Journal of Shanghai Jiao Tong University (Medical Science) ›› 2022, Vol. 42 ›› Issue (12): 1712-1719.doi: 10.3969/j.issn.1674-8115.2022.12.009
• Clinical research • Previous Articles Next Articles
WEI Yifan( ), ZHU Yueniu, KONG Xiangmei, XU Yaya, ZHU Xiaodong()
), ZHU Yueniu, KONG Xiangmei, XU Yaya, ZHU Xiaodong()
Received:2022-07-15
Accepted:2022-12-15
Online:2022-12-28
Published:2022-12-28
Contact:
ZHU Xiaodong
E-mail:weiyifan1994s@163.com;xinhuaxiaodong@126.com
CLC Number:
WEI Yifan, ZHU Yueniu, KONG Xiangmei, XU Yaya, ZHU Xiaodong. Effects of early mechanical ventilation on the morphology and function of the diaphragm in children[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(12): 1712-1719.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2022.12.009
| Indicator | M(Q1, Q3)/n(%) |
|---|---|
| General data | |
| Age/year | 2.94 (1.35, 7.00) |
| Male/female/n(%) | 23 (50.00)/23 (50.00) |
| Height/cm | 97.50 (78.00, 115.00) |
| Weight/kg | 13.08 (10.00, 22.00) |
| BMI/(kg·m-2) | 15.94 (13.55, 17.85) |
| Baseline abdominal fat thickness/mm | 0.70 (0.57, 0.89) |
| Abdominal fat atrophy/n(%) | 23 (50.00) |
| Body surface area/m2 | 0.60 (0.43, 0.87) |
| Clinical score system | |
| PCIS | 88.00 (79.00, 94.00) |
| PRISM Ⅲ | 6.00 (3.00, 10.00) |
| Primary disease | |
| Respiratory diseases/n(%) | 10 (21.74) |
| Neurological diseases/n(%) | 20 (43.48) |
| Hematologic diseases/n(%) | 4 (8.70) |
| Digestive diseases/n(%) | 5 (10.87) |
| Musculoskeletal diseases/n(%) | 1 (2.17) |
| Urinary diseases/n(%) | 1 (2.17) |
| Endocrine diseases/n(%) | 5 (10.87) |
| Etiology | |
| Pneumonia/n(%) | 24 (52.17) |
| CNS lesions/n(%) | 16 (34.78) |
| Septic pyemia/n(%) | 6 (13.04) |
| Complication | |
| MODS/n(%) | 6 (13.04) |
| Treatment | |
| Glucocorticoid/n(%) | 43 (93.50) |
| Parenteral nutrition/n(%) | 7 (15.22) |
| Fasting/n(%) | 10 (21.74) |
| Surgical interventions/n(%) | 26 (56.52) |
| Prognosis | |
| Weaning failure/n(%) | 18 (39.13) |
| Mortality in PICU/n(%) | 10 (21.74) |
| Duration of mechanical ventilation/d | 8.00 (7.00, 12.00) |
| Hospitalization days in PICU/d | 20.00 (11.00, 31.00) |
Tab 1 Main clinical characteristics of 46 children
| Indicator | M(Q1, Q3)/n(%) |
|---|---|
| General data | |
| Age/year | 2.94 (1.35, 7.00) |
| Male/female/n(%) | 23 (50.00)/23 (50.00) |
| Height/cm | 97.50 (78.00, 115.00) |
| Weight/kg | 13.08 (10.00, 22.00) |
| BMI/(kg·m-2) | 15.94 (13.55, 17.85) |
| Baseline abdominal fat thickness/mm | 0.70 (0.57, 0.89) |
| Abdominal fat atrophy/n(%) | 23 (50.00) |
| Body surface area/m2 | 0.60 (0.43, 0.87) |
| Clinical score system | |
| PCIS | 88.00 (79.00, 94.00) |
| PRISM Ⅲ | 6.00 (3.00, 10.00) |
| Primary disease | |
| Respiratory diseases/n(%) | 10 (21.74) |
| Neurological diseases/n(%) | 20 (43.48) |
| Hematologic diseases/n(%) | 4 (8.70) |
| Digestive diseases/n(%) | 5 (10.87) |
