目的·探讨丙型病毒性肝炎(丙肝)肝硬化失代偿期患者发生细菌感染的影响因素,建立列线图预测模型并进行评价。方法·回顾分析昆明市第三人民医院肝病科2020年1月—2021年12月因丙肝肝硬化住院的失代偿期患者574例,以是否发生细菌感染分为细菌感染组和非细菌感染组。收集患者的一般资料、入院合并症及实验室指标。经单因素分析、最小绝对收缩和选择算子(least absolute shrinkage and selection operator,LASSO)回归筛选变量,采用多因素Logistic回归分析影响因素,据此构建列线图模型并进行验证。采用决策曲线及临床影响曲线(clinical impact curve,CIC)评估模型的临床实际应用价值。结果·纳入患者中28.4%(163/574)的患者发生细菌感染,共191个部位,以自发性细菌性腹膜炎(86/191)和肺部细菌感染(79/191)为主;共分离培养出病原菌78株,以肺炎克雷伯菌(15/78)和大肠埃希菌(15/78)为主。多因素Logistic回归分析显示年龄≥60岁[比值比(odds ratio,OR)=2.054,95%置信区间(confidence interval,CI) 1.104~3.822,P=0.023]、女性(OR=1.701,95%CI 1.112~2.602,P=0.014)、腹水(OR=2.386,95%CI 1.601~3.557,P=0.000)、近2周有创操作史(OR=2.605,95%CI 1.368~4.960,P=0.004)、住院时间≥2周(OR=1.629,95%CI 1.098~2.416,P=0.015)是丙肝肝硬化失代偿期患者发生细菌感染的独立危险因素;输注人血白蛋白(OR=0.324,95%CI 0.194~0.542,P=0.000)和高总胆固醇(total cholesterol,CHOL;OR=0.675,95%CI 0.549~0.830,P=0.000)水平是其保护因素。用以上7个影响因素构建列线图模型,采用受试者工作特征曲线(receiver operator characteristic curve,ROC曲线)分析显示曲线下面积(area under the curve,AUC)为0.736,敏感度80.4%,特异度65.1%。Hosmer-lemeshow检验显示,模型具有较好的拟合度(χ2=9.030,P=0.340)。使用Bootstrap法内部重复抽样1 000次进行验证,平均绝对误差0.010,校正曲线和理想曲线基本拟合,预测值和实际值一致性较好。决策曲线显示列线图模型在高风险阈值(0.040~0.715)范围时,有着一定的临床实用性。CIC显示该列线图模型可进行高风险人群分层预测。结论·研究所构建的列线图模型具有较好的预测性、一致性和临床实用性,可为临床医师初步判断丙肝肝硬化失代偿期患者发生细菌感染的风险提供依据。
关键词:丙型病毒性肝炎
;
细菌感染
;
肝硬化失代偿期
;
危险因素
;
列线图
Abstract
Objective ·To explore the influencing factors of bacterial infection in decompensated stage of hepatitis C cirrhosis, and establish a risk prediction model of nomogram. Methods ·A total of 574 patients with decompensated hepatitis C cirrhosis were retrospectively collected from The Third People′s Hospital of Kunming between January 2020 and December 2021, and divided into non-infected and infected groups according to whether bacterial infection occurred. The general information, complications, and laboratory indicators were collected. The variables were screened by univariate analysis, and least absolute shrinkage and selection operator (LASSO) regression, and the nomogram model were constructed and verified by multivariate Logistic regression analysis of influencing factors. The decision curve and clinical impact curve (CIC) were used to evaluate the clinical application value of the model. Results ·Bacterial infections occurred in 28.4% (163/574) of the patients, with a total of 191 sites, mainly including spontaneous bacterial peritonitis (86/191) and pulmonary bacterial infections (79/191). Totally 78 strains of pathogens were isolated and cultured, mainly including Klebsiella pneumoniae (15/78) and Escherichia coli (15/78). Multivariate Logistic regression analysis showed that age ≥60 years [odds ratio (OR)=2.054, 95% confidence interval (CI) 1.104‒3.822, P=0.023], female (OR=1.701, 95%CI 1.112‒2.602, P=0.014), ascites (OR=2.386, 95%CI 1.601‒3.557, P=0.000), history of invasive procedures in the last two weeks (OR=2.605, 95%CI 1.368‒4.960, P=0.004), and hospitalization time≥2 weeks (OR=1.629, 95%CI 1.098‒2.416, P=0.015) were independent risk factors for bacterial infection in decompensated hepatitis C cirrhosis patients, while infusing human serum albumin (OR=0.324, 95%CI 0.194‒0.542, P=0.000) and high level of total cholesterol (OR=0.675, 95%CI 0.549‒0.830, P=0.000) were protective factors. The nomogram model was constructed with the above seven influencing factors. Receiver operator characteristic (ROC) curve analysis showed that the area under the curve (AUC) was 0.736 and the sensitivity was 80.4%; and the specificity was 65.1%. Hosmer-lemeshow test showed that the model had a good degree of fit (χ2=9.030, P=0.340). The bootstrap method was used for internal repeated sampling for 1 000 times, the average absolute error was 0.010, the calibration curve and the ideal curve were basically fitted, and the predicted values were in good agreement with the actual values. The decision curve showed that the nomogram model had certain clinical practicability in the high risk threshold range (0.040‒0.715). CIC showed that the nomogram model can be used to forecast the high-risk population in different levels. Conclusion ·The nomogram risk prediction model constructed in this study has good predictability, consistency and clinical practicability, and can provide evidence for clinicians to preliminary judge the risk of bacterial infection in patients with decompensated hepatitis C cirrhosis.
