上海交通大学学报(医学版) ›› 2023, Vol. 43 ›› Issue (7): 906-915.doi: 10.3969/j.issn.1674-8115.2023.07.013
陈惠( ), 朱唯一, 姚屹瑾()
), 朱唯一, 姚屹瑾()
收稿日期:2023-01-07
接受日期:2023-07-10
出版日期:2023-07-28
发布日期:2023-07-28
通讯作者:
姚屹瑾,电子信箱:776470193@qq.com。作者简介:陈 惠(1992—),女,护师,硕士;电子信箱:1332209878@qq.com。
CHEN Hui(), ZHU Weiyi, YAO Yijin()
Received:2023-01-07
Accepted:2023-07-10
Online:2023-07-28
Published:2023-07-28
Contact:
YAO Yijin, E-mail: 776470193@qq.com.摘要:
目的·采用meta分析评价根据促甲状腺激素(thyroid stimulating hormone,TSH)水平调整左旋甲状腺素(levothyroxine,L-T4)治疗剂量对甲状腺功能减退孕妇母婴结局的影响。方法·检索中国知网、维普中文科技期刊数据库、万方数据知识服务平台、PubMed、Cochrane Library、Embase数据库,收集建库至2022年4月9日所有关于根据TSH水平调整L-T4剂量治疗甲状腺功能减退孕妇的对照研究文献,并追溯参考文献。2名研究人员独立对所获取的文献进行筛选、数据提取及质量评价,其中质量评价采用Cochrane评价表。结局评价指标包括妊娠高血压、妊娠糖尿病、产后出血、分娩方式、早产、胎儿死亡、新生儿窒息、低出生体质量儿,采用RevMan 5.3软件进行meta分析。结果·在6个数据库共检索到1 268篇文献,最终纳入8篇,其中中文文献4篇、英文文献4篇,整体研究偏倚风险处于中等水平。相对于对照组,根据甲状腺功能减退孕妇TSH水平调整L-T4剂量的试验组孕妇发生妊娠糖尿病风险OR值为0.61(95%CI 0.44~0.86,P=0.004),发生胎儿死亡风险OR值为0.38(95%CI 0.18~0.81,P=0.010),均具有统计学意义。而调整L-T4剂量的治疗方式在阴道分娩[OR=1.82(95%CI 0.75~4.40,P=0.180)]、妊娠高血压[OR=0.77(95%CI 0.53~1.12,P=0.170)]、产后出血[OR=1.20(95%CI 0.50~2.92,P=0.680)]、早产[OR=0.72(95%CI 0.48~1.06,P=0.100)]、低出生体质量儿[OR=1.00(95%CI 0.65~1.54,P=0.999)]和新生儿窒息[OR=0.50(95%CI 0.20~1.27,P=0.150)]发生风险方面与对照组差异无统计学意义。结论·根据TSH水平调整L-T4治疗剂量,可能有助于降低甲状腺功能减退孕妇的妊娠糖尿病和胎儿死亡风险。
中图分类号:
陈惠, 朱唯一, 姚屹瑾. 调整左旋甲状腺素治疗剂量对甲状腺功能减退孕妇母婴结局影响的meta分析[J]. 上海交通大学学报(医学版), 2023, 43(7): 906-915.
CHEN Hui, ZHU Weiyi, YAO Yijin. A meta-analysis of the effects of levothyroxine dose adjustment on maternal and infant outcomes in pregnant women with hypothyroidism[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(7): 906-915.