| Musculoskeletal diseases/n(%) | 1 (2.17) |
| Urinary diseases/n(%) | 1 (2.17) |
| Endocrine diseases/n(%) | 5 (10.87) |
| Etiology | |
| Pneumonia/n(%) | 24 (52.17) |
| CNS lesions/n(%) | 16 (34.78) |
| Septic pyemia/n(%) | 6 (13.04) |
| Complication | |
| MODS/n(%) | 6 (13.04) |
| Treatment | |
| Glucocorticoid/n(%) | 43 (93.50) |
| Parenteral nutrition/n(%) | 7 (15.22) |
| Fasting/n(%) | 10 (21.74) |
| Surgical interventions/n(%) | 26 (56.52) |
| Prognosis | |
| Weaning failure/n(%) | 18 (39.13) |
| Mortality in PICU/n(%) | 10 (21.74) |
| Duration of mechanical ventilation/d | 8.00 (7.00, 12.00) |
| Hospitalization days in PICU/d | 20.00 (11.00, 31.00) |
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Oxygenation status | |||||
| SaO2/% | 97.80 (95.2, 99.40) | 97.00 (91.63, 99.23) | 97.50 (89.80, 99.23) | 0.73 | 0.70 |
| OI/mmHg | 349.55±166.03 | 305.97±159.04 | 321.24±161.00 | 0.90 | 0.41 |
| PaCO2/mmHg | 42.32±8.60 | 44.44±10.85 | 43.23±8.37 | 0.60 | 0.55 |
| Ventilator parameter | |||||
| Ppeak/cmH2O | 17.61±4.43 | 16.72±4.04 | 16.04±3.83 | 1.46 | 0.24 |
| Pmean/cmH2O | 8.83±3.48 | 8.26±3.28 | 7.49±2.60 | 1.78 | 0.17 |
| PEEP/cmH2O | 4.57±1.91 | 4.46±1.72 | 4.04±1.45 | 0.89 | 0.42 |
| FiO2/% | 36.76±11.43 | 35.07±10.63 | 34.40±10.12 | 0.39 | 0.68 |
| MVe/(L·min-1) | 3.38±1.83 | 3.21±1.64 | 3.03±1.48 | 0.42 | 0.66 |
| TV/(mL·kg-1) | 7.54±3.31 | 7.44±2.89 | 7.04±2.85 | 2.50 | 0.09 |
Tab 2 Comparison of the oxygenation status of children in PICU and the ventilator parameter settings at multiple time points after mechanical ventilation
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Oxygenation status | |||||
| SaO2/% | 97.80 (95.2, 99.40) | 97.00 (91.63, 99.23) | 97.50 (89.80, 99.23) | 0.73 | 0.70 |
| OI/mmHg | 349.55±166.03 | 305.97±159.04 | 321.24±161.00 | 0.90 | 0.41 |
| PaCO2/mmHg | 42.32±8.60 | 44.44±10.85 | 43.23±8.37 | 0.60 | 0.55 |
| Ventilator parameter | |||||
| Ppeak/cmH2O | 17.61±4.43 | 16.72±4.04 | 16.04±3.83 | 1.46 | 0.24 |
| Pmean/cmH2O | 8.83±3.48 | 8.26±3.28 | 7.49±2.60 | 1.78 | 0.17 |
| PEEP/cmH2O | 4.57±1.91 | 4.46±1.72 | 4.04±1.45 | 0.89 | 0.42 |
| FiO2/% | 36.76±11.43 | 35.07±10.63 | 34.40±10.12 | 0.39 | 0.68 |
| MVe/(L·min-1) | 3.38±1.83 | 3.21±1.64 | 3.03±1.48 | 0.42 | 0.66 |
| TV/(mL·kg-1) | 7.54±3.31 | 7.44±2.89 | 7.04±2.85 | 2.50 | 0.09 |
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Thickness /cm | 0.69 (0.56, 0.90) | 0.74 (0.57, 0.89) | 0.70 (0.56, 0.91) | 1.06 | 0.59 |
| Atrophy rate /% | 0 (0, 0) | -1.30 (-8.80, 5.77) | 0 (-6.92, 7.81) | 1.06 | 0.59 |
Tab 3 Comparison of the abdominal subcutaneous fat of children in PICU during 96 h of mechanical ventilation
| Indicator | MV | H value | P value | ||
|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | |||
| Thickness /cm | 0.69 (0.56, 0.90) | 0.74 (0.57, 0.89) | 0.70 (0.56, 0.91) | 1.06 | 0.59 |