XUE Linlin, LI Binghan, CHANG Lixian, LI Weikun, LIU Chunyun, LIU Li. Construction and evaluation of a nomogram prediction model for bacterial infection in patients with decompensated hepatitis C cirrhosis. Journal of Shanghai Jiao Tong University (Medical Science)[J], 2023, 43(1): 52-60 doi:10.3969/j.issn.1674-8115.2023.01.007
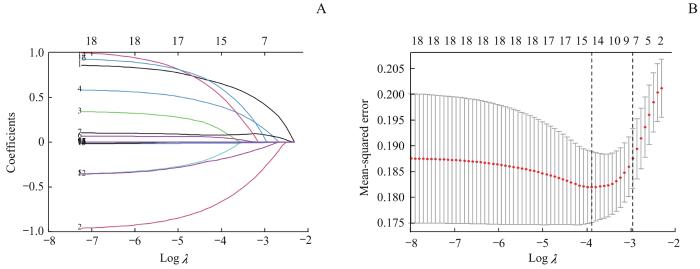
Note: A. Path diagram of regression coefficient. The upper abscissas was the number of variables with non-zero coefficients in the model at this time, the lower abscissas was the logarithm of the penalty coefficient (λ), and the ordinate was the value of the coefficient. B. Cross-verification curve of LASSO regression. The upper and lower abscissas were the same as Fig A, and the ordinate was likelihood bias. The dotted line on the left of Fig B indicates the number of variables corresponding to the minimum λ (when the model has the highest fitting effect), and the number of variables was 14. The dotted line on the right indicates one standard error of the least λ (when the model has better fitting effect, fewer and simpler variables are included), and the number of variables was 7.
Fig 1
LASSO regression model of bacterial infection in patients with decompensated hepatitis C cirrhosis
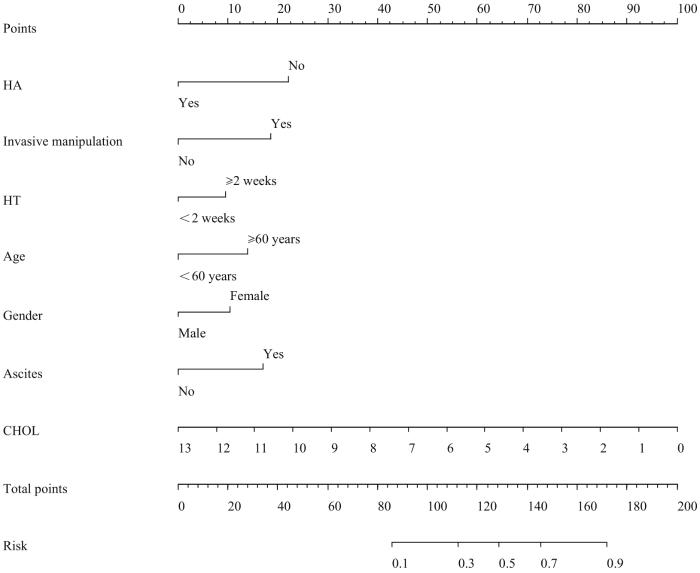
Note: HA—human serum albumin was infused; HT—hospitalization time.
