Journal of Shanghai Jiao Tong University (Medical Science) ›› 2022, Vol. 42 ›› Issue (3): 357-363.doi: 10.3969/j.issn.1674-8115.2022.03.014
• Evidence-based medicine • Previous Articles Next Articles
LI Yan1( ), JIANG Yan2, KANG Qiongfang3, LU Qunfeng2()
), JIANG Yan2, KANG Qiongfang3, LU Qunfeng2()
Received:2021-10-15
Online:2022-03-28
Published:2022-05-09
Contact:
LU Qunfeng
E-mail:ncdwwll@126.com;luluroom2004@163.com
CLC Number:
LI Yan, JIANG Yan, KANG Qiongfang, LU Qunfeng. Summary of the best evidence summary on prevention strategies for diaper dermatitis in infants[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(3): 357-363.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2022.03.014
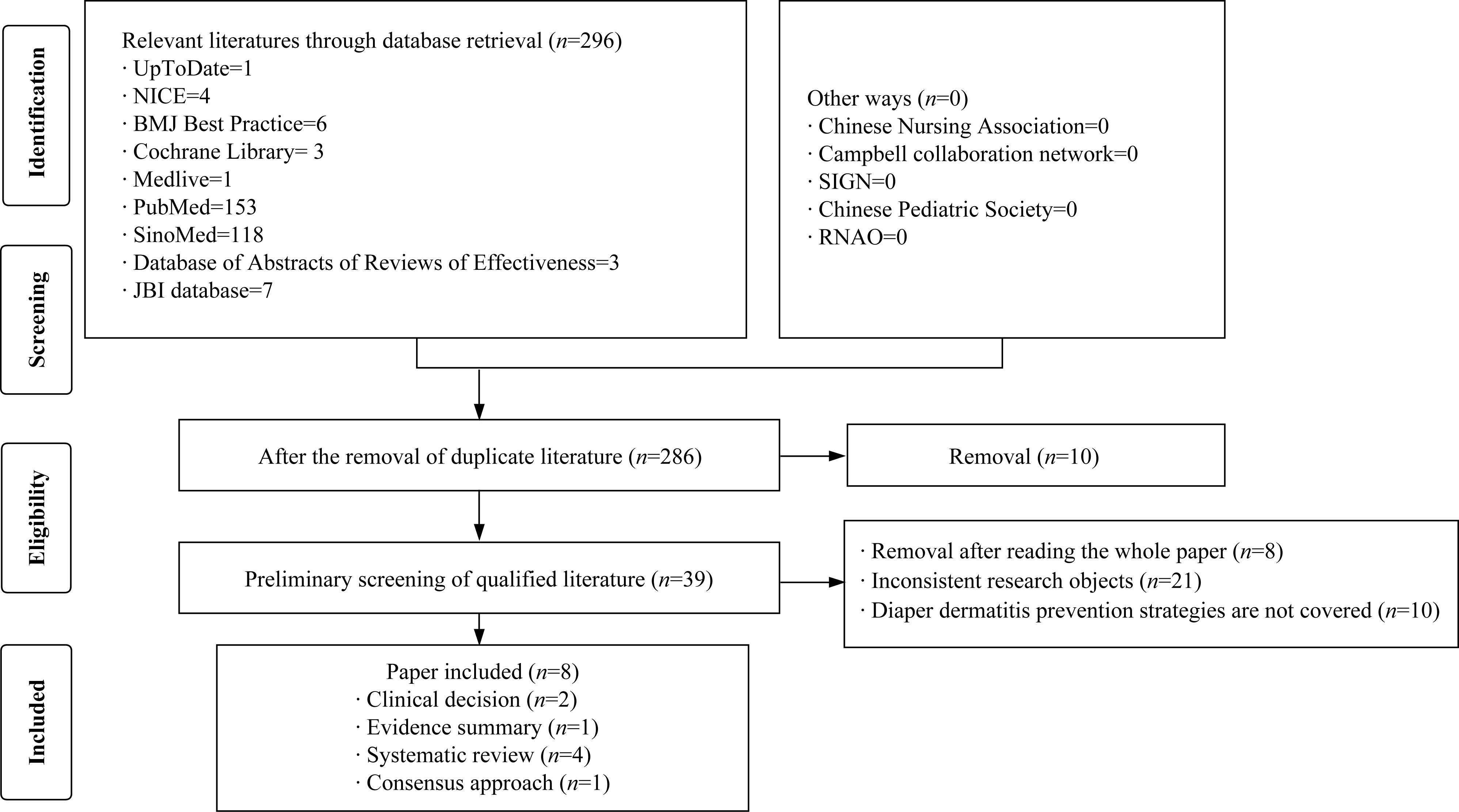
Fig 1 Literature screening process and results
| Study | Year | Resource | Type | Theme |
|---|---|---|---|---|
| MATHEW[ | 2021 | JBI | Evidence summary | Management of diaper dermatitis in infants and preschool children |
| BAER[ | 2006 | Cochrane | Systematic review | Application of disposable diapers in prevention of infant diaper dermatitis |
| DAVIES[ | 2005 | Cochrane | Systematic review | Role of topical vitamin A or its derivatives in the treatment and prevention of infant diaper dermatitis |
| ROWE[ | 2008 | JBI | Systematic review | Effect of barrier preparation on prevention/treatment of diaper dermatitis in infants and preschool children |
| BLUME-PEYTAVI[ | 2014 | DARE | Systematic review | Prevention of diaper dermatitis in infant: a literature review |
| ZHANG[ | 2020 | Medlive | Consensus approach | Expert consensus on nursing practice of infant diaper dermatitis |
| HORII[ | 2019 | UptoDate | Clinical decision | Clinical decision making in the management of diaper dermatitis |
| BMJ[ | 2018 | Best Practice | Clinical decision | An overview of dermatitis |
Tab 1 Characteristics of included studies
| Study | Year | Resource | Type | Theme |
|---|---|---|---|---|
| MATHEW[ | 2021 | JBI | Evidence summary | Management of diaper dermatitis in infants and preschool children |
| BAER[ | 2006 | Cochrane | Systematic review | Application of disposable diapers in prevention of infant diaper dermatitis |
| DAVIES[ | 2005 | Cochrane | Systematic review | Role of topical vitamin A or its derivatives in the treatment and prevention of infant diaper dermatitis |
| ROWE[ | 2008 | JBI | Systematic review | Effect of barrier preparation on prevention/treatment of diaper dermatitis in infants and preschool children |
| BLUME-PEYTAVI[ | 2014 | DARE | Systematic review | Prevention of diaper dermatitis in infant: a literature review |
| ZHANG[ | 2020 | Medlive | Consensus approach | Expert consensus on nursing practice of infant diaper dermatitis |
| HORII[ | 2019 | UptoDate | Clinical decision | Clinical decision making in the management of diaper dermatitis |
| BMJ[ | 2018 | Best Practice | Clinical decision | An overview of dermatitis |
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BAER[ | Y | Y | Y | Y | Y | Y | Y | P | Y | Y | Y | Y | Y | N | Y | Y |