| Atrophy rate /% | 0 (0, 0) | -1.30 (-8.80, 5.77) | 0 (-6.92, 7.81) | 1.06 | 0.59 |
| Indicator | Position | MV | H value | P value | ||
|---|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | ||||
| Diaphragmatic thickness/mm | R-I | 2.82±0.73 | 2.68±0.70 | 2.57±0.65 | 38.68 | 0.000 |
| R-E | 2.47±0.66 | 2.36±0.64 | 2.26±0.58 | 43.92 | 0.000 | |
| L-I | 2.58±0.71 | 2.46±0.70 | 2.35±0.67 | 37.19 | 0.000 | |
| L-E | 2.25±0.62 | 2.16±0.60 | 2.08±0.59 | 44.38 | 0.000 | |
| DE/mm | R | 6.20 (4.09, 8.60) | 5.85 (3.79, 7.72) | 6.09 (4.96, 7.89) | 2.48 | 0.290 |
| L | 5.60 (3.95, 7.25) | 6.15 (4.23, 9.40) | 5.75 (4.10, 8.86) | 4.19 | 0.120 | |
| DCV/(mm·s-1) | R | 6.59±3.61 | 5.35±2.83 | 6.79±4.09 | 4.74 | 0.090 |
| L | 6.28±3.73 | 6.16±3.43 | 6.42±3.49 | 1.65 | 0.440 | |
| DTF/% | R | 14.28±4.98 | 13.85±5.52 | 13.43±5.02 | 0.54 | 0.760 |
| L | 14.75±5.70 | 13.64±4.44 | 13.37±4.77 | 0.84 | 0.660 | |
| DAR/% | R | ‒ | 4.27±7.36 | 7.69±7.74 | 43.92 | 0.000 |
| L | ‒ | 3.88±6.85 | 7.55±7.69 | 37.19 | 0.000 | |
Tab 4 Comparison of the diaphragmatic bedside ultrasound data of children in PICU during early-stage mechanical ventilation
| Indicator | Position | MV | H value | P value | ||
|---|---|---|---|---|---|---|
| 0 h | 48 h | 96 h | ||||
| Diaphragmatic thickness/mm | R-I | 2.82±0.73 | 2.68±0.70 | 2.57±0.65 | 38.68 | 0.000 |
| R-E | 2.47±0.66 | 2.36±0.64 | 2.26±0.58 | 43.92 | 0.000 | |
| L-I | 2.58±0.71 | 2.46±0.70 | 2.35±0.67 | 37.19 | 0.000 | |
| L-E | 2.25±0.62 | 2.16±0.60 | 2.08±0.59 | 44.38 | 0.000 | |
| DE/mm | R | 6.20 (4.09, 8.60) | 5.85 (3.79, 7.72) | 6.09 (4.96, 7.89) | 2.48 | 0.290 |
| L | 5.60 (3.95, 7.25) | 6.15 (4.23, 9.40) | 5.75 (4.10, 8.86) | 4.19 | 0.120 | |
| DCV/(mm·s-1) | R | 6.59±3.61 | 5.35±2.83 | 6.79±4.09 | 4.74 | 0.090 |
| L | 6.28±3.73 | 6.16±3.43 | 6.42±3.49 | 1.65 | 0.440 | |
| DTF/% | R | 14.28±4.98 | 13.85±5.52 | 13.43±5.02 | 0.54 | 0.760 |
| L | 14.75±5.70 | 13.64±4.44 | 13.37±4.77 | 0.84 | 0.660 | |
| DAR/% | R | ‒ | 4.27±7.36 | 7.69±7.74 | 43.92 | 0.000 |
| L | ‒ | 3.88±6.85 | 7.55±7.69 | 37.19 | 0.000 | |
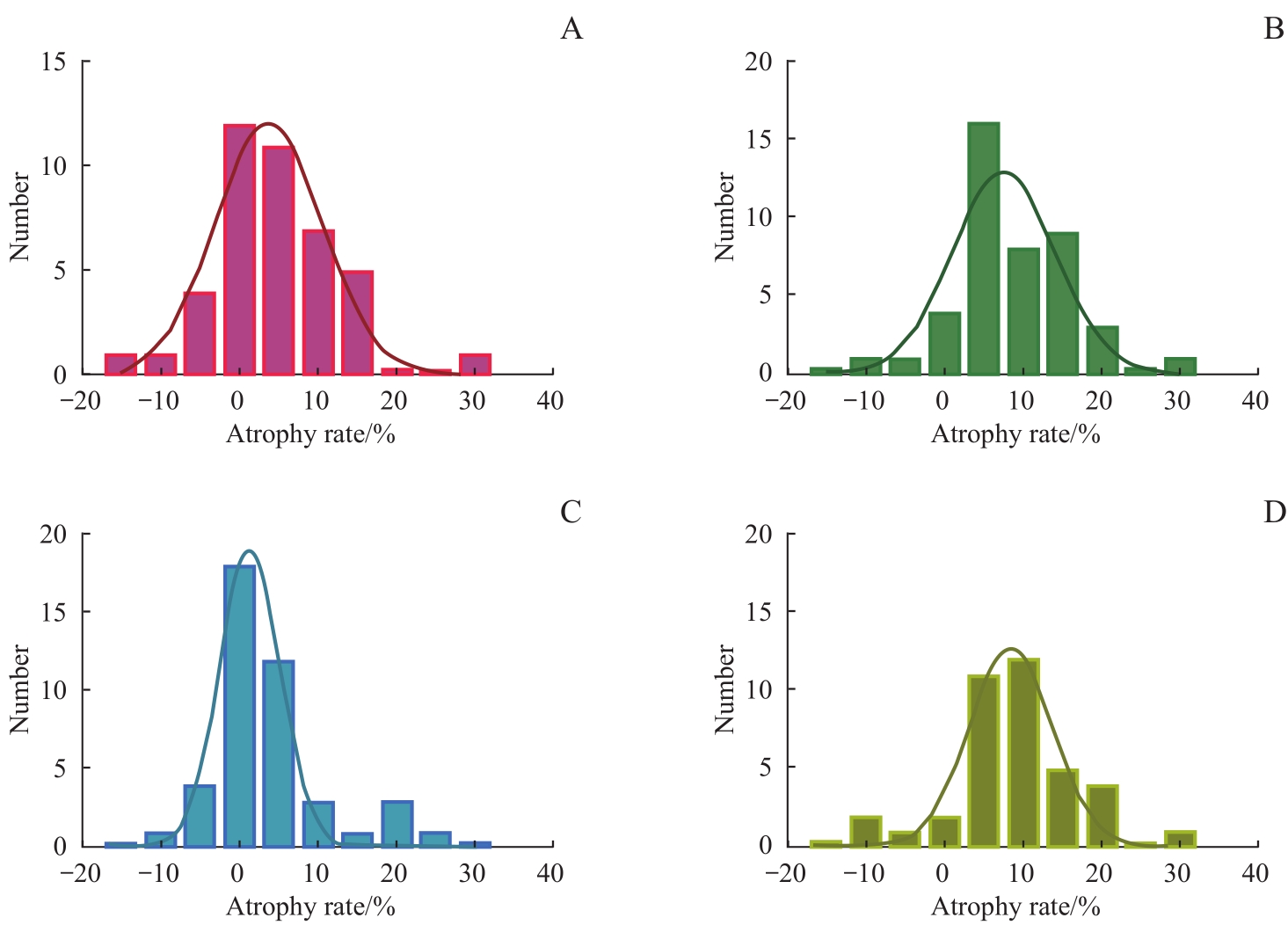
Fig1 Distribution of diaphragm atrophy rate after 48 h and 96 h of mechanical ventilation
| 1 | TOBIN M J, LAGHI F, JUBRAN A. Narrative review: ventilator-induced respiratory muscle weakness[J]. Ann Intern Med, 2010, 153(4): 240-245. |
| 2 | DE JONGHE B, BASTUJI-GARIN S, DURAND M C, et al. Respiratory weakness is associated with limb weakness and delayed weaning in critical illness[J]. Crit Care Med, 2007, 35(9): 2007-2015. |
| 3 | DEMOULE A, MOLINARI N, JUNG B, et al. Patterns of diaphragm function in critically ill patients receiving prolonged mechanical ventilation: a prospective longitudinal study[J]. Ann Inten Care, 2016, 6(1): 75. |