Fig 2
Multivariate Logistic regression analysis of nomogram of bacterial infection in patients with decompensated hepatitis C cirrhosis
2.5 列线图预测模型的评价
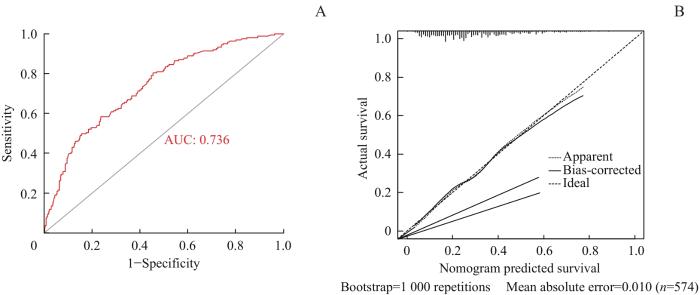
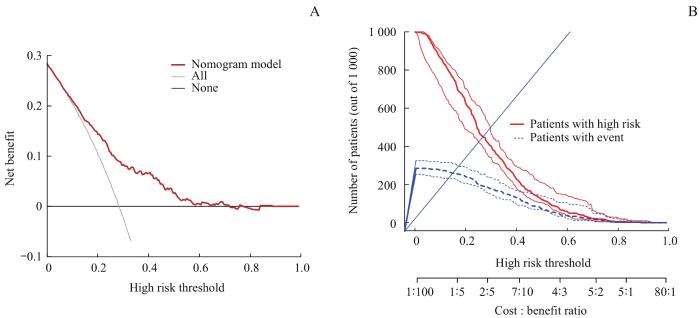
采用ROC曲线分析(图3A)显示,曲线下面积(area under the curve,AUC)为0.736(95%CI 0.692~0.781,P=0.000),敏感度80.4%,特异度65.1%。校准曲线(图3B)显示平均绝对误差0.010,表明细菌感染发生的实际值和预测值之间有较好的一致性。DCA(图4A)显示,阈值为0.040~0.715时,列线图模型有一定的临床实用性。使用CIC进行列线图模型预测1 000人的风险分层,显示“损失∶受益”坐标轴,赋以8个刻度,显示置信区间,如图4B所示:红色曲线表示,在各个阈概率下,被列线图模型划分为阳性(高风险)的人数;蓝色曲线为各个阈概率下真阳性的人数,随着阈值增大,预测的阳性例数减少,其中真阳性的例数也逐渐减少。
The study was designed by LI Binghan, LIU Chunyun, and LI Weikun. The manuscript of revision was directed by LIU Li. XUE Linlin and CHANG Lixian were responsible for data collection and analysis as well as paper writing and modification.
利益冲突声明
所有作者声明不存在利益冲突。
All authors disclose no relevant conflict of interests.
National Health Commission of the People′s Republic of China. Prevention and control plan of viral hepatitis in China (2017‒2020)[EB/OL]. (2017-11-10)[2022-09-01]. http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/11/20171113134002475.pdf.
HEI F X, YE S D, DING G W, et al. Epidemiological analysis on reported hepatitis C cases in China from 2012 to 2016[J]. Biomed Environ Sci, 2018, 31(10): 773-776.
PIANO S, SINGH V, CARACENI P, et al. Epidemiology and effects of bacterial infections in patients with cirrhosis worldwide[J]. Gastroenterology, 2019, 156(5): 1368-1380.e10.
PLEGUEZUELO M, BENITEZ J M, JURADO J, et al. Diagnosis and management of bacterial infections in decompensated cirrhosis[J]. World J Hepatol, 2013, 5(1): 16-25.
FERNÁNDEZ J, PRADO V, TREBICKA J, et al. Multidrug-resistant bacterial infections in patients with decompensated cirrhosis and with acute-on-chronic liver failure in Europe[J]. J Hepatol, 2019, 70(3): 398-411.
Chinese Society of Infectious Diseases, Chinese Medical Association. Expert consensus on diagnosis and treatment of end-stage liver disease complicated infection (2021 version)[J]. Chinese Journal of Hepatology, 2022, 30(2): 147-158.
MIKUŁA T, SAPUŁA M, JABŁOŃSKA J, et al. Significance of heparin-binding protein and D-dimers in the early diagnosis of spontaneous bacterial peritonitis[J]. Mediators Inflamm, 2018, 2018: 1969108.
SPAHR L, MORARD I, HADENGUE A, et al. Procalcitonin is not an accurate marker of spontaneous bacterial peritonitis in patients with cirrhosis[J]. Hepato gastroenterology, 2001, 48(38): 502-505.
ZHU Y, CHENG H, MIN R, et al. Computed tomography images under the nomogram mathematical prediction model in the treatment of cerebral infarction complicated with nonvalvular atrial fibrillation and the impacts of virus infection[J]. Contrast Media Mol Imaging, 2022, 2022: 3950641.
LI S Y, YIN C H, CHEN J S, et al. A nomogram for predicting the development of serious bacterial infections in febrile term neonates: a single medical center experience in southern Taiwan[J]. Pediatr Neonatol, 2022, 63(6): 605-612.