图1 文献筛选流程图
Fig 1 Flow diagram of the selection process of the included articles
| First author | Year of publica-tion | Nation | Number of cases/n | Age/year | Intervention | Primary outcome index | |||
|---|---|---|---|---|---|---|---|---|---|
| Exp | Con | Exp | Con | Exp | Con | ||||
| GAO[ | 2021 | China | 46 | 34 | 25.3±3.4 | 24.8±3.1 | Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted | Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet | GH, PH, GDM, PD |
| YE[ | 2016 | China | 28 | 28 | 22-34 | 22-34 | The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given | GDM, GH, DM, LBW, FD, NA |
| MA[ | 2020 | China | 42 | 42 | 28.74±4.08 | 28.25±4.15 | The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked once a month and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of L-T4 was 50 μg/d | GH, GDM, FD, PD, NA, LBW, DM, abortion |
| LIU[ | 2021 | China | 49 | 49 | 26.9±4.6 | 26.8±4.7 | The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked termly and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of L-T4 was 25 μg/d | DM, FD, abortion, PD, NA, LBW |
| CASEY[ | 2017 | America | 339 | 338 | 27.7±5.7 | 27.3±5.7 | The initial dose of L-T4 was 100 μg/d. TSH level was checked once a month and the L-T4 dose was adjusted. TSH level was controlled in the range of 0.1‒2.5 mIU/L | A placebo of 100 μg was given daily with a dummy adjustment | GDM, GH, LBW, PD, FD |
| BLUMENTHAL[ | 2017 | Australia | 92 | 933 | 33.47±1.41 | 35.00±5.20 | The iodized salt was increased in the diet. The dose of L-T4 was 50 μg/d when TSH>2.5 mIU/L. TSH was checked every 4 weeks and the L-T4 dose was adjusted | The iodine was increased in diet and L-T4 was not given | DM, GH, GDM, PD, FD |
| WANG[ | 2012 | China | 28 | 168 | Not mentioned | 28.14±0.27 | The initial dose of L-T4 depended on the pregnant woman′s TSH level. TSH 2.5‒5 mIU/L: L-T4 50 μg/d; TSH >5‒8 mIU/L: L-T4 75 μg/d; TSH>8 mIU/L: L-T4 100 μg/d. TSH level was checked every 4 weeks and the L-T4 dose was adjusted | L-T4 was not given | GH, PD, LBW, PH, abortion, NA |
