上海交通大学学报(医学版) ›› 2026, Vol. 46 ›› Issue (6): 759-769.doi: 10.3969/j.issn.1674-8115.2026.06.008
• 论著 · 临床研究 • 上一篇
冯琳鸿1, 吴迪1, 朱迎春1, 许佳瑞2, 张翀3, 王亚琨1,3( )
)
收稿日期:2025-09-10
接受日期:2026-01-12
出版日期:2026-06-28
发布日期:2026-06-29
通讯作者:
王亚琨,副主任医师,硕士;电子信箱:kyky1818@163.com。基金资助:
Feng Linhong1, Wu Di1, Zhu Yingchun1, Xu Jiarui2, Zhang Chong3, Wang Yakun1,3()
Received:2025-09-10
Accepted:2026-01-12
Online:2026-06-28
Published:2026-06-29
Contact:
Wang Yakun, E-mail: kyky1818@163.com.Supported by:摘要:
目的·探讨腹膜透析(腹透)患者使用艾考糊精腹透液(icodextrin-based peritoneal dialysis solution,ICO)的临床获益,分析ICO对腹透患者主要不良心血管事件(major adverse cardiovascular event,MACE)发生率等的影响。方法·该研究为多中心、前瞻性、随机对照临床研究。纳入2023年1月至2024年1月3家临床中心的120例腹透患者作为研究对象,按照1∶2随机对照分组,分为ICO组40例和对照组80例:ICO组患者每日白天使用1.5%或2.5%葡萄糖腹透液,夜间使用7.5% ICO留腹8~12 h;对照组患者每日白天使用1.5%或2.5%葡萄糖腹透液,夜间使用2.5%葡萄糖腹透液留腹8~12 h。干预期为12个月。收集患者的基本信息,以及干预前后实验室指标、人体多余水分(overhydration,OH)值、腹膜平衡试验结果、超声心动图指标等,记录2组患者的MACE、住院和死亡情况。采用Kaplan-Meier生存曲线比较2组MACE发生率、住院率、全因死亡率和心血管疾病死亡率的差异。使用多因素Cox回归分析腹透患者发生MACE的相关因素。结果·经过12个月的干预,ICO组的空腹血糖、糖化血红蛋白、体质量指数、OH值和N末端B型钠尿肽前体(N-terminal pro-B-type natriuretic peptide,NT-proBNP)均显著低于对照组(均P<0.05),ICO组的24 h超滤量、残肾Kt/V(residual urea clearance index,r-Kt/V)、总Kt/V(total urea clearance index,t-Kt/V)均显著高于对照组(均P<0.05);心脏超声结果显示ICO组的左心室舒张末期内径(left ventricular end-diastolic diameter,LVEDd)和左心室心肌质量指数(left ventricular mass index,LVMI)均显著低于对照组(均P<0.05),左室射血分数(left ventricular ejection fraction,LVEF)显著高于对照组(P<0.05)。Kaplan-Meier生存曲线分析结果显示:ICO组的心血管疾病死亡率(Log-rank P=0.048)及MACE发生率(Log-rank P=0.043)均显著低于对照组;2组全因死亡率及住院率差异无统计学意义。多因素Cox回归分析显示,既往存在心血管疾病(HR=1.57,95%CI 1.07~2.33,P=0.035)、腹膜高转运(HR=1.65,95%CI 1.08~2.89,P=0.045)以及高NT-proBNP(HR=1.38,95%CI 1.13~2.89,P=0.013)是腹透患者发生MACE的危险因素,使用ICO(HR=0.35,95%CI 0.17~0.89,P=0.012)是其保护性因素。结论·ICO可改善腹透患者的糖代谢、减轻容量负荷、提高透析充分性,并减少腹透患者MACE发生率及心血管疾病死亡率。
中图分类号:
冯琳鸿, 吴迪, 朱迎春, 许佳瑞, 张翀, 王亚琨. 腹膜透析患者应用艾考糊精腹透液的临床获益及心血管风险分析[J]. 上海交通大学学报(医学版), 2026, 46(6): 759-769.
Feng Linhong, Wu Di, Zhu Yingchun, Xu Jiarui, Zhang Chong, Wang Yakun. Clinical benefits of icodextrin-based peritoneal dialysis solution and its impact on cardiovascular risk in patients undergoing peritoneal dialysis[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(6): 759-769.