XU X F, LI H W, SHENG Y J, et al. Nomogram for prediction of bronchial mucus plugs in children with Mycoplasma pneumoniae pneumonia[J]. Sci Rep, 2020, 10(1): 4579.
Chinese Society of Hepatology and Chinese Society of Infectious Diseases, Chinese Medical Association. Guidelines for prevention and treatment of hepatitis C (2019 edition)[J]. Journal of Practical Hepatology, 2020, 23(1): S33-S52.
PIANO S, TONON M, ANGELI P. Changes in the epidemiology and management of bacterial infections in cirrhosis[J]. Clin Mol Hepatol, 2021, 27(3): 437-445.
WU L, HONG H, LI W Z, et al. Clinical characteristics of bacterial infections in patients with liver cirrhosis[J]. Chinese Journal of Infection and Chemotherapy, 2020, 20(6): 601-606.
XU W Q, WU Y Q, ZHANG J Y, et al. Mechanism of estrogen against liver fibrosis in postmenopausal women with chronic liver disease[J]. Journal of Clinical Hepatology, 2021, 37(10): 2425-2428.
KLAIR J S, YANG J D, ABDELMALEK M F, et al. A longer duration of estrogen deficiency increases fibrosis risk among postmenopausal women with nonalcoholic fatty liver disease[J]. Hepatology, 2016, 64(1): 85-91.
MARTIN MATEOS R, ALBILLOS A. Sepsis in patients with cirrhosis awaiting liver transplantation: new trends and management[J]. Liver Transpl, 2019, 25(11): 1700-1709.
MARTÍNEZ J, HERNÁNDEZ-GEA V, RODRÍGUEZ-DE-SANTIAGO E, et al. Bacterial infections in patients with acute variceal bleeding in the era of antibiotic prophylaxis[J]. J Hepatol, 2021, 75(2): 342-350.
GONG N K, QUAN B, LU J, et al. Analysis of the risk factors of nosocomial infection among patients with decompensated liver cirrhosis inpatients based on regression analysis[J]. Journal of Qiqihar Medical University, 2021, 42(9): 772-775.
XU S, XU F, YING L Y, et al. Etiological charateristics and influencing factor for nosocomial infection in liver cirrhosis patients complicated with upper gastrointestinal hemorrhage[J]. Chinese Journal of Nosocomiology, 2019, 29(1): 71-74.
ARROYO V, ANGELI P, MOREAU R, et al. The systemic inflammation hypothesis: towards a new paradigm of acute decompensation and multiorgan failure in cirrhosis[J]. J Hepatol, 2021, 74(3): 670-685.
NING Y X, KIM J K, MIN H K, et al. Cholesterol metabolites alleviate injured liver function and decrease mortality in an LPS-induced mouse model[J]. Metabolism, 2017, 71: 83-93.
GAO P, XIAO P, CHEN Q F, et al. Analysis of factors influencing serum lipids of patients with chronic hepatitis B infection[J]. Academic Journal of Second Military Medical University, 2011, 32(12): 1375-1377.
DELGADO-COELLO B, BRIONES-ORTA M A, MACÍAS-SILVA M, et al. Cholesterol: recapitulation of its active role during liver regeneration[J]. Liver Int, 2011, 31(9): 1271-1284.
XUE Y J, YANG L, ZHU Y, et al. Value of the serum albumin, cholinesterase and prothrombin activity in the diagnosis of viral hepatitis cirrhosis[J]. Journal of Bengbu Medical College, 2019, 44(3): 306-308, 313.
GUAN W L. Clinical application value of serum CHE, ALB and CHO levels in liver function assessment of patients with hepatitis cirrhosis[J]. Laboratory Medicine and Clinic, 2017, 14(18): 2741-2742.
DESCHÊNES M, VILLENEUVE J P. Risk factors for the development of bacterial infections in hospitalized patients with cirrhosis[J]. Am J Gastroenterol, 1999, 94(8): 2193-2197.
ZHANG Q, SHI B X, WU L. Characteristics and risk factors of infections in patients with HBV-related acute-on-chronic liver failure: a retrospective study[J]. PeerJ, 2022, 10: e13519.
YANG H L, LIU X J, HE Y L, et al.Clinical characteristics of and risk factors for nosocomial infections in patients with hospitalized decompensated hepatitis B liver cirrhosis[J]. Journal of Practical Hepatology, 2020, 23(1): 78-81.
CHINA L, FREEMANTLE N, FORREST E, et al. A randomized trial of albumin infusions in hospitalized patients with cirrhosis[J]. N Engl J Med, 2021, 384(9): 808-817.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}