| JU[ | 2016 | China | 184 | 273 | 29.31±3.36 | 28.88±3.53 | The initial LT-4 dose was determined based on TSH level. Dose of LT-4 was adjusted according to the treatment objective of TSH | L-T4 was not given | GDM, GH, PH, PD, LBW |
表1 纳入研究基本特征
Tab 1 Basic characteristics of the studies
| First author | Year of publica-tion | Nation | Number of cases/n | Age/year | Intervention | Primary outcome index | |||
|---|---|---|---|---|---|---|---|---|---|
| Exp | Con | Exp | Con | Exp | Con | ||||
| GAO[ | 2021 | China | 46 | 34 | 25.3±3.4 | 24.8±3.1 | Guidance on routine maternal care was given. The initial dose of L-T4 was 50 μg/d. TSH level was re-examined 2 weeks later and the dose was adjusted | Guidance on routine maternal care was given. The iodized salt was increased and the fat was reduced in the diet | GH, PH, GDM, PD |
| YE[ | 2016 | China | 28 | 28 | 22-34 | 22-34 | The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given. TSH was checked every 4‒6 weeks and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. Routine medication and nursing interventions were given | GDM, GH, DM, LBW, FD, NA |
| MA[ | 2020 | China | 42 | 42 | 28.74±4.08 | 28.25±4.15 | The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked once a month and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of L-T4 was 50 μg/d | GH, GDM, FD, PD, NA, LBW, DM, abortion |
| LIU[ | 2021 | China | 49 | 49 | 26.9±4.6 | 26.8±4.7 | The fat was reduced, and the iodized salt and the protein were increased in the diet. TSH level was checked termly and the L-T4 dose was adjusted | The fat was reduced, and the iodized salt and the protein were increased in the diet. The dose of L-T4 was 25 μg/d | DM, FD, abortion, PD, NA, LBW |
| CASEY[ | 2017 | America | 339 | 338 | 27.7±5.7 | 27.3±5.7 | The initial dose of L-T4 was 100 μg/d. TSH level was checked once a month and the L-T4 dose was adjusted. TSH level was controlled in the range of 0.1‒2.5 mIU/L | A placebo of 100 μg was given daily with a dummy adjustment | GDM, GH, LBW, PD, FD |
| BLUMENTHAL[ | 2017 | Australia | 92 | 933 | 33.47±1.41 | 35.00±5.20 | The iodized salt was increased in the diet. The dose of L-T4 was 50 μg/d when TSH>2.5 mIU/L. TSH was checked every 4 weeks and the L-T4 dose was adjusted | The iodine was increased in diet and L-T4 was not given | DM, GH, GDM, PD, FD |
