Journal of Shanghai Jiao Tong University (Medical Science) ›› 2026, Vol. 46 ›› Issue (5): 642-650.doi: 10.3969/j.issn.1674-8115.2026.05.010
• Clinical research • Previous Articles
Gao Linna1, Tang Yangyang1,2, Liu Yifan1, Xu Junming1,#( ), Xing Tonghai1,#()
), Xing Tonghai1,#()
Received:2025-09-07
Accepted:2026-03-26
Online:2026-05-15
Published:2026-05-15
Contact:
Xu Junming, Xing Tonghai
E-mail:xjmsh@hotmail.com;xingtonghai@126.com
CLC Number:
Gao Linna, Tang Yangyang, Liu Yifan, Xu Junming, Xing Tonghai. Prediction of postoperative prognosis in hepatocellular carcinoma patients undergoing liver transplantation based on preoperative CT imaging combined with clinical indicators[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(5): 642-650.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2026.05.010
| Item | Recurrence group (n=44) | Non-recurrence group (n=51) | χ2/t value | P value |
|---|---|---|---|---|
| Age/year | 50.59±7.64 | 49.92±8.22 | 0.409 | 0.684 |
| Gender (male)/n(%) | 38 (86.36) | 48 (94.12) | 1.656 | 0.198 |
| Liver cirrhosis/n(%) | 34 (77.27) | 48 (94.12) | 5.674 | 0.017 |
| Etiology (hepatitis B)/n(%) | 40 (90.91) | 46 (90.20) | 0.014 | 0.906 |
| Preoperative AFP(≤400 ng·mL-1)/n(%) | 20 (45.45) | 43 (84.31) | 15.968 | <0.001 |
| Poor differentiation/n(%) | 6 (13.64) | 4 (7.84) | 0.842 | 0.359 |
| Tumor number≤3/n(%) | 30 (68.18) | 43 (84.31) | 3.454 | 0.063 |
| Maximum tumor diameter/n(%) | 22.455 | <0.001 | ||
| ≤3 cm | 3 (6.82) | 25 (49.02) | ||
| >3 cm and ≤8 cm | 19 (43.18) | 17 (33.33) | ||
| >8 cm | 22 (50.00) | 9 (17.65) | ||
| Distance from tumor mass to hepatic capsule/n(%) | 3.641 | 0.162 | ||
| Penetration | 13 (29.55) | 9 (17.65) | ||
| ≤2 cm | 28 (63.64) | 33 (64.70) | ||
| >2 cm | 3 (6.81) | 9 (17.65) | ||
| Hepatic capsule invasion/n(%) | 25 (56.82) | 18 (35.29) | 4.417 | 0.036 |
| Vascular tumor thrombus/n(%) | 37 (84.09) | 19 (37.25) | 21.412 | <0.001 |
| Portal vein tumor thrombus/n(%) | 9.976 | 0.007 | ||
| Main trunk | 7 (15.91) | 3 (5.88) | ||
| Branch | 7 (15.91) | 1 (1.96) | ||
| Absent | 30 (68.18) | 47 (92.16) | ||
| Satellite nodules/n(%) | 19 (43.18) | 10 (19.61) | 6.190 | 0.013 |
| LSR≤1.2/n(%) | 11 (25.00) | 12 (23.53) | 0.028 | 0.867 |