| DAVIES[ | Y | Y | Y | Y | Y | Y | P | Y | Y | N | Y | Y | Y | N | Y | Y |
| ROWE[ | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | N | Y | Y |
| BLUME-PEYTAVI[ | Y | N | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | N | N | N |
Tab 2 Quality evaluation of systematic reviews
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BAER[ | Y | Y | Y | Y | Y | Y | Y | P | Y | Y | Y | Y | Y | N | Y | Y |
| DAVIES[ | Y | Y | Y | Y | Y | Y | P | Y | Y | N | Y | Y | Y | N | Y | Y |
| ROWE[ | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | Y | Y | Y | N | Y | Y |
| BLUME-PEYTAVI[ | Y | N | Y | Y | Y | N | Y | Y | Y | N | Y | Y | Y | N | N | N |
| Evaluation criterion | Result | |
|---|---|---|
| LI[ | ADALAT[ | |
| 1. Whether the inclusion criteria of the sample are clearly defined | Y | N |
| 2. Whether the research object and the research site are described in detail | Y | Y |
| 3. Whether the measurement method of exposure factors has reliability and validity | Y | N/C |
| 4. Whether diseases or health problems are defined by objective and consistent criteria | Y | Y |
| 5. Whether confounding factors are identified | N | N |
| 6. Whether measures are taken to control confounding factors | N | N |
| 7. Whether the measurement method of outcome index has reliability and validity | Y | Y |
| 8. Whether the data analysis methods are appropriate | Y | Y |
Tab 3 Evaluation of cross-sectional studies
| Evaluation criterion | Result | |
|---|---|---|
| LI[ | ADALAT[ | |
| 1. Whether the inclusion criteria of the sample are clearly defined | Y | N |
| 2. Whether the research object and the research site are described in detail | Y | Y |
| 3. Whether the measurement method of exposure factors has reliability and validity | Y | N/C |
| 4. Whether diseases or health problems are defined by objective and consistent criteria | Y | Y |
| 5. Whether confounding factors are identified | N | N |
| 6. Whether measures are taken to control confounding factors | N | N |
| 7. Whether the measurement method of outcome index has reliability and validity | Y | Y |
| 8. Whether the data analysis methods are appropriate | Y | Y |
| Prevention strategy | Evidence | Grade |
|---|---|---|
| Air | 1. There should be a period of nappy-free time each day[ | Ⅴb |
| Barrier | 2. Apply protectant at each diaper change to protect skin from irritants, such as urine and feces[ | Ⅰc |
| 3. It is better to choose a barrier preparation or medicine for external usage with the fewest ingredients, avoiding irritating or allergenic ingredients, such as aromatic agent, preservative, neomycin, boric acid, camphor, phenol, benzocaine and salicylate. Otherwise, it may result in systemic toxicity or methemoglobinemia[ | Ⅰc | |
| 4. Pastes and ointments are usually better than creams and lotions; the adhesion of creams and emulsions is poor and the sealing degree is very low. They often contain aromatics and preservatives as well[ | Ⅰb | |
| 5. Sucralfate can also act as a physical barrier against irritants. It has antibacterial activity, which is useful in the treatment of severe or intractable irritant diaper dermatitis[ | Ⅳd | |