| WANG[ | 2012 | China | 28 | 168 | Not mentioned | 28.14±0.27 | The initial dose of L-T4 depended on the pregnant woman′s TSH level. TSH 2.5‒5 mIU/L: L-T4 50 μg/d; TSH >5‒8 mIU/L: L-T4 75 μg/d; TSH>8 mIU/L: L-T4 100 μg/d. TSH level was checked every 4 weeks and the L-T4 dose was adjusted | L-T4 was not given | GH, PD, LBW, PH, abortion, NA |
| JU[ | 2016 | China | 184 | 273 | 29.31±3.36 | 28.88±3.53 | The initial LT-4 dose was determined based on TSH level. Dose of LT-4 was adjusted according to the treatment objective of TSH | L-T4 was not given | GDM, GH, PH, PD, LBW |
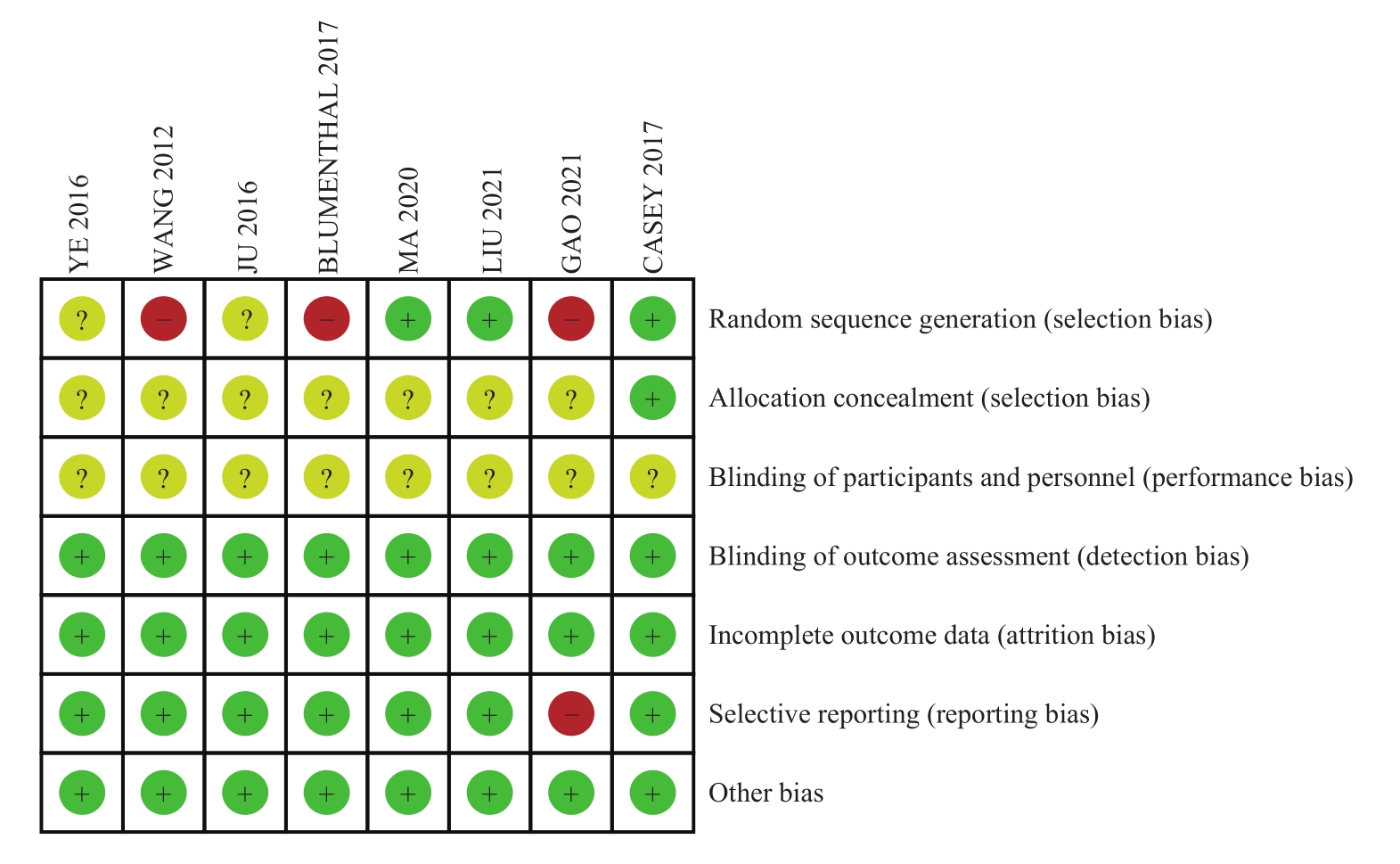
图2 纳入文献的风险偏倚评估
Fig 2 Risk bias assessment of the included articles
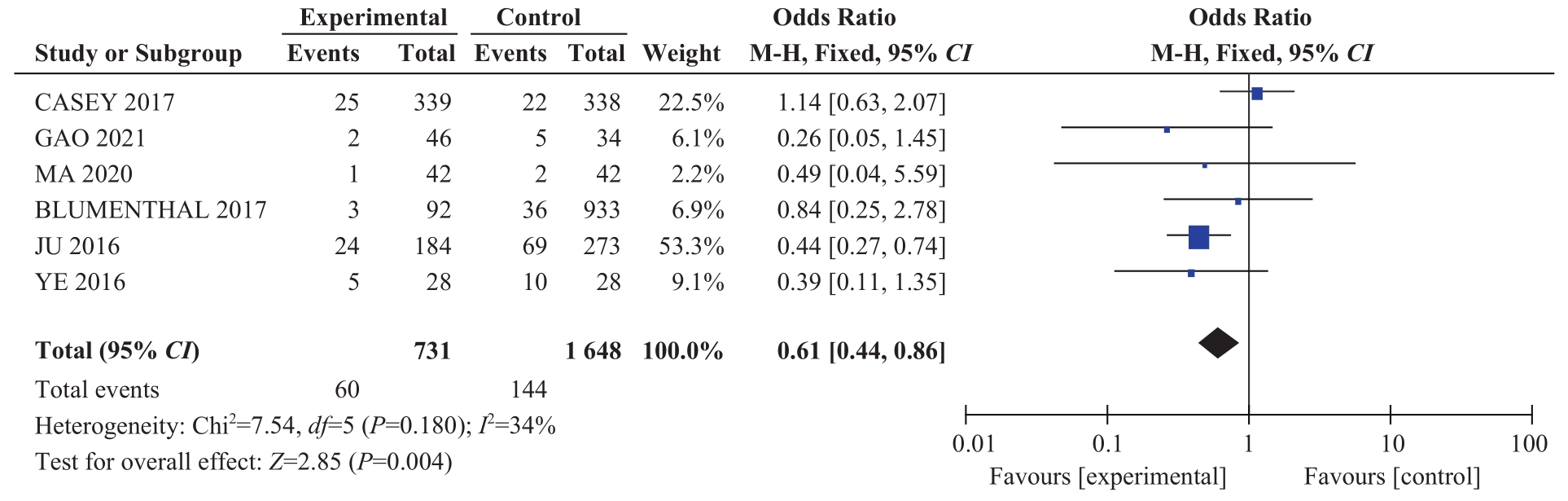
图3 2组甲减孕妇发生妊娠糖尿病风险的比较
Fig 3 Comparison of the risk of gestational diabetes in the pregnant women with hypothyroidism between the two groups

图4 2组甲减孕妇发生妊娠高血压风险的比较
Fig 4 Comparison of the risk of gestational hypertension in the pregnant women with hypothyroidism between the two groups

图5 2组甲减孕妇发生产后出血风险的比较
Fig 5 Comparison of the risk of postpartum hemorrhage in the pregnant women with hypothyroidism between the two groups

图6 2组甲减孕妇经阴道分娩的比较
Fig 6 Comparison of vaginal delivery in the pregnant women with hypothyroidism between the two groups

图7 2组甲减孕妇的胎儿死亡风险的比较
Fig 7 Comparison of the risk of fetal death in the pregnant women with hypothyroidism between the two groups

图8 2组甲减孕妇的新生儿窒息风险的比较
Fig 8 Comparison of the risk of neonatal asphyxia in the pregnant women with hypothyroidism between the two groups
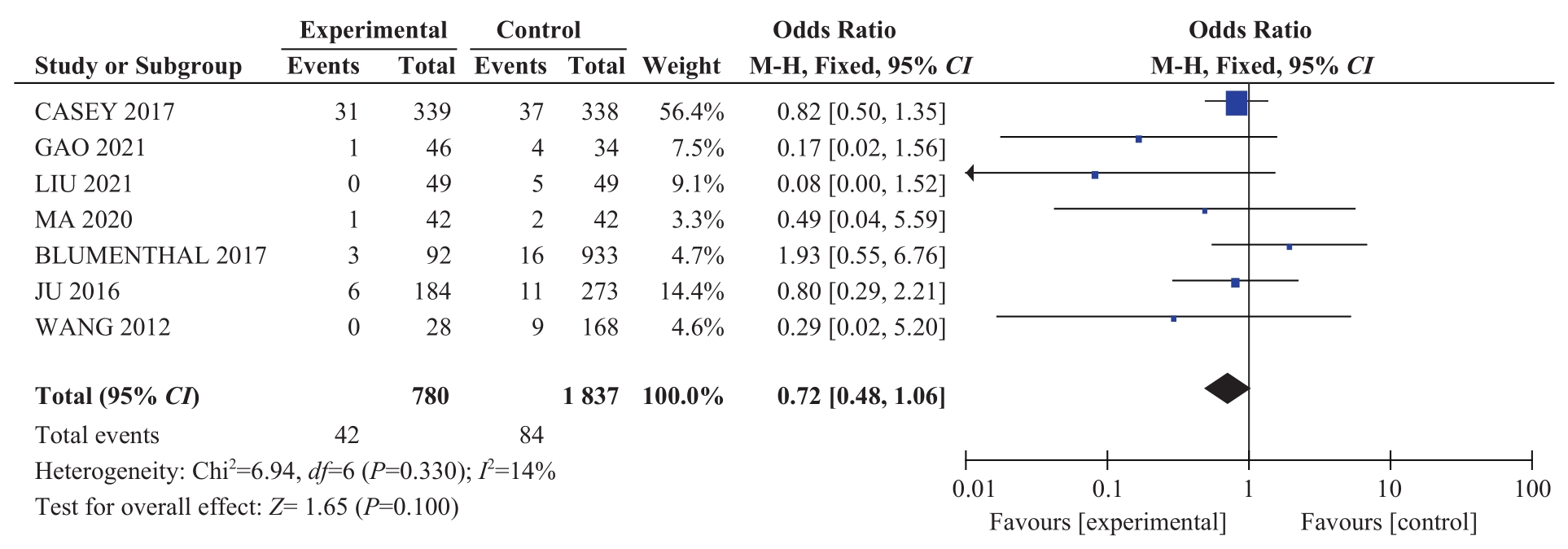
图9 2组甲减孕妇的早产风险的比较
Fig 9 Comparison of the risk of preterm birth in the pregnant women with hypothyroidism between the two groups

图10 2组甲减孕妇的低出生体质量儿风险的比较
Fig 10 Comparison of the risk of low birth weight infants in the pregnant women with hypothyroidism between the two groups
| 1 | DONG A C, STAGNARO-GREEN A. Differences in diagnostic criteria mask the true prevalence of thyroid disease in pregnancy: a systematic review and meta-analysis[J]. Thyroid, 2019, 29(2): 278-289. |