| 4 | BÉDUNEAU G, PHAM T, SCHORTGEN F, et al. Epidemiology of weaning outcome according to a new definition. the WIND study[J]. Am J Respir Crit Care Med, 2017, 195(6): 772-783. |
| 5 | DRES M, DUBÉ B P, MAYAUX J, et al. Coexistence and impact of limb muscle and diaphragm weakness at time of liberation from mechanical ventilation in medical intensive care unit patients[J]. Am J Respir Crit Care Med, 2017, 195(1): 57-66. |
| 6 | KIM W Y, SUH H J, HONG S B, et al. Diaphragm dysfunction assessed by ultrasonography: influence on weaning from mechanical ventilation[J]. Crit Care Med, 2011, 39(12): 2627-2630. |
| 7 | GOLIGHER E C, DRES M, FAN E, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes[J]. Am J Respir Crit Care Med, 2018, 197(2): 204-213. |
| 8 | DAMUTH E, MITCHELL J A, BARTOCK J L, et al. Long-term survival of critically ill patients treated with prolonged mechanical ventilation: a systematic review and meta-analysis[J]. Lancet Respir Med, 2015, 3(7): 544-553. |
| 9 | GROSU H B, LEE Y I, LEE J, et al. Diaphragm muscle thinning in patients who are mechanically ventilated[J]. Chest, 2012, 142(6): 1455-1460. |
| 10 | LEVINE S, NGUYEN T, TAYLOR N, et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans[J]. N Engl J Med, 2008, 358(13): 1327-1335. |
| 11 | POWERS S K, SHANELY R A, COOMBES J S, et al. Mechanical ventilation results in progressive contractile dysfunction in the diaphragm[J]. J Appl Physiol (1985), 2002, 92(5): 1851-1858. |
| 12 | JABER S, PETROF B J, JUNG B, et al. Rapidly progressive diaphragmatic weakness and injury during mechanical ventilation in humans[J]. Am J Respir Crit Care Med, 2011, 183(3): 364-371. |
| 13 | SHANELY R A, ZERGEROGLU M A, LENNON SL, et al. Mechanical ventilation-induced diaphragmatic atrophy is associated with oxidative injury and increased proteolytic activity[J]. Am J Respir Crit Care Med, 2002, 166(10): 1369-1374. |
| 14 | GOLIGHER E C, FAN E, HERRIDGE M S, et al. Evolution of diaphragm thickness during mechanical ventilation. impact of inspiratory effort[J]. Am J Respir Crit Care Med, 2015, 192(9): 1080-1088. |
| 15 | OROZCO-LEVI M, LLORETA J, MINGUELLA J, et al. Injury of the human diaphragm associated with exertion and chronic obstructive pulmonary disease[J]. Am J Respir Crit Care Med, 2001, 164(9): 1734-1739. |
| 16 | GOLIGHER E C, LAGHI F, DETSKY M E, et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity[J]. Intensive Care Med, 2015, 41(4): 642-649. |
| 17 | FAYSSOIL A, BEHIN A, OGNA A, et al. Diaphragm: pathophysiology and ultrasound imaging in neuromuscular disorders[J]. J Neuromuscul Dis, 2018, 5(1): 1-10. |
| 18 | FARIAS J A, FRUTOS F, ESTEBAN A, et al. What is the daily practice of mechanical ventilation in pediatric intensive care units? A multicenter study[J]. Intensive Care Med, 2004, 30(5): 918-925. |