| 6. Olive oil and marigold ointment have similar effect on preventing diaper-related dermatitis[ | Ⅰc | |
| 7. The effect of vitamin A in the prevention of diaper dermatitis is unclear[ | Ⅰc | |
| Cleaning | 8. Dry manure can be gently removed by dipping a cotton ball in paraffin oil[ | Ⅴc |
| 9. Barrier paste doesn’t need to be completely removed at each diaper change, and paraffin oil can be used to assist when necessary[ | Ⅰa | |
| 10. Excessive use of cleaners and excessive friction should be avoided[ | ||
| 11. Warm water (37‒40 ℃) and soft cloth can be used to clean the skin, and baby wipes with the least additive and no aromatic agent, ethanol, fluorescent agent, dyes, and preservatives can be chosen. You should scrub and pat gently on the undamaged skin[ | Ⅰa | |
| 12. Baby wipes should be discontinued if irritation or breakage occurs[ | Ⅴc | |
| 13. The diaper area should be cleaned with a small amount of a gentle cleanser with a physiological pH[ | Ⅴc | |
| 14. In preterm and term newborns, the use of wipe will reduce skin pH value, percutaneous moisture loss and less skin erythema[ | Ⅰc | |
| 15. A separate baby bath should be used to reduce diaper red spots and rough, dry skin[ | Ⅰc | |
| 16. In the case of bathing twice a week, bathing with water alone can improve newborn skin conditions and reduce the incidence of nappy-related dermatitis compared to bathing with water and body gel[ | Ⅰc | |
| Diaper | 17. Disposable diapers are recommended[ | Ⅰa |
| 18. Nappies with hydroscopicity gel are superior to cellulose core nappies, cellulose core diapers are better than cloth diapers, air permeable nappies are superior to air tight nappies, and diapers with permeability stains are better than regular diapers[ | Ⅰa | |
| 19. Using plastic underwear over diapers should be avoided[ | Ⅴc | |
| 20. Diapers should at suitable size and tightness[ | Ⅴb | |
| 21. If the baby is allergic to diapers, a different brand or a soft cotton diaper should be chosen[ | Ⅴb | |
| 22. Frequent diaper changes are effective measures to prevent diaper dermatitis[ | Ⅰa | |
| 23. Diapers should be changed every 2 h (or checked for soiled at least every 2 h), and newborns and children with diarrhea should be changed more frequently [ | Ⅴb | |
| 24. Diapers after defecation immediately should be changed[ | Ⅴb | |
| 25. The diaper should be replaced 1 h after diuretic application[ | Ⅴb | |
| Education | 26. Parents and healthcare personnel should be educated on appropriate exposure, selection of barrier agents, skin cleaning, diaper selection, and timing of diaper change[ | Ⅴb |
Tab 4 Summary of the best evidence on risk screening and prevention strategies for diaper dermatitis in infants
| Prevention strategy | Evidence | Grade |
|---|---|---|
| Air | 1. There should be a period of nappy-free time each day[ | Ⅴb |
| Barrier | 2. Apply protectant at each diaper change to protect skin from irritants, such as urine and feces[ | Ⅰc |