| 2 | ABALOVICH M, GUTIERREZ S, ALCARAZ G, et al. Overt and subclinical hypothyroidism complicating pregnancy[J]. Thyroid, 2002, 12(1): 63-68. |
| 3 | SULLIVAN S A. Hypothyroidism in pregnancy[J]. Clin Obstet Gynecol, 2019, 62(2): 308-319. |
| 4 | The Consortium on Thyroid and Pregnancy-Study Group on Preterm Birth. Association of thyroid function test abnormalities and thyroid autoimmunity with preterm birth: a systematic review and meta-analysis[J]. JAMA, 2019, 322(7): 632-641. |
| 5 | MARAKA S, OSPINA N M S, O′KEEFFE D T, et al. Subclinical hypothyroidism in pregnancy: a systematic review and meta-analysis[J]. Thyroid, 2016, 26(4): 580-590. |
| 6 | SULLIVAN S D, DOWNS E, POPOVENIUC G, et al. Randomized trial comparing two algorithms for levothyroxine dose adjustment in pregnant women with primary hypothyroidism[J]. J Clin Endocrinol Metab, 2017, 102(9): 3499-3507. |
| 7 | TOLOZA F J K, ABEDZADEH-ANARAKI S, MARAKA S. Subclinical hypothyroidism in pregnancy[J]. Curr Opin Endocrinol Diabetes Obes, 2019, 26(5): 225-231. |
| 8 | 高金保. 观察妊娠期亚临床甲减以及甲状腺激素干预治疗对妊娠结局的影响[J]. 云南医药, 2021, 42(4): 345-347. |
| GAO J B. Observation of the effect of subclinical hypothyroidism during pregnancy and thyroid hormone intervention on pregnancy outcome[J]. Medicine and Pharmacy of Yunnan, 2021, 42(4):345-347. | |
| 9 | 叶晓梅, 陈友英. 左旋甲状腺素片治疗妊娠合并甲状腺功能减退28例剂量调整[J]. 中国妇幼健康研究, 2016, 27(S1): 425. |
| YE X M,CHEN Y Y. Dose adjustment of levothyroxine tablets for 28 cases of pregnancy complicated with hypothyroidism[J]. Chinese Journal of Woman and Child Health Research, 2016, 27(S1): 425. | |
| 10 | 马玉红. 左旋甲状腺素钠片的不同剂量对妊娠期甲减患者的治疗效果分析[J]. 医学理论与实践, 2020, 33(18): 3060-3062. |
| MA Y H. Analysis of therapeutic effect of different doses of levothyroxine sodium tablets on pregnant women with hypothyroidism [J]. The Journal of Medical Theory and Practice, 2020, 33(18): 3060-3062. | |
| 11 | 柳丽君. 左旋甲状腺素片治疗妊娠合并甲减患者剂量调整分析[J]. 海峡药学, 2021, 33(7): 181-182 |
| LIU L J. Dose adjustment analysis of levothyroxine tablets for pregnant women with hypothyroidism[J]. Strait Pharmaceutical Journal, 2021, 33(7): 181-182. | |