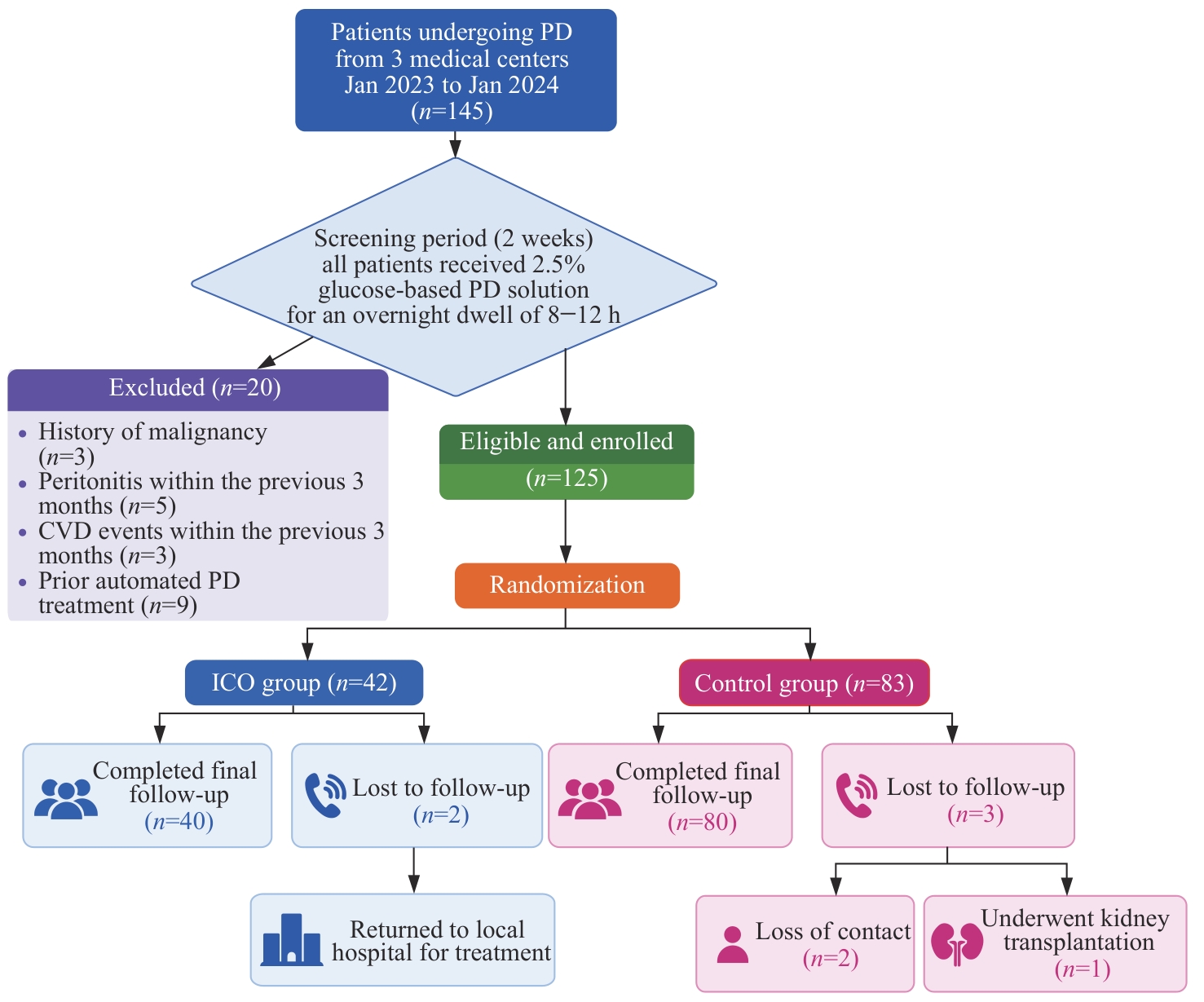
图1 研究对象纳入流程图
Fig 1 Flowchart of patient enrollment
| Item | Total (n=120) | ICO group (n=40) | Control group (n=80) | P value |
|---|---|---|---|---|
| Gender | 0.899 | |||
| Male/n(%) | 62 (51.67) | 21 (52.50) | 41 (51.25) | |
| Female/n(%) | 58 (48.33) | 19 (47.50) | 39 (48.75) | |
| Age/year | 60.25±12.00 | 61.25±8.16 | 59.58±14.13 | 0.080 |
| BMI/(kg·m-2) | 24.14±2.27 | 24.66±1.86 | 23.79±3.25 | 0.296 |
| PD duration/month | 16.5 (9.0, 22.0) | 11.5 (9.0, 20.8) | 17.0 (10.5, 23.8) | 0.342 |
| Smoking/n(%) | 17 (14.17) | 4 (10.00) | 13 (16.25) | 0.583 |
| Comorbidity/n(%) | ||||
| CVD | 23 (19.17) | 9 (22.50) | 14 (17.50) | 0.505 |
| Hypertension | 83 (69.17) | 29 (72.50) | 54 (67.50) | 0.573 |
| Diabetes | 44 (36.67) | 15 (37.50) | 29 (36.25) | 0.894 |
| Cerebral infarction | 7 (5.83) | 2 (5.00) | 5 (6.25) | 0.782 |
| Primary kidney disease/n(%) | 0.260 | |||
| Chronic glomerulonephritis | 58 (48.33) | 17 (42.50) | 41 (51.25) | |
| Diabetic nephropathy | 39 (32.50) | 13 (32.50) | 26 (32.50) | |
| Hypertensive nephropathy | 17 (14.17) | 6 (15.00) | 11 (13.75) | |
| Others | 6 (5.00) | 4 (10.00) | 2 (2.50) | |
| OH/L | 4.35±0.95 | 4.31±0.95 | 4.38±0.97 | 0.809 |
| SBP/mmHg | 142.85±23.92 | 151.88±23.64 | 136.83±22.62 | 0.034 |
| DBP/mmHg | 80.23±12.67 | 83.25±15.22 | 78.21±10.51 | 0.036 |
| Hb/(g·L-1) | 96.12±13.02 | 92.87±14.38 | 98.29±11.85 | 0.202 |
| CRP/(mg·L-1) | 14.14±19.50 | 10.58±12.61 | 16.51±13.04 | 0.057 |
| IL-6/(pg·mL-1) | 24.98±15.08 | 39.57±10.82 | 25.26±13.22 | 0.072 |
| FBG/(mmol·L-1) | 6.45±2.23 | 6.63±3.05 | 6.32±1.52 | 0.712 |
| HbA1c/% | 6.32±1.59 | 6.68±2.17 | 6.08±1.04 | 0.323 |
| Alb/(g·L-1) | 31.82±4.38 | 30.56±4.47 | 32.66±4.2 | 0.146 |
| BUN/(μmol·L-1) | 23.40±5.98 | 22.40±6.04 | 24.37±6.10 | 0.587 |
| TC/(mmol·L-1) | 4.73±1.49 | 4.76±1.38 | 4.70±1.59 | 0.914 |
| TAG/(mmol·L-1) | 1.81±0.94 | 1.84±0.89 | 1.78±1.01 | 0.860 |
| LDL-C/(mmol·L-1) | 2.46±1.06 | 2.42±1.13 | 2.48±1.03 | 0.526 |
| HDL-C/(mmol·L-1) | 1.01±0.35 | 0.95±0.34 | 1.15±0.42 | 0.309 |
| Ca/(mmol·L-1) | 2.21±0.30 | 2.06±0.27 | 2.32±0.28 | 0.871 |
| P/(mmol·L-1) | 1.87±0.61 | 1.93±0.75 | 1.84±0.50 | 0.190 |
| Ca×P/(mg2·dL-2) | 51.00±18.67 | 49.60±21.03 | 51.92±17.33 | 0.376 |
| NT-proBNP/(pg·mL-1) | 7 900 (4 339, 14 025) | 7 650 (4 425, 15 375) | 8 050(4 189, 13 755) | 0.740 |
| PTH/(ng·L-1) | 188.50 (109.25, 305.52) | 175.00 (118.07, 301.0) | 201.15 (87.42, 362.52) | 0.759 |
| SI/(μmol·L-1) | 12.97±4.60 | 11.73±4.47 | 13.80±4.58 | 0.838 |
| TIBC/(μmol·L-1) | 48.94±11.85 | 50.80±12.85 | 47.70±11.24 | 0.547 |
| SF/(ng·mL-1) | 156.50 (67.12, 434.25) | 169.00 (132.50, 417.50) | 143.00 (48.65, 478.50) | 0.438 |
| 24 h urine volume/mL | 500 (50, 1 000) | 550 (313, 1 075) | 495 (0, 950) | 0.351 |
| 24 h ultrafiltration volume/mL | 696 (245, 973) | 660 (401, 938) | 710 (55, 995) | 0.790 |
| rGFR/[mL·(min·1.73 m2)-1] | 0.78±0.84 | 0.53±0.16 | 0.51±0.16 | 0.829 |
