒ | ‒ | ||
| 1 | Lewin SN. Revised FIGO staging system for endometrial cancer[J]. Clin Obstet Gynecol, 2011, 54(2): 215-218. |
| 2 | Lortet-Tieulent J, Ferlay J, Bray F, et al. International patterns and trends in endometrial cancer incidence, 1978‒2013[J]. J Natl Cancer Inst, 2018, 110(4): 354-361. |
| 3 | 魏丽惠. 重视子宫内膜癌的筛查[J]. 中华妇产科杂志, 2013, 48(12): 881-883. |
| 4 | Salvesen HB, Haldorsen IS, Trovik J. Markers for individualised therapy in endometrial carcinoma[J]. Lancet Oncol, 2012, 13(8): e353-e361. |
| 5 | Morice P, Leary A, Creutzberg C, et al. Endometrial cancer[J]. Lancet, 2016, 387(10023): 1094-1108. |
| 6 | Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015[J]. CA Cancer J Clin, 2015, 65(1): 5-29. |
| 7 | Ashour ME, Mosammaparast N. Mechanisms of damage tolerance and repair during DNA replication[J]. Nucleic Acids Res, 2021, 49(6): 3033-3047. |
| 8 | Ranjha L, Howard SM, Cejka P. Main steps in DNA double-strand break repair: an introduction to homologous recombination and related processes[J]. Chromosoma, 2018, 127(2): 187-214. |
| 9 | Chang HHY, Pannunzio NR, Adachi N, et al. Non-homologous DNA end joining and alternative pathways to double-strand break repair[J]. Nat Rev Mol Cell Biol, 2017, 18(8): 495-506. |
| 10 | Koole W, van Schendel R, Karambelas AE, et al. A polymerase theta-dependent repair pathway suppresses extensive genomic instability at endogenous G4 DNA sites[J]. Nat Commun, 2014, 5: 3216. |
| 11 | Yousefzadeh MJ, Wyatt DW, Takata K, et al. Mechanism of suppression of chromosomal instability by DNA polymerase POLQ[J]. PLoS Genet, 2014, 10(10): e1004654. |
| 12 | Kamp JA, van Schendel R, Dilweg IW, et al. BRCA1-associated structural variations are a consequence of polymerase theta-mediated end-joining[J]. Nat Commun, 2020, 11(1): 3615. |
| 13 | Lemée F, Bergoglio V, Fernandez-Vidal A, et al. DNA polymerase theta up-regulation is associated with poor survival in breast cancer, perturbs DNA replication, and promotes genetic instability[J]. Proc Natl Acad Sci U S A, 2010, 107(30): 13390-13395. |
| 14 | 李学孝, 吴爱国, 胡斌, 等. DNA聚合酶θ对乳腺癌细胞株MCF-7放射敏感性的影响[J]. 中华实验外科杂志, 2012, 29(5): 801-804. |
| 15 | Shima N, Munroe RJ, Schimenti JC. The mouse genomic instability mutation chaos1 is an allele of Polq that exhibits genetic interaction with Atm[J]. Mol Cell Biol, 2004, 24(23): 10381-10389. |
| 16 | Seki M, Marini F, Wood RD. POLQ (Pol θ), a DNA polymerase and DNA-dependent ATPase in human cells[J]. Nucleic Acids Res, 2003, 31(21): 6117-6126. |
| 17 | Kawamura K, Bahar R, Seimiya M, et al. DNA polymerase θ is preferentially expressed in lymphoid tissues and upregulated in human cancers[J]. Int J Cancer, 2004, 109(1): 9-16. |
| 18 | Leoncini E, Ricciardi W, Cadoni G, et al. Adult height and head and neck cancer: a pooled analysis within the INHANCE Consortium[J]. Eur J Epidemiol, 2014, 29(1): 35-48. |
| 19 | Allera-Moreau C, Rouquette I, Lepage B, et al. DNA replication stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients[J]. Oncogenesis, 2012, 1(10): e30. |
| 20 | Pillaire MJ, Selves J, Gordien K, et al. A 'DNA replication' signature of progression and negative outcome in colorectal cancer[J]. Oncogene, 2010, 29(6): 876-887. |