| 12 | CASEY B M, THOM E A, PEACEMAN A M, et al. Treatment of subclinical hypothyroidism or hypothyroxinemia in pregnancy[J]. N Engl J Med, 2017, 376(9): 815-825. |
| 13 | BLUMENTHAL N J, EASTMAN C J. Beneficial effects on pregnancy outcomes of thyroid hormone replacement for subclinical hypothyroidism[J]. J Thyroid Res, 2017, 2017: 4601365. |
| 14 | WANG S, TENG W P, LI J X, et al. Effects of maternal subclinical hypothyroidism on obstetrical outcomes during early pregnancy[J]. J Endocrinol Invest, 2012, 35(3): 322-325. |
| 15 | JU R, LIN L, LONG Y, et al. Clinical efficacy of therapeutic intervention for subclinical hypothyroidism during pregnancy[J]. Genet Mol Res, 2016, 15(4). DOI: 10.4238/gmr15049019. |
| 16 | 李春莉, 黄卉, 李秋红. 妊娠早期亚临床甲状腺功能减退与妊娠糖尿病的相关性研究[J]. 中华内分泌代谢杂志, 2014, 30(9): 747-748. |
| LI C L, HUANG H, LI Q H. Relationship of subclinical hypothyroidism with gestational diabetes mellitus during early pregnancy[J]. Chinese Journal of Endocrinology and Metabolism, 2014, 30(9): 747-748. | |
| 17 | DERAKHSHAN A, KOREVAAR T I M, TAYLOR P N, et al. The association of maternal thyroid autoimmunity during pregnancy with child IQ[J]. J Clin Endocrinol Metab, 2018, 103(10): 3729-3736. |
| 18 | 刘娟弟, 王瑞, 何菊仙. 甲状腺功能减退与孕早期自发性流产的相关性分析[J]. 医学临床研究, 2022, 39(2): 232-235 |
| LIU J D, WANG R, HE J X. Relationship between hypothyroidism and spontaneous abortion in early pregnancy[J]. Journal of Clinical Research, 2022, 39(2): 232-235. | |
| 19 | ALEXANDER E K, PEARCE E N, BRENT G A, et al. 2017 guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum[J]. Thyroid, 2017, 27(3): 315-389. |
| 20 | DING Z, LIU Y D, MARAKA S, et al. Pregnancy and neonatal outcomes with levothyroxine treatment in women with subclinical hypothyroidism based on new diagnostic criteria: a systematic review and meta-analysis[J]. Front Endocrinol (Lausanne), 2021, 12: 797423. |
| 21 | JIAO X F, ZHANG M, CHEN J J, et al. The impact of levothyroxine therapy on the pregnancy, neonatal and childhood outcomes of subclinical hypothyroidism during pregnancy: an updated systematic review, meta-analysis and trial sequential analysis[J]. Front Endocrinol (Lausanne), 2022, 13: 964084. |