| 19 | TAKAZAKURA R, TAKAHASHI M, NITTA N, et al. Diaphragmatic motion in the sitting and supine positions: healthy subject study using a vertically open magnetic resonance system[J]. J Magn Reson Imaging, 2004, 19(5): 605-609. |
| 20 | YAMAGUTI W P, PAULIN E, SHIBAO S, et al. Ultrasound evaluation of diaphragmatic mobility in different postures in healthy subjects[J]. J Bras Pneumol, 2007, 33(4): 407-413. |
| 21 | VIVIER E, MEKONTSO DESSAP A, DIMASSI S, et al. Diaphragm ultrasonography to estimate the work of breathing during non-invasive ventilation[J]. Intensive Care Med, 2012, 38(5): 796-803. |
| 22 | MATAMIS D, SOILEMEZI E, TSAGOURIAS M, et al. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications[J]. Intensive Care Med, 2013, 39(5): 801-810. |
| 23 | MCCOOL F D, CONOMOS P, BENDITT J O, et al. Maximal inspiratory pressures and dimensions of the diaphragm[J]. Am J Respir Crit Care Med, 1997, 155(4): 1329-1334. |
| 24 | COHN D, BENDITT J O, EVELOFF S, et al. Diaphragm thickening during inspiration[J]. J Appl Physiol (1985), 1997, 83(1): 291-296. |
| 25 | LIU Y Y, LI L F. Ventilator-induced diaphragm dysfunction in critical illness[J]. Exp Biol Med (Maywood), 2018, 243(17/18): 1329-1337. |
| 26 | POWERS S K, WIGGS M P, SOLLANEK K J, et al. Ventilator-induced diaphragm dysfunction: cause and effect[J]. Am J Physiol Regul Integr Comp Physiol, 2013, 305(5): R464-R477. |
| 27 | POWERS S K, KAVAZIS A N, LEVINE S. Prolonged mechanical ventilation alters diaphragmatic structure and function[J]. Crit Care Med, 2009, 37(10 Suppl): S347-S353. |
| 28 | SCHEPENS T, VERBRUGGHE W, DAMS K, et al. The course of diaphragm atrophy in ventilated patients assessed with ultrasound: a longitudinal cohort study[J]. Crit Care, 2015, 19: 422. |
| 29 | IJLAND M M, LEMSON J, VAN DER HOEVEN J G, et al. The impact of critical illness on the expiratory muscles and the diaphragm assessed by ultrasound in mechanical ventilated children[J]. Ann Intensive Care, 2020, 10(1): 115. |
| 30 | GLAU C L, CONLON T W, HIMEBAUCH A S, et al. Progressive diaphragm atrophy in pediatric acute respiratory failure[J]. Pediatr Crit Care Med, 2018, 19(5): 406-411. |
| 31 | JOHNSON R W, NG K W P, DIETZ A R, et al. Muscle atrophy in mechanically-ventilated critically ill children[J]. PLoS One, 2018, 13(12): e0207720. |
| 32 | LEE E P, HSIA S H, HSIAO H F, et al. Evaluation of diaphragmatic function in mechanically ventilated children: an ultrasound study[J]. PLoS One, 2017, 12(8): e0183560. |
| 33 | GRASSI A, FERLICCA D, LUPIERI E, et al. Assisted mechanical ventilation promotes recovery of diaphragmatic thickness in critically ill patients: a prospective observational study[J]. Crit Care, 2020, 24: 85. |
| 34 | ZAMBON M, BECCARIA P, MATSUNO J, et al. Mechanical ventilation and diaphragmatic atrophy in critically ill patients: an ultrasound study[J]. Crit Care Med, 2016, 44(7): 1347-1352. |