| r-Kt/V | 0.40±0.28 | 0.43±0.26 | 0.38±0.29 | 0.513 |
| p-Kt/V | 1.26±0.49 | 1.14±0.51 | 1.35±0.47 | 0.211 |
| t-Kt/V | 1.65±0.40 | 1.55±0.46 | 1.73±0.34 | 0.199 |
| nPCR/(g·kg-1·d-1) | 0.45±0.08 | 0.41±0.06 | 0.48±0.08 | 0.178 |
| Peritoneal transport type/n(%) | 0.874 | |||
| High transport | 42 (35.00) | 14 (35.00) | 28 (35.00) | |
| High average | 51 (42.50) | 18 (45.00) | 33 (41.30) | |
| Low average | 21 (17.50) | 6 (15.00) | 15 (18.70) | |
| Low transport | 6 (5.00) | 2 (5.00) | 4 (5.00) | |
| Baseline medication/n(%) | ||||
| RAS inhibitor | 85 (70.80) | 29 (72.50) | 56 (70.00) | 0.772 |
| β-blocker | 58 (48.30) | 18 (45.00) | 40 (50.00) | 0.602 |
| Calcium channel blocker | 71 (59.20) | 25 (62.50) | 46 (57.50) | 0.598 |
| Diuretic | 45 (37.50) | 14 (35.00) | 31 (38.80) | 0.692 |
| Antiplatelet agent | 38 (31.70) | 11 (27.50) | 27 (33.80) | 0.485 |
| Statin | 52 (43.30) | 16 (40.00) | 36 (45.00) | 0.601 |
| Insulin | 30 (25.00) | 9 (22.50) | 21 (26.30) | 0.654 |
表1 ICO组和对照组基线临床资料的比较
Tab 1 Comparison of baseline clinical characteristics between ICO group and control group
| Item | Total (n=120) | ICO group (n=40) | Control group (n=80) | P value |
|---|---|---|---|---|
| Gender | 0.899 | |||
| Male/n(%) | 62 (51.67) | 21 (52.50) | 41 (51.25) | |
| Female/n(%) | 58 (48.33) | 19 (47.50) | 39 (48.75) | |
| Age/year | 60.25±12.00 | 61.25±8.16 | 59.58±14.13 | 0.080 |
| BMI/(kg·m-2) | 24.14±2.27 | 24.66±1.86 | 23.79±3.25 | 0.296 |
| PD duration/month | 16.5 (9.0, 22.0) | 11.5 (9.0, 20.8) | 17.0 (10.5, 23.8) | 0.342 |
| Smoking/n(%) | 17 (14.17) | 4 (10.00) | 13 (16.25) | 0.583 |
| Comorbidity/n(%) | ||||
| CVD | 23 (19.17) | 9 (22.50) | 14 (17.50) | 0.505 |
| Hypertension | 83 (69.17) | 29 (72.50) | 54 (67.50) | 0.573 |
| Diabetes | 44 (36.67) | 15 (37.50) | 29 (36.25) | 0.894 |
| Cerebral infarction | 7 (5.83) | 2 (5.00) | 5 (6.25) | 0.782 |
| Primary kidney disease/n(%) | 0.260 | |||
| Chronic glomerulonephritis | 58 (48.33) | 17 (42.50) | 41 (51.25) | |
| Diabetic nephropathy | 39 (32.50) | 13 (32.50) | 26 (32.50) | |
| Hypertensive nephropathy | 17 (14.17) | 6 (15.00) | 11 (13.75) | |
| Others | 6 (5.00) | 4 (10.00) | 2 (2.50) | |
| OH/L | 4.35±0.95 | 4.31±0.95 | 4.38±0.97 | 0.809 |
| SBP/mmHg | 142.85±23.92 | 151.88±23.64 | 136.83±22.62 | 0.034 |
| DBP/mmHg | 80.23±12.67 | 83.25±15.22 | 78.21±10.51 | 0.036 |
| Hb/(g·L-1) | 96.12±13.02 | 92.87±14.38 | 98.29±11.85 | 0.202 |
| CRP/(mg·L-1) | 14.14±19.50 | 10.58±12.61 | 16.51±13.04 | 0.057 |
| IL-6/(pg·mL-1) | 24.98±15.08 | 39.57±10.82 | 25.26±13.22 | 0.072 |
| FBG/(mmol·L-1) | 6.45±2.23 | 6.63±3.05 | 6.32±1.52 | 0.712 |
| HbA1c/% | 6.32±1.59 | 6.68±2.17 | 6.08±1.04 | 0.323 |
| Alb/(g·L-1) | 31.82±4.38 | 30.56±4.47 | 32.66±4.2 | 0.146 |
| BUN/(μmol·L-1) | 23.40±5.98 | 22.40±6.04 | 24.37±6.10 | 0.587 |
| TC/(mmol·L-1) | 4.73±1.49 | 4.76±1.38 | 4.70±1.59 | 0.914 |
| TAG/(mmol·L-1) | 1.81±0.94 | 1.84±0.89 | 1.78±1.01 | 0.860 |