| LSLR≤1.43/n(%) | 4 (9.09) | 21 (41.18) | 12.541 | <0.001 |
Tab 1 Baseline characteristics of 95 patients
| Item | Recurrence group (n=44) | Non-recurrence group (n=51) | χ2/t value | P value |
|---|---|---|---|---|
| Age/year | 50.59±7.64 | 49.92±8.22 | 0.409 | 0.684 |
| Gender (male)/n(%) | 38 (86.36) | 48 (94.12) | 1.656 | 0.198 |
| Liver cirrhosis/n(%) | 34 (77.27) | 48 (94.12) | 5.674 | 0.017 |
| Etiology (hepatitis B)/n(%) | 40 (90.91) | 46 (90.20) | 0.014 | 0.906 |
| Preoperative AFP(≤400 ng·mL-1)/n(%) | 20 (45.45) | 43 (84.31) | 15.968 | <0.001 |
| Poor differentiation/n(%) | 6 (13.64) | 4 (7.84) | 0.842 | 0.359 |
| Tumor number≤3/n(%) | 30 (68.18) | 43 (84.31) | 3.454 | 0.063 |
| Maximum tumor diameter/n(%) | 22.455 | <0.001 | ||
| ≤3 cm | 3 (6.82) | 25 (49.02) | ||
| >3 cm and ≤8 cm | 19 (43.18) | 17 (33.33) | ||
| >8 cm | 22 (50.00) | 9 (17.65) | ||
| Distance from tumor mass to hepatic capsule/n(%) | 3.641 | 0.162 | ||
| Penetration | 13 (29.55) | 9 (17.65) | ||
| ≤2 cm | 28 (63.64) | 33 (64.70) | ||
| >2 cm | 3 (6.81) | 9 (17.65) | ||
| Hepatic capsule invasion/n(%) | 25 (56.82) | 18 (35.29) | 4.417 | 0.036 |
| Vascular tumor thrombus/n(%) | 37 (84.09) | 19 (37.25) | 21.412 | <0.001 |
| Portal vein tumor thrombus/n(%) | 9.976 | 0.007 | ||
| Main trunk | 7 (15.91) | 3 (5.88) | ||
| Branch | 7 (15.91) | 1 (1.96) | ||
| Absent | 30 (68.18) | 47 (92.16) | ||
| Satellite nodules/n(%) | 19 (43.18) | 10 (19.61) | 6.190 | 0.013 |
| LSR≤1.2/n(%) | 11 (25.00) | 12 (23.53) | 0.028 | 0.867 |
| LSLR≤1.43/n(%) | 4 (9.09) | 21 (41.18) | 12.541 | <0.001 |
| Item | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | 1.002 (0.963‒1.042) | 0.921 | ||
| Gender (male) | 0.576 (0.243‒1.364) | 0.210 | ||
| Liver cirrhosis | 0.457 (0.225‒0.929) | 0.031 | ||
| Hepatitis B | 1.431 (0.512‒4.003) | 0.495 | ||
| Preoperative AFP>400 ng·mL-1 | 4.287 (2.344‒7.838) | <0.001 | 2.746 (1.430‒5.276) | 0.002 |
| Poor differentiation | 2.446 (1.016‒5.891) | 0.046 | ||
| Tumor number>3 | 3.128 (1.618‒6.047) | <0.001 | 2.526 (1.266‒5.041) | 0.009 |
| Maximum tumor diameter | <0.001 | |||
| ≤3 cm | 1.000 | 1.000 | ||
| >3 cm and ≤8 cm | 7.385 (2.178‒25.038) | 0.001 | 5.860 (1.690‒20.325) | 0.005 |
| >8 cm | 13.751 (4.079‒46.357) | <0.001 | 8.317 (2.363‒29.273) | <0.001 |