| 35 | POWERS S K, DECRAMER M, GAYAN-RAMIREZ G, et al. Pressure support ventilation attenuates ventilator-induced protein modifications in the diaphragm[J]. Crit Care, 2008, 12(6): 191. |
| 36 | DEVOTO G, GALLO F, MARCHELLO C, et al. Prealbumin serum concentrations as a useful tool in the assessment of malnutrition in hospitalized patients[J]. Clin Chem, 2006, 52(12): 2281-2285. |
| 37 | JIANG J R. Ultrasonographic evaluation of liver/spleen movements and extubation outcome[J]. Chest, 2004, 126(1): 179-185. |
| 38 | SUMMERHILL E M, EL-SAMEED Y A, GLIDDEN T J, et al. Monitoring recovery from diaphragm paralysis with ultrasound[J]. Chest, 2008, 133(3): 737-743. |
| 39 | DININO E, GARTMAN E J, SETHI J M, et al. Diaphragm ultrasound as a predictor of successful extubation from mechanical ventilation[J]. Thorax, 2014, 69(5): 423-427. |
| 40 | FARGHALY S, HASAN A A. Diaphragm ultrasound as a new method to predict extubation outcome in mechanically ventilated patients[J]. Aust Crit Care, 2017, 30(1): 37-43. |
| 41 | GOTTESMAN E, MCCOOL F D. Ultrasound evaluation of the paralyzed diaphragm[J]. Am J Respir Crit Care Med, 1997, 155(5): 1570-1574. |
| 42 | ZAMBON M, GRECO M, BOCCHINO S, et al. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: a systematic review[J]. Intensive Care Med, 2017, 43(1): 29-38. |
| 43 | NEWTH C J L, VENKATARAMAN S, WILLSON D F, et al. Weaning and extubation readiness in pediatric patients[J]. Pediatr Crit Care Med, 2009, 10(1): 1-11. |
| 44 | DOORDUIN J, VAN HEES H W H, VAN DER HOEVEN J G, et al. Monitoring of the respiratory muscles in the critically ill[J]. Am J Respir Crit Care Med, 2013, 187(1): 20-27. |
| 45 | CATTAPAN S E, LAGHI F, TOBIN M J. Can diaphragmatic contractility be assessed by airway twitch pressure in mechanically ventilated patients? [J]. Thorax, 2003, 58(1): 58-62. |
| [1] | Wang Shaoyan, Li Chao, Huang Shuo, Wu Shuqi, Chen Suyun. Physiological distribution characteristics and influencing factors of hepatic background and mediastinal blood pool on 18F-FDG PET/CT in children and adolescents of different ages [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(4): 496-501. |
| [2] | Writing Group of Chinese Expert Consensus on Ultrasound-Guided Pediatric Nerve Blocks in Children (2025 edition) . Chinese expert consensus on ultrasound-guided nerve blocks in children (2025 edition) [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(9): 1079-1098. |
| [3] | SHEN Haoliang, YUAN Kaihao, YU Lei, YANG Nana, WANG Yiping, ZHAO Hongsheng, GUO Fengmei, SUN Chenliang. Value of combined diaphragm and intercostal muscle ultrasonography in guiding weaning assessment in mechanically ventilated patients with sepsis [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(2): 186-193. |
| [4] | LIU Meiling, ZHOU Yabing, WANG Xiaoqiang. Advances in the treatment of intracranial neoplastic lesions in children with neurofibromatosis 1 [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(3): 399-406. |