| LDL-C/(mmol·L-1) | 2.46±1.06 | 2.42±1.13 | 2.48±1.03 | 0.526 |
| HDL-C/(mmol·L-1) | 1.01±0.35 | 0.95±0.34 | 1.15±0.42 | 0.309 |
| Ca/(mmol·L-1) | 2.21±0.30 | 2.06±0.27 | 2.32±0.28 | 0.871 |
| P/(mmol·L-1) | 1.87±0.61 | 1.93±0.75 | 1.84±0.50 | 0.190 |
| Ca×P/(mg2·dL-2) | 51.00±18.67 | 49.60±21.03 | 51.92±17.33 | 0.376 |
| NT-proBNP/(pg·mL-1) | 7 900 (4 339, 14 025) | 7 650 (4 425, 15 375) | 8 050(4 189, 13 755) | 0.740 |
| PTH/(ng·L-1) | 188.50 (109.25, 305.52) | 175.00 (118.07, 301.0) | 201.15 (87.42, 362.52) | 0.759 |
| SI/(μmol·L-1) | 12.97±4.60 | 11.73±4.47 | 13.80±4.58 | 0.838 |
| TIBC/(μmol·L-1) | 48.94±11.85 | 50.80±12.85 | 47.70±11.24 | 0.547 |
| SF/(ng·mL-1) | 156.50 (67.12, 434.25) | 169.00 (132.50, 417.50) | 143.00 (48.65, 478.50) | 0.438 |
| 24 h urine volume/mL | 500 (50, 1 000) | 550 (313, 1 075) | 495 (0, 950) | 0.351 |
| 24 h ultrafiltration volume/mL | 696 (245, 973) | 660 (401, 938) | 710 (55, 995) | 0.790 |
| rGFR/[mL·(min·1.73 m2)-1] | 0.78±0.84 | 0.53±0.16 | 0.51±0.16 | 0.829 |
| r-Kt/V | 0.40±0.28 | 0.43±0.26 | 0.38±0.29 | 0.513 |
| p-Kt/V | 1.26±0.49 | 1.14±0.51 | 1.35±0.47 | 0.211 |
| t-Kt/V | 1.65±0.40 | 1.55±0.46 | 1.73±0.34 | 0.199 |
| nPCR/(g·kg-1·d-1) | 0.45±0.08 | 0.41±0.06 | 0.48±0.08 | 0.178 |
| Peritoneal transport type/n(%) | 0.874 | |||
| High transport | 42 (35.00) | 14 (35.00) | 28 (35.00) | |
| High average | 51 (42.50) | 18 (45.00) | 33 (41.30) | |
| Low average | 21 (17.50) | 6 (15.00) | 15 (18.70) | |
| Low transport | 6 (5.00) | 2 (5.00) | 4 (5.00) | |
| Baseline medication/n(%) | ||||
| RAS inhibitor | 85 (70.80) | 29 (72.50) | 56 (70.00) | 0.772 |
| β-blocker | 58 (48.30) | 18 (45.00) | 40 (50.00) | 0.602 |
| Calcium channel blocker | 71 (59.20) | 25 (62.50) | 46 (57.50) | 0.598 |
| Diuretic | 45 (37.50) | 14 (35.00) | 31 (38.80) | 0.692 |
| Antiplatelet agent | 38 (31.70) | 11 (27.50) | 27 (33.80) | 0.485 |
| Statin | 52 (43.30) | 16 (40.00) | 36 (45.00) | 0.601 |
| Insulin | 30 (25.00) | 9 (22.50) | 21 (26.30) | 0.654 |
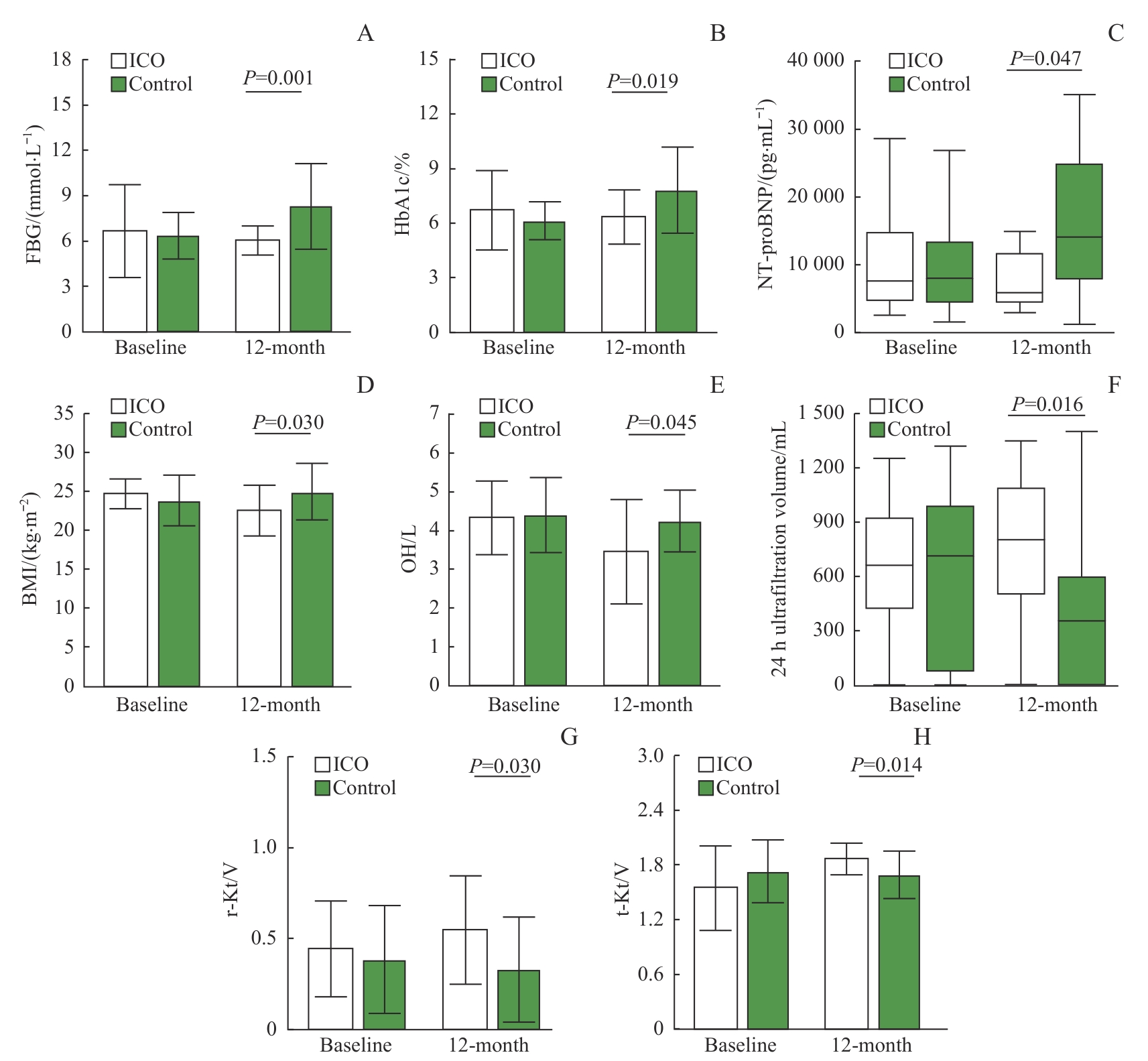
图2 ICO组及对照组透析前后实验室指标及腹透相关指标的变化
Fig 2 Changes in laboratory parameters and peritoneal dialysis-related indicators between ICO group and control groups before and after peritoneal dialysisNote: A. FBG. B. HbA1c. C. NT-proBNP. D. BMI. E. OH. F. 24-h ultrafiltration volume. G. r-Kt/V. H. t-Kt/V.
| Item | Follow-up time | ICO group① | Control group② | P value |
|---|---|---|---|---|
| PASP/mmHg | Baseline | 34.65±6.87 | 32.55±4.40 | 0.099 |
| 12-month | 34.50±5.95 | 32.98±3.24 | 0.168 | |
| LVEDd/mm | Baseline | 51.38±4.02 | 50.96±4.07 | 0.758 |
| 12-month | 48.94±2.98③ | 51.38±4.35 | 0.045 | |
| LVESd/mm | Baseline | 33.00±7.48 | 33.60±6.12 | 0.683 |
| 12-month | 34.10±5.46 | 34.05±5.41 | 0.968 | |
| IVS/mm | Baseline | 10.50±1.55 | 10.38±1.58 | 0.810 |
| 12-month | 10.81±1.05 | 10.50±1.14 | 0.369 | |
| ARD/mmHg | Baseline | 32.06±2.46 | 31.00±2.23 | 0.155 |
| 12-month | 31.56±1.71 | 31.71±2.00 | 0.796 | |