| 3. It is better to choose a barrier preparation or medicine for external usage with the fewest ingredients, avoiding irritating or allergenic ingredients, such as aromatic agent, preservative, neomycin, boric acid, camphor, phenol, benzocaine and salicylate. Otherwise, it may result in systemic toxicity or methemoglobinemia[ | Ⅰc | |
| 4. Pastes and ointments are usually better than creams and lotions; the adhesion of creams and emulsions is poor and the sealing degree is very low. They often contain aromatics and preservatives as well[ | Ⅰb | |
| 5. Sucralfate can also act as a physical barrier against irritants. It has antibacterial activity, which is useful in the treatment of severe or intractable irritant diaper dermatitis[ | Ⅳd | |
| 6. Olive oil and marigold ointment have similar effect on preventing diaper-related dermatitis[ | Ⅰc | |
| 7. The effect of vitamin A in the prevention of diaper dermatitis is unclear[ | Ⅰc | |
| Cleaning | 8. Dry manure can be gently removed by dipping a cotton ball in paraffin oil[ | Ⅴc |
| 9. Barrier paste doesn’t need to be completely removed at each diaper change, and paraffin oil can be used to assist when necessary[ | Ⅰa | |
| 10. Excessive use of cleaners and excessive friction should be avoided[ | ||
| 11. Warm water (37‒40 ℃) and soft cloth can be used to clean the skin, and baby wipes with the least additive and no aromatic agent, ethanol, fluorescent agent, dyes, and preservatives can be chosen. You should scrub and pat gently on the undamaged skin[ | Ⅰa | |
| 12. Baby wipes should be discontinued if irritation or breakage occurs[ | Ⅴc | |
| 13. The diaper area should be cleaned with a small amount of a gentle cleanser with a physiological pH[ | Ⅴc | |
| 14. In preterm and term newborns, the use of wipe will reduce skin pH value, percutaneous moisture loss and less skin erythema[ | Ⅰc | |
| 15. A separate baby bath should be used to reduce diaper red spots and rough, dry skin[ | Ⅰc | |
| 16. In the case of bathing twice a week, bathing with water alone can improve newborn skin conditions and reduce the incidence of nappy-related dermatitis compared to bathing with water and body gel[ | Ⅰc | |
| Diaper | 17. Disposable diapers are recommended[ | Ⅰa |
| 18. Nappies with hydroscopicity gel are superior to cellulose core nappies, cellulose core diapers are better than cloth diapers, air permeable nappies are superior to air tight nappies, and diapers with permeability stains are better than regular diapers[ | Ⅰa | |
| 19. Using plastic underwear over diapers should be avoided[ | Ⅴc | |
| 20. Diapers should at suitable size and tightness[ | Ⅴb | |
| 21. If the baby is allergic to diapers, a different brand or a soft cotton diaper should be chosen[ | Ⅴb | |
| 22. Frequent diaper changes are effective measures to prevent diaper dermatitis[ | Ⅰa | |
| 23. Diapers should be changed every 2 h (or checked for soiled at least every 2 h), and newborns and children with diarrhea should be changed more frequently [ | Ⅴb | |
| 24. Diapers after defecation immediately should be changed[ | Ⅴb | |