| 22 | MAGRI F, CHIOVATO L, CROCE L, et al. Thyroid hormone therapy for subclinical hypothyroidism[J]. Endocrine, 2019, 66(1): 27-34. |
| 23 | PEARCE E N. Management of hypothyroidism and hypothyroxinemia during pregnancy[J]. Endocr Pract, 2022, 28(7): 711-718. |
| 24 | 单忠艳, 滕卫平. 《妊娠和产后甲状腺疾病诊治指南》(第2版)要点解读[J]. 中华内分泌代谢杂志, 2019, 35(8): 632-635. |
| SHAN Z Y, TENG W P. Guideline on diagnosis and management of thyroid diseases during pregnancy and postpartum (2nd edition): an essential introduction[J]. Chinese Journal of Endocrinology and Metabolism, 2019, 35(8): 632-635. | |
| 25 | 《孕产期甲状腺疾病防治管理指南》编撰委员会, 中华医学会内分泌学分会, 中华预防医学会妇女保健分会. 孕产期甲状腺疾病防治管理指南[J]. 中华内分泌代谢杂志, 2022, 38(7): 539-551. |
| Writing Committee for Guidelines for Prevention and Management of Thyroid Diseases During Pregnancy and Perinatal Period, Chinese Society of Endocrinology, Chinese Medical Association, Women′s Health Care Branch of Chinese Preventive Medicine Association. Guidelines for prevention and management of thyroid diseases during pregnancy and perinatal period[J]. Chinese Journal of Endocrinology and Metabolism, 2022, 38(7): 539-551. | |
| 26 | HUBALEWSKA-DYDEJCZYK A, TROFIMIUK-MÜLDNER M, RUCHALA M, et al. Thyroid diseases in pregnancy: guidelines of the Polish Society of Endocrinology[J]. Endokrynol Pol, 2021, 72(5): 425-488. |
| 27 | 王文娟. 左甲状腺素钠片对妊娠期甲减患者甲状腺功能、不良反应及妊娠结局的改善效果[J]. 实用妇科内分泌电子杂志, 2022, 9(12): 27-30. |
| WANG W J. Effects of levothyroxine sodium tablets on thyroid function, adverse reactions and pregnancy outcomes in patients with hypothyroidism during pregnancy[J]. Electronic Journal of Practical Gynecological Endocrinology, 2022, 9(12): 27-30. | |
| 28 | HAN Y, WANG J, WANG X Y, et al. Relationship between subclinical hypothyroidism in pregnancy and hypertensive disorder of pregnancy: a systematic review and meta-analysis[J]. Front Endocrinol (Lausanne), 2022, 13: 823710. |
| 29 | 宋茜茜, 李志红, 郭淑芹, 等. 妊娠糖尿病伴亚临床甲减对孕妇骨密度及骨钙素、25-羟基维生素D的影响[J]. 中国计划生育学杂志, 2020, 28(1): 56-59 |