| Distance from tumor mass to hepatic capsule | 0.142 | |||
| >2 cm | 1.000 | |||
| ≤2 cm | 3.520 (0.999‒12.399) | 0.050 | ||
| Penetration | 3.010 (0.912‒9.936) | 0.071 | ||
| Hepatic capsule invasion | 1.754 (0.965‒3.191) | 0.065 | ||
| Vascular tumor thrombus | 4.751 (2.114‒10.677) | <0.001 | ||
| Portal vein tumor thrombus | 0.007 | |||
| Absent | 1.000 | |||
| Branch | 2.868 (1.239‒6.639) | 0.014 | ||
| Main trunk | 2.894 (1.247‒6.716) | 0.013 | ||
| Satellite nodules | 2.061 (1.131‒3.756) | 0.018 | ||
| LSR>1.2 | 1.166 (0.588‒2.311) | 0.660 | ||
| LSLR>1.43 | 4.662 (1.666‒13.046) | 0.003 | 3.106 (1.086‒8.888) | 0.035 |
Tab 2 Results of Cox regression analysis of recurrence-free survival in 95 patients
| Item | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | 1.002 (0.963‒1.042) | 0.921 | ||
| Gender (male) | 0.576 (0.243‒1.364) | 0.210 | ||
| Liver cirrhosis | 0.457 (0.225‒0.929) | 0.031 | ||
| Hepatitis B | 1.431 (0.512‒4.003) | 0.495 | ||
| Preoperative AFP>400 ng·mL-1 | 4.287 (2.344‒7.838) | <0.001 | 2.746 (1.430‒5.276) | 0.002 |
| Poor differentiation | 2.446 (1.016‒5.891) | 0.046 | ||
| Tumor number>3 | 3.128 (1.618‒6.047) | <0.001 | 2.526 (1.266‒5.041) | 0.009 |
| Maximum tumor diameter | <0.001 | |||
| ≤3 cm | 1.000 | 1.000 | ||
| >3 cm and ≤8 cm | 7.385 (2.178‒25.038) | 0.001 | 5.860 (1.690‒20.325) | 0.005 |
| >8 cm | 13.751 (4.079‒46.357) | <0.001 | 8.317 (2.363‒29.273) | <0.001 |
| Distance from tumor mass to hepatic capsule | 0.142 | |||
| >2 cm | 1.000 | |||
| ≤2 cm | 3.520 (0.999‒12.399) | 0.050 | ||
| Penetration | 3.010 (0.912‒9.936) | 0.071 | ||
| Hepatic capsule invasion | 1.754 (0.965‒3.191) | 0.065 | ||
| Vascular tumor thrombus | 4.751 (2.114‒10.677) | <0.001 | ||
| Portal vein tumor thrombus | 0.007 | |||
| Absent | 1.000 | |||
| Branch | 2.868 (1.239‒6.639) | 0.014 | ||
| Main trunk | 2.894 (1.247‒6.716) | 0.013 | ||
| Satellite nodules | 2.061 (1.131‒3.756) | 0.018 | ||
| LSR>1.2 | 1.166 (0.588‒2.311) | 0.660 | ||
| LSLR>1.43 | 4.662 (1.666‒13.046) | 0.003 | 3.106 (1.086‒8.888) | 0.035 |
| Item | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | 1.003 (0.958‒1.051) | 0.891 | ||
| Gender (male) | 0.893 (0.269‒2.960) | 0.853 | ||