| LAD/mm | Baseline | 39.38±3.40 | 38.63±3.07 | 0.470 |
| 12-month | 38.63±2.47 | 39.00±2.45 | 0.647 | |
| LVEF/% | Baseline | 57.30±4.50 | 59.30±1.50 | 0.095 |
| 12-month | 60.00±4.50④ | 57.50±2.50⑤ | 0.045 | |
| LVMI/(g·m-2) | Baseline | 117.19±10.52 | 114.29±10.30 | 0.401 |
| 12-month | 107.69±8.47⑥ | 111.71±8.51 | 0.038 |
表2 ICO组与对照组患者超声心动图指标比较
Tab 2 Comparison of echocardiographic parameters between the ICO group and the control group
| Item | Follow-up time | ICO group① | Control group② | P value |
|---|---|---|---|---|
| PASP/mmHg | Baseline | 34.65±6.87 | 32.55±4.40 | 0.099 |
| 12-month | 34.50±5.95 | 32.98±3.24 | 0.168 | |
| LVEDd/mm | Baseline | 51.38±4.02 | 50.96±4.07 | 0.758 |
| 12-month | 48.94±2.98③ | 51.38±4.35 | 0.045 | |
| LVESd/mm | Baseline | 33.00±7.48 | 33.60±6.12 | 0.683 |
| 12-month | 34.10±5.46 | 34.05±5.41 | 0.968 | |
| IVS/mm | Baseline | 10.50±1.55 | 10.38±1.58 | 0.810 |
| 12-month | 10.81±1.05 | 10.50±1.14 | 0.369 | |
| ARD/mmHg | Baseline | 32.06±2.46 | 31.00±2.23 | 0.155 |
| 12-month | 31.56±1.71 | 31.71±2.00 | 0.796 | |
| LAD/mm | Baseline | 39.38±3.40 | 38.63±3.07 | 0.470 |
| 12-month | 38.63±2.47 | 39.00±2.45 | 0.647 | |
| LVEF/% | Baseline | 57.30±4.50 | 59.30±1.50 | 0.095 |
| 12-month | 60.00±4.50④ | 57.50±2.50⑤ | 0.045 | |
| LVMI/(g·m-2) | Baseline | 117.19±10.52 | 114.29±10.30 | 0.401 |
| 12-month | 107.69±8.47⑥ | 111.71±8.51 | 0.038 |
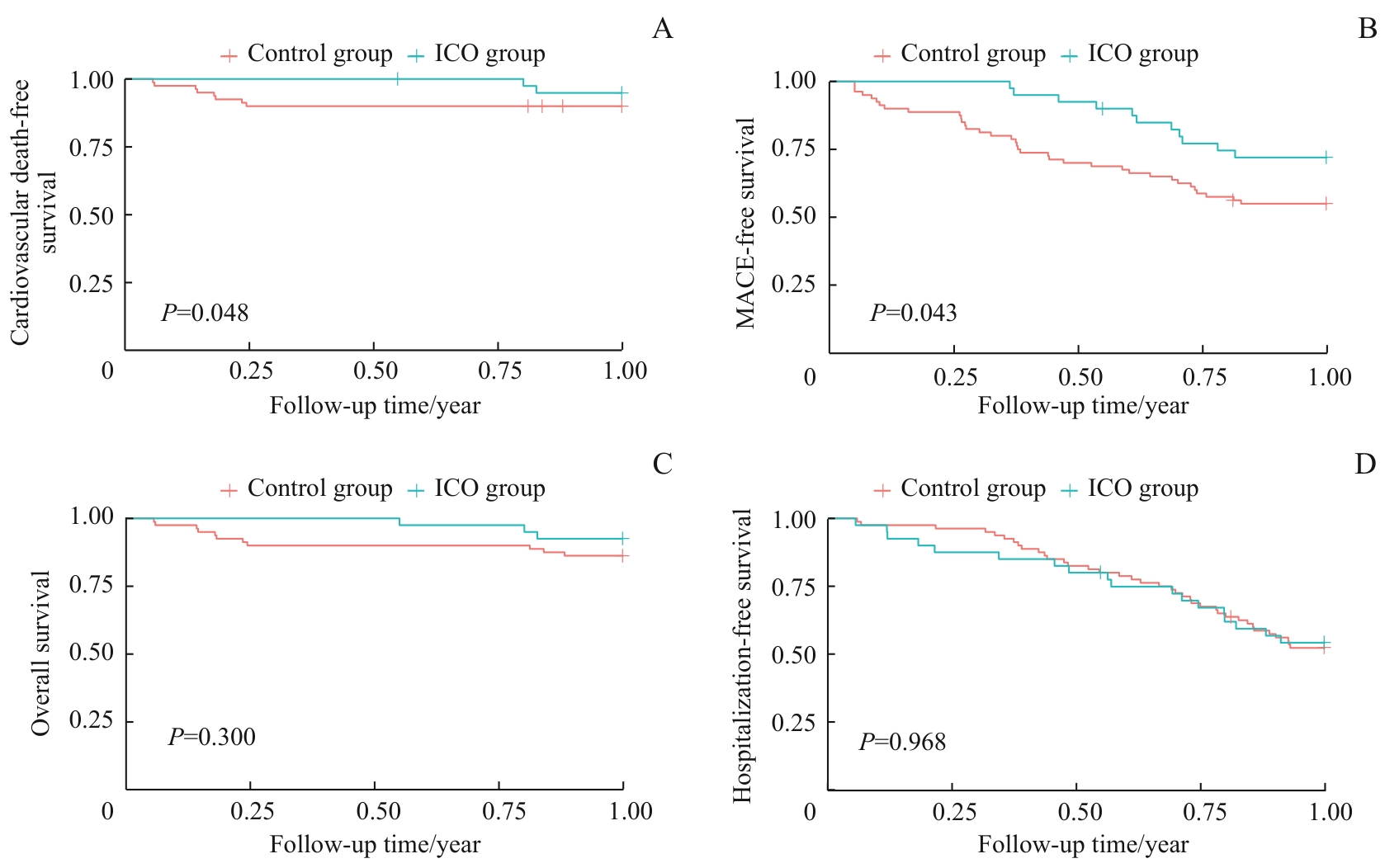
图3 ICO组与对照组患者心血管死亡率(A)、MACE发生率(B)、全因死亡率(C)、住院率(D)的Kaplan-Meier生存曲线比较
Fig 3 Comparison of Kaplan-Meier survival curves for cardiovascular mortality (A), MACE incidence (B), all-cause mortality (C), and hospitalization rate (D) between the ICO group and the control group
| Factor | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P value | HR | 95%CI | P value | |
| Age (per year increase) | 2.50 | 1.38‒3.30 | 0.028 | 2.4 | 1.48‒3.40 | 0.112 |
| PD duration (per month increase) | 3.81 | 2.90‒4.80 | 0.898 | |||
| Diabetes (Yes vs No) | 1.32 | 1.27‒2.80 | 0.039 | 1.23 | 0.98‒3.44 | 0.078 |
| Concomitant CVD (Yes vs No) | 0.41 | 0.17‒0.89 | 0.029 | 1.57 | 1.07‒2.33 | 0.035 |
| Use of ICO (Yes vs No) | 0.41 | 0.28‒0.80 | 0.015 | 0.35 | 0.17‒0.89 | 0.012 |
| High peritoneal transport (Yes vs No) | 1.92 | 1.15‒3.45 | 0.021 | 1.65 | 1.08‒2.89 | 0.045 |
| OH (per 0.1 L increase) | 2.53 | 1.80‒3.40 | 0.104 | |||
| HbA1c (per 1% increase) | 0.72 | 0.39‒0.94 | 0.109 | |||
| Alb (per 1 g·L-1 decrease) | 0.81 | 0.64‒1.15 | 0.541 | |||
| NT-proBNP (per 100 pg·mL-1 increase) | 1.42 | 1.02‒2.50 | 0.024 | 1.38 | 1.13‒2.89 | 0.013 |
| CRP (per 1 mg·L-1 increase) | 1.15 | 1.05‒1.26 | 0.003 | 1.10 | 1.01‒1.20 | 0.054 |
| t-Kt/V (per 0.1 decrease) | 0.83 | 0.33‒0.97 | 0.023 | 0.99 | 0.29‒1.02 | 0.088 |
| r-Kt/V (per 0.1 decrease) | 1.25 | 1.08‒1.45 | 0.003 | 1.15 | 0.98‒1.34 | 0.089 |
| Use of RAS inhibitor (Yes vs No) | 0.55 | 0.31‒0.98 | 0.042 | 0.61 | 0.34‒1.09 | 0.095 |