| [5] | HUANG Qin, HUANG Ying, LI Wen. Timing of ultrasonography in the diagnosis of fallopian tubal heterotopic pregnancy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(12): 1545-1551. |
| [6] | LI Pengyun, DAI Yinfang, LU Yanhong, YU Xingmei, XU Lina, DI Wujianfeng, HAO Chuangli. Clinical study of exhaled nitric oxide in children with asthma and allergic rhinitis [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(6): 673-679. |
| [7] | XU Xiaojun, YE Minjie, WANG Yuchen, WANG Wenxia, QIAN Sheng, YE Dandi, PAN Lele, HU Xin, YIN Xiaoli, LI Meihua, LING Guangyao. A comparative study of prepulse inhibition in children with first episode schizophrenia and normal children [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(5): 606-610. |
| [8] | LIU Zhehui, XIE Hui, WANG Jingjing, YANG Jinliuxing, ZHANG Bo, HE Xiangui, XU Xun. Analysis on life quality of children with high myopia [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(12): 1548-1553. |
| [9] | LUO Wenyi, CHEN Lin, YUAN Li, NI Ping, CAI Xiaoman, ZHANG Yaqing. Rasch analysis of postoperative cardiac rehabilitation and related factors in 3-6-year-old children with congenital heart disease [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(9): 1303-1310. |
| [10] | HU Yi, DING Guodong. Associations between paraben exposure and pulmonary function in preschool children in Shanghai [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(8): 1103-1109. |
| [11] | XING Zhengwen, WU Ying, WANG Xueli, WANG Qingyu, WANG Wenting, LI Zhi, ZHANG Bin, JIN Jing. Clinicopathological characteristics of CIC-rearranged sarcoma in children [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(8): 1151-1157. |
| [12] | Zhengwen XING, Ying WU, Xueli WANG, Qingyu WANG, Wenting WANG, Zhi LI, Bin ZHANG, Jing JIN. Analysis of clinicopathologic features and prognosis of eight children with granulosa cell tumor of ovary [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2022, 42(2): 192-196. |
| [13] | LI Bo, ZHU Ming, ZHENG Jijian. Effect of lidocaine on median effective dose of esketamine for children undergoing circumcision [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(12): 1706-1711. |
| [14] | Cui CHEN, Ye JIN, Lin WANG, Hongli LI, Caifeng WAN, Lixin JIANG. Comparative analysis of 30 cases of metaplastic carcinoma of the breast [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2022, 42(1): 70-76. |
| [15] | Xue-yao WANG, Wei-hua PAN, Wei-peng WANG, Quan-hua LIU, Wei XIE, Lei WANG, Jun WANG. Evaluation of postoperative pulmonary function in children with congenital diaphragmatic hernia and analysis of influencing factors [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2021, 41(9): 1169-1174. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||