| Liver cirrhosis | 0.483 (0.205‒1.141) | 0.097 | ||
| Hepatitis B | 1.738 (0.414‒7.298) | 0.450 | ||
| Preoperative AFP>400 ng·mL-1 | 3.428 (1.646‒7.137) | <0.001 | 2.265 (1.027‒4.993) | 0.043 |
| Poor differentiation | 2.528 (0.964‒6.632) | 0.059 | ||
| Tumor number>3 | 2.506 (1.165‒5.390) | 0.019 | 2.464 (1.110‒5.466) | 0.027 |
| Maximum tumor diameter | 0.020 | |||
| ≤3 cm | 1.000 | 1.000 | ||
| >3 cm and ≤8 cm | 3.168 (1.029‒9.747) | 0.044 | 4.375 (1.298‒14.739) | 0.017 |
| >8 cm | 4.901 (1.602‒14.993) | 0.005 | 4.844 (1.437‒16.330) | 0.011 |
| Distance from tumor mass to hepatic capsule | 0.402 | |||
| >2 cm | 1.000 | |||
| ≤2 cm | 2.212 (0.582‒8.409) | 0.244 | ||
| Penetration | 2.329 (0.677‒8.015) | 0.180 | ||
| Hepatic capsule invasion | 1.240 (0.610‒2.518) | 0.552 | ||
| Vascular tumor thrombus | 2.533 (1.090‒5.889) | 0.031 | ||
| Portal vein tumor thrombus | 0.286 | |||
| Absent | 1.000 | |||
| Branch | 1.335 (0.397‒4.495) | 0.641 | ||
| Main trunk | 2.413 (0.802‒7.257) | 0.117 | ||
| Satellite nodules | 2.070 (1.008‒4.253) | 0.048 | ||
| LSR>1.2 | 2.676 (1.013‒7.073) | 0.047 | 4.432 (1.568‒12.523) | 0.005 |
| LSLR>1.43 | 2.198 (0.768‒6.286) | 0.142 | ||
Tab 3 Results of Cox regression analysis of overall survival in 95 patients
| Item | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR | P value | HR | P value | |
| Age | 1.003 (0.958‒1.051) | 0.891 | ||
| Gender (male) | 0.893 (0.269‒2.960) | 0.853 | ||
| Liver cirrhosis | 0.483 (0.205‒1.141) | 0.097 | ||
| Hepatitis B | 1.738 (0.414‒7.298) | 0.450 | ||
| Preoperative AFP>400 ng·mL-1 | 3.428 (1.646‒7.137) | <0.001 | 2.265 (1.027‒4.993) | 0.043 |
| Poor differentiation | 2.528 (0.964‒6.632) | 0.059 | ||
| Tumor number>3 | 2.506 (1.165‒5.390) | 0.019 | 2.464 (1.110‒5.466) | 0.027 |
| Maximum tumor diameter | 0.020 | |||
| ≤3 cm | 1.000 | 1.000 | ||
| >3 cm and ≤8 cm | 3.168 (1.029‒9.747) | 0.044 | 4.375 (1.298‒14.739) | 0.017 |
| >8 cm | 4.901 (1.602‒14.993) | 0.005 | 4.844 (1.437‒16.330) | 0.011 |
| Distance from tumor mass to hepatic capsule | 0.402 | |||
| >2 cm | 1.000 | |||
| ≤2 cm | 2.212 (0.582‒8.409) | 0.244 | ||
| Penetration | 2.329 (0.677‒8.015) | 0.180 | ||
| Hepatic capsule invasion | 1.240 (0.610‒2.518) | 0.552 | ||
| Vascular tumor thrombus | 2.533 (1.090‒5.889) | 0.031 | ||