表3 腹透患者发生MACE的危险因素分析 (n=120,Cox回归模型)
Tab 3 Aanlysis of risk factors for MACE in patients undergoing PD (n=120, Cox regression model)
| Factor | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P value | HR | 95%CI | P value | |
| Age (per year increase) | 2.50 | 1.38‒3.30 | 0.028 | 2.4 | 1.48‒3.40 | 0.112 |
| PD duration (per month increase) | 3.81 | 2.90‒4.80 | 0.898 | |||
| Diabetes (Yes vs No) | 1.32 | 1.27‒2.80 | 0.039 | 1.23 | 0.98‒3.44 | 0.078 |
| Concomitant CVD (Yes vs No) | 0.41 | 0.17‒0.89 | 0.029 | 1.57 | 1.07‒2.33 | 0.035 |
| Use of ICO (Yes vs No) | 0.41 | 0.28‒0.80 | 0.015 | 0.35 | 0.17‒0.89 | 0.012 |
| High peritoneal transport (Yes vs No) | 1.92 | 1.15‒3.45 | 0.021 | 1.65 | 1.08‒2.89 | 0.045 |
| OH (per 0.1 L increase) | 2.53 | 1.80‒3.40 | 0.104 | |||
| HbA1c (per 1% increase) | 0.72 | 0.39‒0.94 | 0.109 | |||
| Alb (per 1 g·L-1 decrease) | 0.81 | 0.64‒1.15 | 0.541 | |||
| NT-proBNP (per 100 pg·mL-1 increase) | 1.42 | 1.02‒2.50 | 0.024 | 1.38 | 1.13‒2.89 | 0.013 |
| CRP (per 1 mg·L-1 increase) | 1.15 | 1.05‒1.26 | 0.003 | 1.10 | 1.01‒1.20 | 0.054 |
| t-Kt/V (per 0.1 decrease) | 0.83 | 0.33‒0.97 | 0.023 | 0.99 | 0.29‒1.02 | 0.088 |
| r-Kt/V (per 0.1 decrease) | 1.25 | 1.08‒1.45 | 0.003 | 1.15 | 0.98‒1.34 | 0.089 |
| Use of RAS inhibitor (Yes vs No) | 0.55 | 0.31‒0.98 | 0.042 | 0.61 | 0.34‒1.09 | 0.095 |
| Adverse event type | ICO group (n=40) | Control group (n=80) | P value |
|---|---|---|---|
| Infectious complication | 8 (20.00) | 14 (17.50) | 0.735 |
| Peritonitis | 5 (12.50) | 10 (12.50) | 1.000 |
| Catheter-related infection | 3 (7.50) | 4 (5.00) | 0.584 |
| Non-infectious complication | 7 (17.50) | 14 (17.50) | 1.000 |
| Peritoneal dialysis catheter displacement | 3 (7.50) | 3 (3.75) | 0.393 |
| Severe electrolyte disorder | 2 (5.00) | 4 (5.00) | 1.000 |
| Severe constipation or diarrhea | 2 (5.00) | 7 (8.75) | 0.716 |
表4 ICO组与对照组患者不良事件比较 [n(%)]
Tab 4 Comparison of adverse events between the ICO group and the control group [n(%)]
| Adverse event type | ICO group (n=40) | Control group (n=80) | P value |
|---|---|---|---|
| Infectious complication | 8 (20.00) | 14 (17.50) | 0.735 |
| Peritonitis | 5 (12.50) | 10 (12.50) | 1.000 |
| Catheter-related infection | 3 (7.50) | 4 (5.00) | 0.584 |
| Non-infectious complication | 7 (17.50) | 14 (17.50) | 1.000 |
| Peritoneal dialysis catheter displacement | 3 (7.50) | 3 (3.75) | 0.393 |
| Severe electrolyte disorder | 2 (5.00) | 4 (5.00) | 1.000 |
| Severe constipation or diarrhea | 2 (5.00) | 7 (8.75) | 0.716 |
| [1] | Goossen K, Becker M, Marshall M R, et al. Icodextrin versus glucose solutions for the once-daily long dwell in peritoneal dialysis: an enriched systematic review and meta-analysis of randomized controlled trials[J]. Am J Kidney Dis, 2020, 75(6): 830-846. |
| [2] | Himmelfarb J, Vanholder R, Mehrotra R, et al. The current and future landscape of dialysis[J]. Nat Rev Nephrol, 2020, 16(10): 573-585. |