| 25. The diaper should be replaced 1 h after diuretic application[ | Ⅴb | |
| Education | 26. Parents and healthcare personnel should be educated on appropriate exposure, selection of barrier agents, skin cleaning, diaper selection, and timing of diaper change[ | Ⅴb |
| 1 | 梅建国. 儿童护理[M]. 北京: 高等教育出版社, 2005. |
| 2 | COHEN B. Differential diagnosis of diaper dermatitis[J]. Clin Pediatr (Phila), 2017, 56(5_suppl): 16S-22S. |
| 3 | ŠIKIĆ P M, MAVER U, MARČUN V N, et al. Diagnosis and management of diaper dermatitis in infants with emphasis on skin microbiota in the diaper area[J]. Int J Dermatol, 2018, 57(3): 265-275. |
| 4 | O'CONNOR R J, SANCHEZ V, WANG Y, et al. Evaluation of the impact of 2 disposable diapers in the “Natural” diaper category on diapered skin condition[J]. Clin Pediatr (Phila), 2019, 58(7): 806-815. |
| 5 | LI C H, ZHU Z H, DAI Y H. Diaper dermatitis: a survey of risk factors for children aged 1-24 months in China[J]. J Int Med Res, 2012, 40(5): 1752-1760. |
| 6 | SUKHNEEWAT C, CHAIYARIT J, TECHASATIAN L. Diaper dermatitis: a survey of risk factors in Thai children aged under 24 months[J]. BMC Dermatol, 2019, 19(1): 7. |
| 7 | 郭一峰, 李萍, 汤建萍, 等. 中国12城市0~7岁儿童皮肤病患病率调查[J]. 中华皮肤科杂志, 2017, 50(11): 790-794. |
| 8 | 李彩虹, 朱宗涵, 戴耀华. 0~24月龄婴幼儿家庭养育情况调查[J]. 中国妇幼健康研究, 2012, 23(3): 253-255, 264. |
| 9 | CARR A N, DEWITT T, CORK M J, et al. Diaper dermatitis prevalence and severity: global perspective on the impact of caregiver behavior[J]. Pediatr Dermatol, 2020, 37(1): 130-136. |
| 10 | 姜妍, 尹小兵, 李娜, 等. 婴幼儿尿布性皮炎影响因素及预防的研究进展[J]. 护士进修杂志, 2021, 36(10): 906-910. |
| 11 | DICENSO A, BAYLEY L, HAYNES R B. Accessing pre-appraised evidence: fine-tuning the 5S model into a 6S model[J]. Evid Based Nurs, 2009, 12(4): 99-101. |
| 12 | PIEPER D, KOENSGEN N, BREUING J, et al. How is AMSTAR applied by authors-a call for better reporting[J]. BMC Med Res Methodol, 2018, 18(1): 56. |
| 13 | MCARTHUR A, KLUGÁROVÁ J, YAN H, et al. Innovations in the systematic review of text and opinion[J]. Int J Evid Based Healthc, 2015, 13(3): 188-195. |
| 14 | 王春青, 胡雁. JBI证据预分级及证据推荐级别系统(2014版)[J]. 护士进修杂志, 2015, 30(11): 964-967. |
| 15 | MATHEW S. Diaper dermatitis (infants and preschool): management[EB/OL]. (2021-04-19) [2021-06-30]. http://ovidsp.dc2.ovid.com/ovid-a/ovidweb.cgi?&S=DNHDFPCPLMEBLBEGJPPJNHBFMA GOAA00&Complete+Reference=S.sh.83%7c6%7c1&Counter5=SS_view_found_complete%7cJBI1296%7cjbi%7cjbidb%7cjbi&Counter 5Data=JBI1296%7cjbi%7cjbidb%7cjbi. |
| 16 | BAER E L, DAVIES M W, EASTERBROOK K J. Disposable nappies for preventing napkin dermatitis in infants[J]. Cochrane Database Syst Rev, 2006, 2006(3): CD004262. |
| 17 | DAVIES M W, DORE A J, PERISSINOTTO K L. Topical vitamin A, or its derivatives, for treating and preventing napkin dermatitis in infants[J]. Cochrane Database Syst Rev, 2005, 2005(4): CD004300. |
| 18 | ROWE J, MCCALL E, KENT B. Clinical effectiveness of barrier preparations in the prevention and treatment of nappy dermatitis in infants and preschool children of nappy age[J]. Int J Evid Based Healthc, 2008, 6(1): 3-23. |