| Portal vein tumor thrombus | 0.286 | |||
| Absent | 1.000 | |||
| Branch | 1.335 (0.397‒4.495) | 0.641 | ||
| Main trunk | 2.413 (0.802‒7.257) | 0.117 | ||
| Satellite nodules | 2.070 (1.008‒4.253) | 0.048 | ||
| LSR>1.2 | 2.676 (1.013‒7.073) | 0.047 | 4.432 (1.568‒12.523) | 0.005 |
| LSLR>1.43 | 2.198 (0.768‒6.286) | 0.142 | ||
| Index | β | Score |
|---|---|---|
| Preoperative AFP>400 ng·mL-1 | 1.010 | 6 |
| Maximum tumor diameter>3 cm and ≤8 cm | 1.768 | 10 |
| Maximum tumor diameter>8 cm | 2.118 | 12 |
| Tumor number>3 | 0.927 | 5 |
| LSLR>1.43 | 1.133 | 6 |
Tab 4 Scoring system of recurrence-free prediction model
| Index | β | Score |
|---|---|---|
| Preoperative AFP>400 ng·mL-1 | 1.010 | 6 |
| Maximum tumor diameter>3 cm and ≤8 cm | 1.768 | 10 |
| Maximum tumor diameter>8 cm | 2.118 | 12 |
| Tumor number>3 | 0.927 | 5 |
| LSLR>1.43 | 1.133 | 6 |
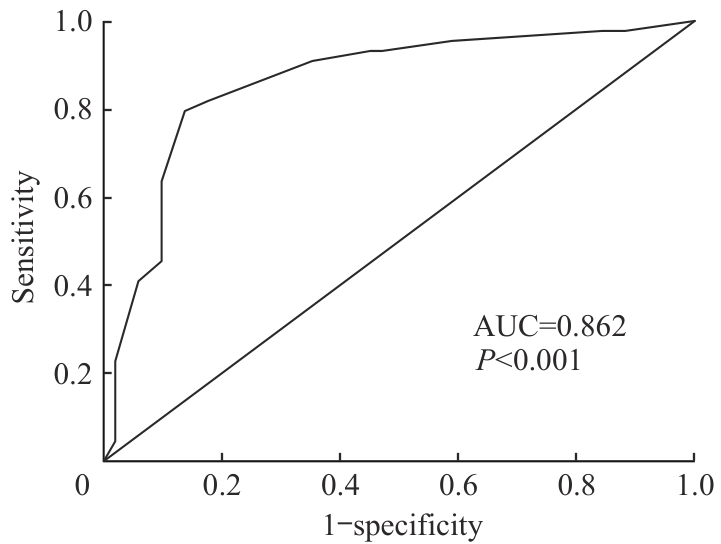
Fig 1 Predictive performance of the recurrence-free prediction model for HCC
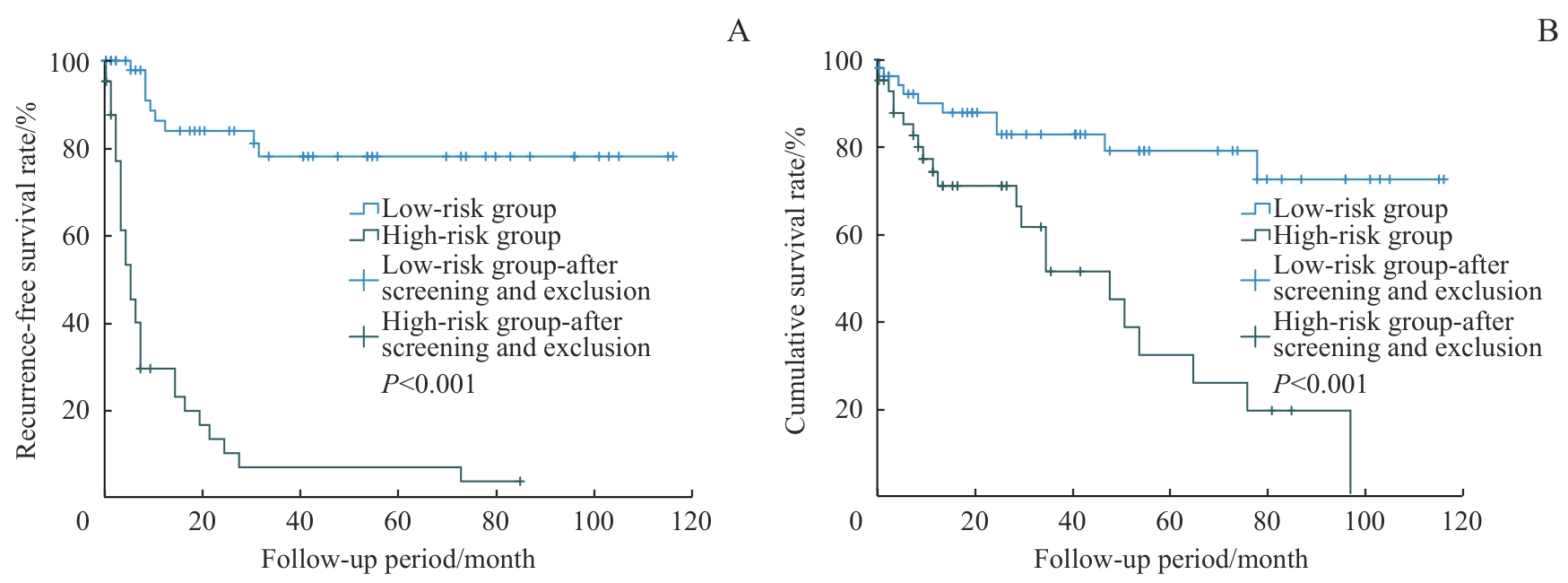
Fig 2 Comparison of recurrence-free survival rate and cumulative survival among groups stratified by recurrence-free prediction modelNote: A. Comparison of recurrence-free survival between the low-risk group and the high-risk group. B. Comparison of cumulative survival between the low-risk group and the high-risk group.
| Index | β | Score |
|---|---|---|
| Preoperative AFP>400 ng·mL-1 | 0.817 | 5 |
| Maximum tumor diameter>3 cm and ≤8 cm | 1.476 | 9 |
| Maximum tumor diameter>8 cm | 1.578 | 10 |
| Tumor number>3 | 0.902 | 6 |
| LSR>1.2 | 1.489 | 9 |
Tab 5 Scoring system of the survival prediction model
| Index | β | Score |
|---|---|---|
| Preoperative AFP>400 ng·mL-1 | 0.817 | 5 |
| Maximum tumor diameter>3 cm and ≤8 cm | 1.476 | 9 |
| Maximum tumor diameter>8 cm | 1.578 | 10 |
| Tumor number>3 | 0.902 | 6 |
| LSR>1.2 | 1.489 | 9 |
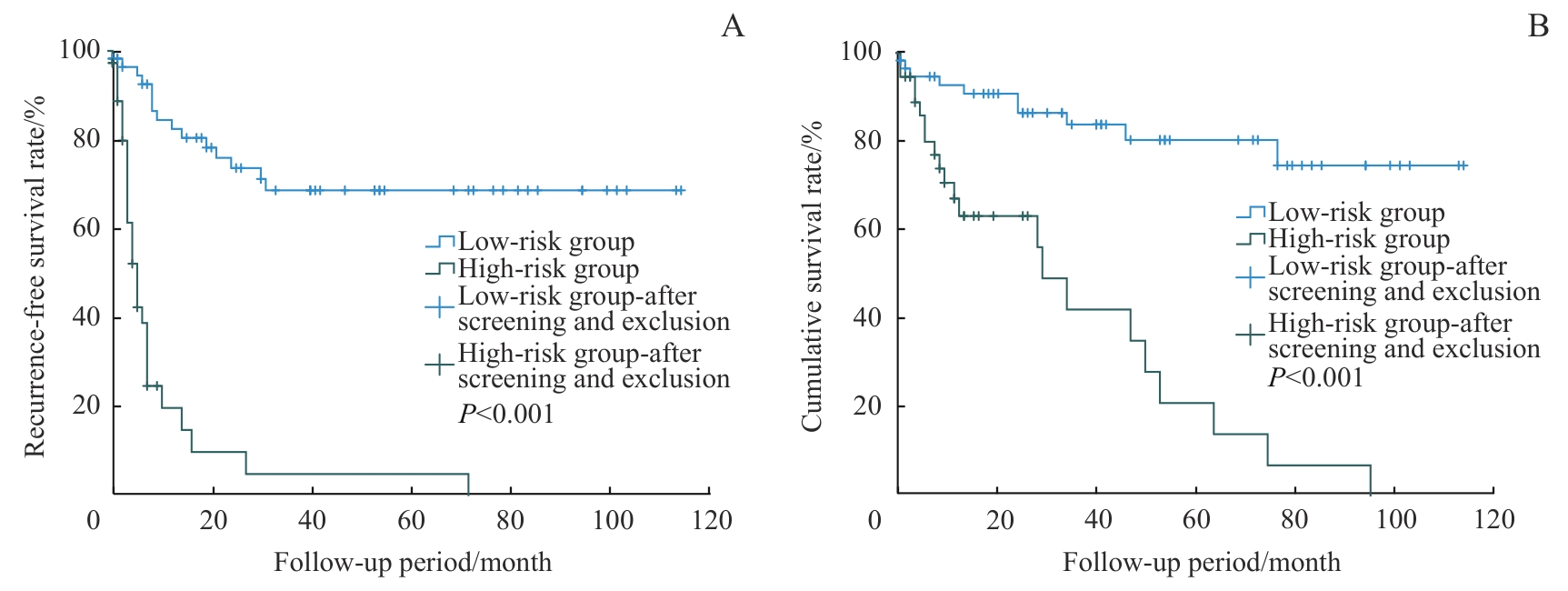
Fig 3 Comparison of recurrence-free survival rate and cumulative survival among groups stratified by survival prediction modelNote: A. Comparison of recurrence-free survival between the low-risk group and the high-risk group. B. Comparison of cumulative survival between the low-risk group and the high-risk group.