| [3] | Ahmad M, Shah H, Pliakogiannis T, et al. Prevention of membrane damage in patient on peritoneal dialysis with new peritoneal dialysis solutions[J]. Int Urol Nephrol, 2007, 39(1): 299-312. |
| [4] | Olszowska A, Waniewski J, Stachowska-Pietka J, et al. Long peritoneal dialysis dwells with icodextrin: kinetics of transperitoneal fluid and polyglucose transport[J]. Front Physiol, 2019, 10: 1326. |
| [5] | Kunin M, Beckerman P. The peritoneal membrane: a potential mediator of fibrosis and inflammation among heart failure patients on peritoneal dialysis[J]. Membranes, 2022, 12(3): 318. |
| [6] | Grzywacz A, Lubas A, Smoszna J, et al. Risk factors associated with all-cause death among dialysis patients with diabetes[J]. Med Sci Monit, 2021, 27: e930152. |
| [7] | Chang T I, Ryu D R, Yoo T H, et al. Effect of icodextrin solution on the preservation of residual renal function in peritoneal dialysis patients: a randomized controlled study[J]. Medicine, 2016, 95(13): e2991. |
| [8] | 肖一凡. 基于真实世界的艾考糊精腹膜透析液疗效分析[D]. 沈阳: 中国医科大学, 2024. |
| Xiao Y F. Analysis of the therapeutic effect of icodextrin peritoneal dialysate based on the real world[D]. Shenyang: China Medical University, 2024. | |
| [9] | Morelle J, Sow A, Fustin C A, et al. Mechanisms of crystalloid versus colloid osmosis across the peritoneal membrane[J]. J Am Soc Nephrol, 2018, 29(7): 1875-1886. |
| [10] | Dousdampanis P, Musso C G, Trigka K. Icodextrin and peritoneal dialysis: advantages and new applications[J]. Int Urol Nephrol, 2018, 50(3): 495-500. |
| [11] | 阳晓, 严骏飞, 余学清. 艾考糊精腹透液的临床优势及获益人群[J]. 中华肾脏病杂志, 2021, 37(6): 528-533. |
| Yang X, Yan J F, Yu X Q. Clinical advantages of icodextrin peritoneal dialysis solution and its beneficial population[J]. Chinese Journal of Nephrology, 2021, 37(6): 528-533. | |
| [12] | Wang I K, Lin C L, Yen T H, et al. Icodextrin reduces the risk of congestive heart failure in peritoneal dialysis patients[J]. Pharmacoepidemiol Drug Saf, 2018, 27(4): 447-452. |
| [13] | Paniagua R, Orihuela O, Ventura M J, et al. Echocardiographic, electrocardiographic and blood pressure changes induced by icodextrin solution in diabetic patients on peritoneal dialysis[J]. Kidney Int, 2008, 73: S125-S130. |
| [14] | Yoon H E, Chang Y K, Shin S J, et al. Benefits of a continuous ambulatory peritoneal dialysis (CAPD) technique with one icodextrin-containing and two biocompatible glucose-containing dialysates for preservation of residual renal function and biocompatibility in incident CAPD patients[J]. J Korean Med Sci, 2014, 29(9): 1217-1225. |
| [15] | Takatori Y, Akagi S, Sugiyama H, et al. Icodextrin increases technique survival rate in peritoneal dialysis patients with diabetic nephropathy by improving body fluid management: a randomized controlled trial[J]. Clin J Am Soc Nephrol, 2011, 6(6): 1337-1344. |
| [16] | Gokal R, Moberly J, Lindholm B, et al. Metabolic and laboratory effects of icodextrin[J]. Kidney Int, 2002, 62: S62-S71. |