| SONG Q Q, LI Z H, GUO S Q, et al. Effect of disease of pregnant women with gestational diabetes mellitus and subclinical hypothyroidism on their bone mineral density, and levels of osteocalcin and 25-hydroxyvitamin D[J]. Chinese Journal of Family Planning, 2020, 28(1): 56-59. | |
| 30 | VELASCO I, VILA L, GOYA M, et al. Executive summary of the SEEN (Sociedad Española de Endocrinología y Nutrición [Spanish Society of Endocrinology and Nutrition])-SEGO (Sociedad Española deGinecología y Obstetricia [Spanish Society of Gynaecology and Obstetrics]) consensus document on the management of thyroid dysfunction during pregnancy[J]. Endocrinol Diabetes Nutr (Engl Ed), 2023, 70(Suppl 1): 38-50. |
| [1] | 赵建磊, 赵婧琦, 刘唱, 黄靖竣, 金升元. 水动力清创治疗烧伤的效果:随机对照试验的系统评价[J]. 上海交通大学学报(医学版), 2025, 45(5): 614-623. |
| [2] | 孙晨寅, 吴百川, 张慧凤, 方贻儒, 彭代辉. 体动记录仪评估抑郁症昼夜节律:一项系统综述和meta分析[J]. 上海交通大学学报(医学版), 2024, 44(5): 606-616. |
| [3] | 杨越, 何开举, 宗家豪, 杨自逸, 吴向嵩, 龚伟. 细胞游离DNA在胆道癌诊断中的价值:一项meta分析[J]. 上海交通大学学报(医学版), 2023, 43(9): 1175-1185. |
| [4] | 马卓然, 袁安彩, 蒋惠如, 陈潇雨, 张薇, 卜军. 脂质蓄积指数与中国成年人高血压关系的meta分析[J]. 上海交通大学学报(医学版), 2023, 43(4): 466-473. |
| [5] | 张越, 瞿蕾, 谷沁, 朱亦清, 马莉莹, 孙文广. 妊娠期糖尿病孕妇尿酮体持续阳性对母婴临床结局的影响[J]. 上海交通大学学报(医学版), 2023, 43(3): 314-319. |
| [6] | 梁妍景, 黄楚贤, 李红艳, 侯黎莉. 维生素E对放疗或化疗导致的口腔黏膜炎有效性的meta分析[J]. 上海交通大学学报(医学版), 2023, 43(2): 208-214. |
| [7] | 杨玲, 侯黎莉, 赵燕, 陈卫宏, 张金凤, 毛艳. 口腔癌患者张口受限患病率的meta分析[J]. 上海交通大学学报(医学版), 2023, 43(1): 61-69. |
| [8] | 方芳, 台瑞, 余倩, 章雅青. 预康复对胃肠道择期手术患者术后恢复效果的系统评价[J]. 上海交通大学学报(医学版), 2023, 43(1): 70-78. |
| [9] | 陈卫宏, 侯黎莉, 杨玲, 毛艳, 张金凤. 冷冻疗法预防头颈癌患者放射性口腔黏膜炎的meta分析[J]. 上海交通大学学报(医学版), 2022, 42(5): 635-645. |
| [10] | 谭颖超, 杨珺玥, 王莉娜. 白细胞介素-1B-511C/T基因多态性与冠状动脉粥样硬化性心脏病关联的meta分析[J]. 上海交通大学学报(医学版), 2022, 42(2): 197-204. |
| [11] | 钱德伟, 周任, 关礼春, 张航, 虞敏. 吸入一氧化氮气体对外科手术后肾功能损伤和出血影响的meta分析[J]. 上海交通大学学报(医学版), 2022, 42(1): 95-100. |
| [12] | 王毅, 程诚, 沈红艳, 高红艳, 戴悦宁, 易正辉. 经颅磁刺激对阿尔茨海默病患者认知功能及伴痴呆的行为精神症状疗效的meta分析[J]. 上海交通大学学报(医学版), 2021, 41(7): 931-941. |
| [13] | 刘洁, 谢新民, 支雪梅, 陆静毅. 睡眠时间与糖尿病性视网膜病变风险关系的meta分析[J]. 上海交通大学学报(医学版), 2021, 41(11): 1502-1508. |
| [14] | 陈智灵, 罗晨, 赵康佳, 沈玲, 胡三莲. 2种镇痛方式在结直肠癌术后应用效果的meta分析[J]. 上海交通大学学报(医学版), 2021, 41(10): 1344-1350. |
| [15] | 潘胜珂,李 惠,魏燕燕,姚培芬,李华芳. 安慰剂治疗原发性失眠症患者的meta分析[J]. 上海交通大学学报(医学版), 2020, 40(4): 505-. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||