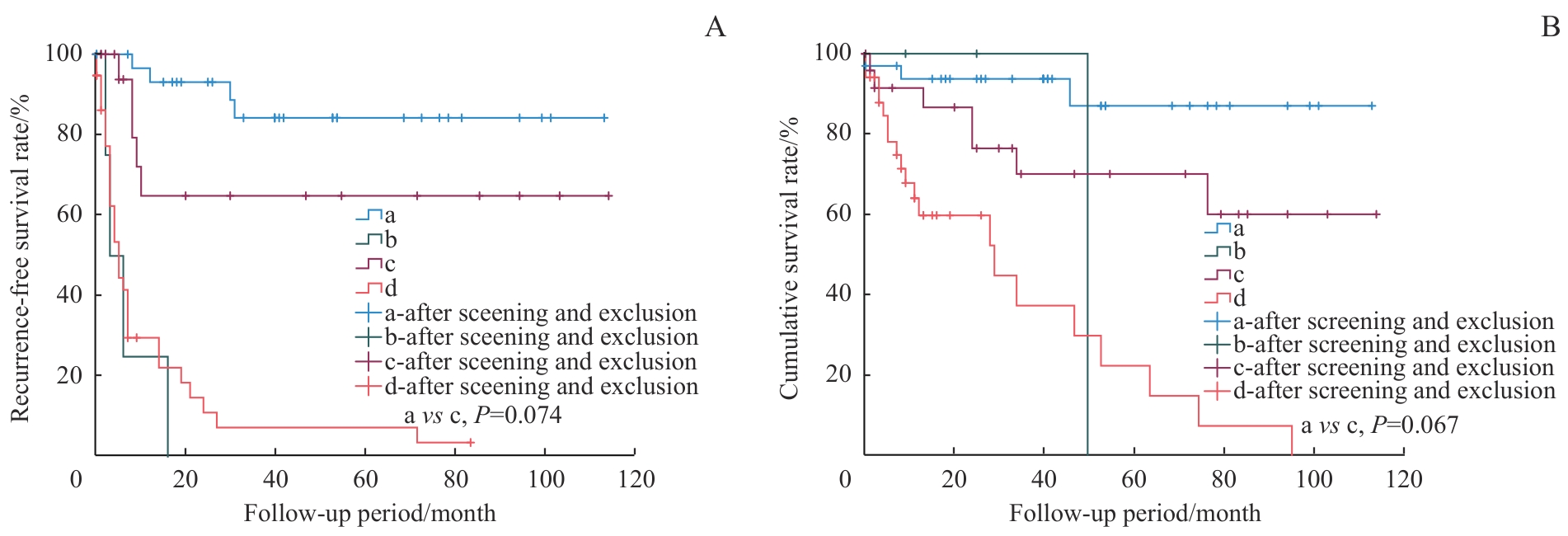
Fig 4 Kaplan-Meier curves of recurrence-free survival and cumulative survival stratified by the prediction models and the UCSF criteriaNote: A. Comparison of recurrence-free survival among groups stratified by the recurrence-free prediction model and the UCSF criteria. B. Comparison of cumulative survival among groups stratified by the survival prediction model and the UCSF criteria. a—Low-risk, within UCSF criteria; b—High-risk, within UCSF criteria; c—Low-risk, beyond UCSF criteria; d—High-risk, beyond UCSF criteria.