| 21 | Higgins GS, Harris AL, Prevo R, et al. Overexpression of POLQ confers a poor prognosis in early breast cancer patients[J]. Oncotarget, 2010, 1(3): 175-184. |
| 22 | Wood RD, Doublié S. DNA polymerase θ (POLQ), double-strand break repair, and cancer[J]. DNA Repair (Amst), 2016, 44: 22-32. |
| 23 | van Schendel R, van Heteren J, Welten R, et al. Genomic scars generated by polymerase θ reveal the versatile mechanism of alternative end-joining[J]. PLoS Genet, 2016, 12(10): e1006368. |
| 24 | Ahrabi S, Sarkar S, Pfister SX, et al. A role for human homologous recombination factors in suppressing microhomology-mediated end joining[J]. Nucleic Acids Res, 2016, 44(12): 5743-5757. |
| 25 | Goullet de Rugy T, Bashkurov M, Datti A, et al. Excess Polθ functions in response to replicative stress in homologous recombination-proficient cancer cells[J]. Biol Open, 2016, 5(10): 1485-1492. |
| 26 | Ceccaldi R, Liu JC, Amunugama R, et al. Homologous-recombination-deficient tumours are dependent on Polθ-mediated repair[J]. Nature, 2015, 518(7538): 258-262. |
| 27 | Nik-Zainal S, Davies H, Staaf J, et al. Landscape of somatic mutations in 560 breast cancer whole-genome sequences[J]. Nature, 2016, 534(7605): 47-54. |
| 28 | Alexandrov LB, Nik-Zainal S, Wedge DC, et al. Signatures of mutational processes in human cancer[J]. Nature, 2013, 500(7463): 415-421. |
| 29 | Carvajal-Garcia J, Cho JE, Carvajal-Garcia P, et al. Mechanistic basis for microhomology identification and genome scarring by polymerase θ[J]. Proc Natl Acad Sci U S A, 2020, 117(15): 8476-8485. |
| [1] | 彭倩倩, 宋璟涵, 徐杏怡, 肖辉. RNA结合蛋白HuR通过调控ITGB1促进非小细胞肺癌进展的生物信息学分析及验证[J]. 上海交通大学学报(医学版), 2026, 46(4): 451-466. |
| [2] | 王一然, 张哲, 沈键锋. 综合分析SF3B1突变在葡萄膜黑色素瘤中的功能、预后及免疫浸润特征[J]. 上海交通大学学报(医学版), 2026, 46(4): 475-485. |
| [3] | 梅子贤, 孟旭晨, 苏文静, 钟伟杰, 汤定中, 李轶. 临床-炎症联合模型预测前循环急性大血管闭塞性缺血性卒中男性患者机械取栓术后的不良预后[J]. 上海交通大学学报(医学版), 2026, 46(3): 332-339. |
| [4] | 何嘉音, 陈思远, 施晴, 张慕晨, 易红梅, 董磊, 钱樱, 王黎, 程澍, 许彭鹏, 赵维莅. 肾上腺累及的弥漫性大B细胞淋巴瘤患者临床病理特征、基因突变谱及预后分析[J]. 上海交通大学学报(医学版), 2025, 45(9): 1194-1201. |
| [5] | 陈思远, 施晴, 付迪, 王黎, 程澍, 许彭鹏, 赵维莅. 肺受累弥漫大B细胞淋巴瘤临床病理特征、基因突变谱及预后分析[J]. 上海交通大学学报(医学版), 2025, 45(9): 1214-1220. |
| [6] | 严治, 吴星玥, 姚卫芹, 颜灵芝, 金松, 商京晶, 施晓兰, 吴德沛, 傅琤琤. 免疫不全麻痹在新诊断多发性骨髓瘤患者中的动态变化及预后意义[J]. 上海交通大学学报(医学版), 2025, 45(7): 807-814. |
| [7] | 李卓杭, 于新迪, 任婧雅, 沈佳, 董素贞, 王伟. 主动脉缩窄端侧吻合纠治术后的神经系统预后分析[J]. 上海交通大学学报(医学版), 2025, 45(6): 753-759. |
| [8] | 汤开然, 冯成领, 韩邦旻. 基于单细胞测序与转录组测序构建M2巨噬细胞基因相关的前列腺癌预后模型[J]. 上海交通大学学报(医学版), 2025, 45(5): 549-561. |
| [9] | 许天芸, 沈奕茗, 姜萌. 射血分数改善型心力衰竭的临床管理: 治疗与维持[J]. 上海交通大学学报(医学版), 2025, 45(4): 493-499. |
| [10] | 刘田恬, 赵奕琳, 宁菁菁, 张育才, 王春霞. 儿童脓毒症预后相关长链非编码RNA筛选及竞争性内源RNA网络的构建[J]. 上海交通大学学报(医学版), 2025, 45(3): 282-291. |
| [11] | 王博恩, 陈思远, 施晴, 张慕晨, 易红梅, 董磊, 王黎, 程澍, 许彭鹏, 赵维莅. 肾脏累及的弥漫性大B细胞淋巴瘤患者临床病理特征[J]. 上海交通大学学报(医学版), 2024, 44(9): 1162-1168. |
| [12] | 魏云鑫, 蒋绪顺, 蔡梦瑶, 温睿智, 杜晓刚. COMP与糖尿病肾病自噬相关性分析及其功能验证[J]. 上海交通大学学报(医学版), 2024, 44(7): 847-858. |
| [13] | 宋晨璐, 向军, 杨惠忠. 血清肝素结合蛋白对重度烧伤患者预后及脓毒症发生的早期预警价值[J]. 上海交通大学学报(医学版), 2024, 44(4): 474-481. |
| [14] | 王鑫, 王晓霞, 李彦庆, 郑永鑫, 乌杰, 任猛, 贾向东, 许天祥. 香叶基香叶基焦磷酸合成酶在肺鳞状细胞癌中的表达及临床意义[J]. 上海交通大学学报(医学版), 2024, 44(3): 312-324. |
| [15] | 王桂杰, 杜传冲, 陆叶, 赵健, 沈勰, 金冬林, 耿佳财. 多发伤患者血清高迁移率族蛋白B1及可溶性髓样细胞触发受体-1水平变化及预后意义[J]. 上海交通大学学报(医学版), 2024, 44(3): 350-357. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||