| 19 | BLUME-PEYTAVI U, HAUSER M, LÜNNEMANN L, et al. Prevention of diaper dermatitis in infants: a literature review[J]. Pediatr Dermatol, 2014, 31(4): 413-429. |
| 20 | 张琳琪, 李杨, 宋楠, 等. 婴幼儿尿布性皮炎护理实践专家共识[J].中华护理杂志, 2020, 55(8): 1169. |
| 21 | HORII K A, PROSSICK T A. Diaper dermatitis[EB/OL]. (2019-11-08) [2021-06-30]. https://www.uptodate.com/contents/zh-Hans/diaper-dermatitis?search=diaper%20dermatitis&source=search_result&selectedTitle=1~107&usage_type=default&display_rank=1#. |
| 22 | Overview of dermatitis[EB/OL]. (2018-10-16) [2021-06-30]. https://bestpractice.bmj.com/topics/en-gb/88#referencePop19. |
| 23 | LAVENDER T, FURBER C, CAMPBELL M, et al. Effect on skin hydration of using baby wipes to clean the napkin area of newborn babies: assessor-blinded randomised controlled equivalence trial[J]. BMC Pediatr, 2012, 12: 59. |
| 24 | ADALAT S, WALL D, GOODYEAR H. Diaper dermatitis-frequency and contributory factors in hospital attending children[J]. Pediatr Dermatol, 2007, 24(5): 483-488. |
| 25 | 周英凤, 顾莺, 胡雁, 等. JBI循证卫生保健中心关于不同类型研究的质量评价工具: 干预性研究的质量评价[J]. 护士进修杂志, 2018, 33(1): 24-26. |
| 26 | 周英凤, 顾莺, 胡雁, 等. JBI循证卫生保健中心对关于不同类型研究的质量评价工具: 患病率及分析性横断面研究的质量评价[J]. 护士进修杂志, 2018, 33(3): 219-221. |
| 27 | ATHERTON D J. A review of the pathophysiology, prevention and treatment of irritant diaper dermatitis[J]. Curr Med Res Opin, 2004, 20(5): 645-649. |
| 28 | BOIKO S. Making rash decisions in the diaper area[J]. Pediatr Ann, 2000, 29(1): 50-56. |
| 29 | SHIN H T. Diaper dermatitis that does not quit[J]. Dermatol Ther, 2005, 18(2): 124-135. |
| 30 | FURBER C, BEDWELL C, CAMPBELL M, et al. The challenges and realties of diaper area cleansing for parents[J]. J Obstet Gynecol Neonatal Nurs, 2012, 41(6): E13-E25. |
| 31 | 乐琼, 张岚, 吴丽芬, 等. 新生儿尿布皮炎结构化管理流程的制订及应用[J]. 护理学报, 2019, 26(19): 22-26. |
| 32 | ROY S,MOLLAH M A H,MANNAN M A, et al. Hazards of wearing diaper among infants[J]. J Bangladesh Coll Phys Surg, 2017, 35(4): 170-173. |
| 33 | 陈羽双, 杨斯钰, 黄玉婷, 等. 新生儿尿布皮炎的影响因素及预防进展[J]. 中国儿童保健杂志, 2021, 29(3): 277-280, 284. |
| 34 | FUTAMURA M, ITO K, OTSUJI K, et al. Effects of “Skin Care School,” a parental education program on childhood atopic dermatitis conducted during short hospitalization stays[J]. Arerugi, 2009, 58(12): 1610-1618. |
| [1] | Xu Yulin, Du Bowen, Wang Jian, Sun Kun. Review of impact of maternal perinatal mental health on offspring cardiovascular system [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(3): 408-414. |
| [2] | ZHU Hanjing, GUO Yan, YIN Hongfan, WANG Beibei, XIE Juan, YANG Yan. Best evidence summary of weight management in patients undergoing endocrine therapy for prostate cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(2): 194-203. |
| [3] | CAO Siyao, LIU Jieqiong, WANG Guangshuai, WANG Guanghai. Research progress in preemptive screening and intervention for autism spectrum disorder in infancy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(2): 222-227. |
| [4] | LI Yibai, CUI Ruiji, GAO Shan, HU Jiajin, GUO Xiaoying. Research progress in late-onset group B Streptococcus infection in infants and its prevention [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(8): 1044-1049. |