| [1] | Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74(3): 229-263. |
| [2] | di Marco L, Romanzi A, Pivetti A, et al. Suppressing, stimulating and/or inhibiting: the evolving management of HCC patient after liver transplantation[J]. Crit Rev Oncol Hematol, 2025, 207: 104607. |
| [3] | Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis[J]. N Engl J Med, 1996, 334(11): 693-699. |
| [4] | Shen Y H, Chen S, Peng Y F, et al. Quantitative assessment of the effect of glutathione S-transferase genes GSTM1 and GSTT1 on hepatocellular carcinoma risk[J]. Tumor Biol, 2014, 35(5): 4007-4015. |
| [5] | 郭晓娜, 韩文, 陈思荣. 肝脾体积在肝硬化中的相关进展[J]. 临床医学进展, 2022, 12(12): 11045-11050. |
| Guo X N, Han W, Chen S R. Related progress in liver and spleen volume in liver cirrhosis[J]. Advances in Clinical Medicine, 2022, 12(12): 11045-11050. | |
| [6] | Kwon J H, Lee S S, Yoon J S, et al. Liver-to-spleen volume ratio automatically measured on CT predicts decompensation in patients with B viral compensated cirrhosis[J]. Korean J Radiol, 2021, 22(12): 1985-1995. |
| [7] | Hu N, Yan G, Tang M W, et al. CT-based methods for assessment of metabolic dysfunction associated with fatty liver disease[J]. Eur Radiol Exp, 2023, 7(1): 72. |
| [8] | Brown Z J, Ruff S M, Pawlik T M. The effect of liver disease on hepatic microenvironment and implications for immune therapy[J]. Front Pharmacol, 2023, 14: 1225821. |
| [9] | Ren A, Li Z Q, Zhou X Z, et al. Evaluation of the α-fetoprotein model for predicting recurrence and survival in patients with hepatitis B virus (HBV)-related cirrhosis who received liver transplantation for hepatocellular carcinoma[J]. Front Surg, 2020, 7: 52. |
| [10] | Sullivan L M, Massaro J M, D′Agostino R B Sr. Presentation of multivariate data for clinical use: the Framingham Study risk score functions[J]. Stat Med, 2004, 23(10): 1631-1660. |
| [11] | 张炜琪, 谢炎, 陈池义, 等. 超米兰标准肝细胞癌肝移植术后复发预测模型的建立[J]. 临床肝胆病杂志, 2022, 38(4): 837-842. |
| Zhang W Q, Xie Y, Chen C Y, et al. Development of a new model for predicting recurrence after liver transplantation for hepatocellular carcinoma beyond Milan criteria[J]. Journal of Clinical Hepatology, 2022, 38(4): 837-842. | |
| [12] | Jou Y J, Huang C L, Cho H J. A VIF-based optimization model to alleviate collinearity problems in multiple linear regression[J]. Comput Stat, 2014, 29(6): 1515-1541. |
| [13] | Hassanzad M, Hajian-Tilaki K. Methods of determining optimal cut-point of diagnostic biomarkers with application of clinical data in ROC analysis: an update review[J]. BMC Med Res Methodol, 2024, 24(1): 84. |
| [14] | 中国医师协会器官移植医师分会,中华医学会器官移植学分会肝移植学组. 中国肝癌肝移植临床实践指南(2021版)[J]. 中华移植杂志(电子版), 2021, 15(6): 321-328. |
| Chinese College of Transplant Doctors, Liver Transplantation Group, Chinese Society of Organ Transplantation, Chinese Medical Association. The Chinese clinical practice guidelines on liver transplantation for hepatocellular carcinoma (2021 edition)[J]. Chinese Journal of Transplantation (Electronic Edition), 2021, 15(6): 321-328. | |
| [15] | 沈未, 鲁迪, 徐骁. 肝癌肝移植适应证的科学演进[J]. 器官移植, 2025, 16(2): 202-207. |
| Shen W, Lu D, Xu X. Scientific evolution of indications for liver transplantation in hepatocellular carcinoma[J]. Organ Transplantation, 2025, 16(2): 202-207. | |
| [16] | Schindler P, von Beauvais P, Hoffmann E, et al. Combining radiomics and imaging biomarkers with clinical variables for the prediction of HCC recurrence after liver transplantation[J]. Liver Transpl, 2025, 31(10): 1226-1237. |
| [17] | Jiang N, Zeng K N, Dou K F, et al. Preoperative α-fetoprotein and fibrinogen predict hepatocellular carcinoma recurrence after liver transplantation regardless of the Milan criteria: model development with external validation[J]. Cell Physiol Biochem, 2018, 48(1): 317-327. |
| [18] | Brusset B, Dumortier J, Cherqui D, et al. Liver transplantation for hepatocellular carcinoma: a real-life comparison of Milan criteria and AFP model[J]. Cancers, 2021, 13(10): 2480. |
| [19] | Kutaiba N, Chung W, Goodwin M, et al. The impact of hepatic and splenic volumetric assessment in imaging for chronic liver disease: a narrative review[J]. Insights Imaging, 2024, 15(1): 146. |
| [20] | Huang D Q, Tran A, Tan E X, et al. Characteristics and outcomes of hepatocellular carcinoma patients with macrovascular invasion following surgical resection: a meta-analysis of 40 studies and 8 218 patients[J]. Hepatobiliary Surg Nutr, 2022, 11(6): 848-860. |
| [1] | Liu Zhitong, Fan Zixu, Li Xiang, Zhang Min. Safety outcomes of immunotherapy continuation versus permanent discontinuation after immune checkpoint inhibitor-associated myocarditis in patients with lung cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(5): 612-623. |
| [2] | Peng Qianqian, Song Jinghan, Xu Xingyi, Xiao Hui. Bioinformatic analysis and validation of the RNA-binding protein HuR promoting non-small cell lung cancer progression via ITGB1 [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(4): 451-466. |
| [3] | LI Qianyu, QIAN Yifei, LI Songling, ZHU Zijun, QIN Wenli, LIU Yanfeng, QIU Bijun. Function and mechanism of suppressor of zeste 12 in hepatocellular carcinoma [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(9): 1138-1148. |
| [4] | ZHU Zijun, QIAN Yife, LI Qianyu, LI Songling, QIN Wenli, LIU Yanfeng. Anaphase-promoting complex subunit 10 promotes hepatocellular carcinoma progression through regulation of the PI3K-AKT-mTOR signaling pathway [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(9): 1171-1182. |
| [5] | LU Yefeng, GAO Leiqing, NI Xiaoxiao, FU Jingjing. Multitime-point monitoring and analysis of influencing factors of early postoperative blood glucose and lipid levels in pediatric liver transplantation [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(4): 443-451. |
| [6] | CHEN Jiaying, CHU Yimin, PENG Haixia. Study on prediction model and influencing factors of progression-free survival in colorectal cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2025, 45(3): 324-334. |
| [7] | Aishanjiang Kedeerya, FU Yi, LAI Donglin, WU Hailong, GONG Wei. An integrated prognostic model of nuclear-encoded mitochondrial gene signature and clinical information for hepatocellular carcinoma [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(1): 1-12. |
| [8] | LI Qianyu, GUO Wenyun, QIAN Yifei, LI Songling, ZHU Zijun, LIU Yanfeng. Study on the significance and mechanism of ASGR1 in hepatocellular carcinoma [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(9): 1107-1114. |
| [9] | YU Li, SU Xiandu, ZHANG Min, LI Yahui, WANG Le. Construction and validation of prognostic risk model for hepatocellular carcinoma based on biological analysis of palmitoyl-associated enzyme long-chain non-coding RNA [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(6): 747-754. |
| [10] | YANG Xiaoxuan, ZHU Shan, QIAN Cheng, CHU Xiaoying. Effect of intraoperative use of low-dose dexmedetomidine on the prognosis of patients undergoing breast cancer surgery [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(2): 194-200. |
| [11] | BENEDICK Jun Er Chin, SON Peng, ZHANG Yifan, WANG Junqing, GUO Simin. Research progress of the impact of nonalcoholic fatty liver disease on chronic hepatitis B infection [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(12): 1585-1590. |
| [12] | LU Yu, WANG Hao, BA Qian. Role of gut microbiota in hepatocellular carcinoma: cancer occurrence, progresses and treatments [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(7): 939-944. |
| [13] | HU Zhexuan, ZHANG Xin, WO Lulu, LI Jingchi, WANG Jiao, ZHOU Cixiang, ZHAO Qian. Study on the function of TRMT61A in liver cancer cell and its mechanism [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(6): 742-750. |
| [14] | ZHU Tianyu, ZONG Chunyan, XU Shiqiong, GE Shengfang, FAN Xianqun, JIA Renbing. Relationship between histopathological features, Ki-67 expression and prognosis of conjunctival melanoma [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(5): 617-623. |
| [15] | XIA Kunjian, DENG Linlin, WANG Lin. Construction and evaluation of a prediction model for liver injury induced by chemotherapy for breast cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(4): 502-509. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||