| [5] | CUI Fangming, WANG Jingna, ZHANG Yuxia. Clinical effect of oral motor training combined with pediatric tui-na on feeding intolerance in preterm infants [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(8): 975-980. |
| [6] | YANG Liling, ZHAN Sha, XUE Xiaoyan, CHEN Kai, LIU Qing, WANG Li, WANG Yiyi, WU Meng, LU Qunfeng. Development of indicators and analysis of barriers for assessment and prevention of cutaneous graft-versus-host disease after haematopoietic stem cell transplantation in children [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(12): 1552-1560. |
| [7] | MA Jinqian, FAN Pianpian, ZHENG Tao, ZHANG Lin, CHEN Yuanzhi, SHEN Jian, OUYANG Fengxiu. Relationship among maternal gut, vaginal microbiota and microbiota in meconium and vernix caseosa in newborns [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(1): 50-63. |
| [8] | WU Kaimin, MA Jing, ZHAO Xuyun. Combined effects of intermittent fasting and thermogenic fat activation on the treatment and prevention of obesity in mice [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(9): 1131-1144. |
| [9] | CHEN Hui, ZHU Weiyi, YAO Yijin. A meta-analysis of the effects of levothyroxine dose adjustment on maternal and infant outcomes in pregnant women with hypothyroidism [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(7): 906-915. |
| [10] | JIANG Xinting, HUANG Gaozhong. Research progress in the effect of nutritional intervention on cognitive impairment related to Alzheimer's disease [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(6): 788-794. |
| [11] | SHEN Li, HUANG Hengye, YU Guangjun. Current status of neurodevelopmental outcomes and its influencing factors of early-to-moderate preterm infants at corrected age of 18 months [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(4): 445-452. |
| [12] | SHA Pan, ZHAO Xuewen, ZHU Haotian, GAO Chongzhou, LIU Shen. Research progress in the mechanism and intervention of tendon adhesion [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(8): 1116-1121. |
| [13] | LI Guodong, YAN Shaohua, ZHANG Qiuxia, LEI Li, ZHANG Xinlu, LIANG Hongbin, LU Junyan, XIAO Min, LUO Wei, PU Jun, XIU Jiancheng. Evaluation of the application effect of “Internet+”-based “co-prevention and co-management” health management model for cardio-cerebrovascular diseases on the improvement of blood pressure in target surveillance population in community [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(6): 797-804. |
| [14] | WU Shiyin, CAI Meiqin. Summary of clinical research of Pediococcus pentosaceus in treatment of infantile colic [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(11): 1633-1637. |
| [15] | Wen YIN, Teng WANG, Yu-xi ZHOU, Yan-nan HANG, Da-xiang WEN. Pharmacodynamics of cisatracurium intravenously infused in infants and young children undergoing living donor liver transplantation [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2021, 41(6): 761-763. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||