| [17] | Kadiroğlu AK, Ustündag S, Kayabaşi H, et al. A comparative study of the effect of icodextrin based peritoneal dialysis and hemodialysis on lipid metabolism[J]. Indian J Nephrol, 2013, 23(5): 358. |
| [18] | Ng J K, Chan G C, Li P K. Icodextrin in peritoneal dialysis: implications on clinical practice and survival outcome[J]. Kidney360, 2022, 3(5): 793-795. |
| [19] | Kim Y L, van Biesen W. Fluid overload in peritoneal dialysis patients[J]. Semin Nephrol, 2017, 37(1): 43-53. |
| [20] | Davies S, Zhao J H, McCullough K P, et al. International icodextrin use and association with peritoneal membrane function, fluid removal, patient and technique survival[J]. Kidney360, 2022, 3(5): 872-882. |
| [21] | 林爱武, 钱家麒, 李晓玫, 等. 腹膜转运特性明显影响艾考糊精腹透液的超滤量[J]. 中华肾脏病杂志, 2010, 26(7): 504-509. |
| Lin A W, Qian J Q, Li X M, et al. Great influence of peritoneal transport characteristics on ultrafiltration of icodextrin[J]. Chinese Journal of Nephrology, 2010, 26(7): 504-509. | |
| [22] | Lui S L, Yung S, Yim A, et al. A combination of biocompatible peritoneal dialysis solutions and residual renal function, peritoneal transport, and inflammation markers: a randomized clinical trial[J]. Am J Kidney Dis, 2012, 60(6): 966-975. |
| [23] | 徐光, 任东升, 陶雅非, 等. 艾考糊精透析液治疗维持性腹膜透析容量超负荷患者疗效观察[J]. 中华实用诊断与治疗杂志, 2023, 37(6): 637-640. |
| Xu G, Ren D S, Tao Y F, et al. Effect of icodextrin in maintenance peritoneal dialysis volume overload patients[J]. Journal of Chinese Practical Diagnosis and Therapy, 2023, 37(6): 637-640. | |
| [24] | Sav T, Inanc M T, Dogan A, et al. Two daytime icodextrin exchanges decrease brain natriuretic peptide levels and improve cardiac functions in continuous ambulatory peritoneal dialysis patients[J]. Nephrology, 2010, 15(3): 307-312. |
| [25] | Paniagua R, Ventura M D J, Ávila-Díaz M, et al. Icodextrin improves metabolic and fluid management in high and high-average transport diabetic patients[J]. Perit Dial Int, 2009, 29(4): 422-432. |
| [26] | Cnossen T T, Konings C J, van der Sande F M, et al. Clinical effects of icodextrin in peritoneal dialysis[J]. NDT Plus, 2008, 1(suppl 4): iv18-iv22. |
| [27] | 吴杏, 叶任高, 汪涛, 等. 尿毒症患者发生左心室肥厚的危险性及其相关因素[J]. 中国中西医结合肾病杂志, 2004, 5(1): 18-20. |
| Wu X, Ye R G, Wang T, et al. Risk factors of left ventricular hypertrophy (LVH) and its relationship with blood volume of uremic patients[J]. Chinese Journal of Integrated Traditional and Western Nephrology, 2004, 5(1): 18-20. | |
| [28] | Konings C J A M, Kooman J P, Schonck M, et al. Effect of icodextrin on volume status, blood pressure and echocardiographic parameters: a randomized study[J]. Kidney Int, 2003, 63(4): 1556-1563. |
| [29] | 鲍霞, 徐佳美, 黄春香, 等. 艾考糊精透析液在腹膜透析患者心力衰竭中的应用效果观察[J]. 中国中西医结合肾病杂志, 2025, 26(3): 234-236. |
| Bao X, Xu J M, Huang C X, et al. Effect of icodextrin dialysate on heart failure in peritoneal dialysis patients[J]. Chinese Journal of Integrated Traditional and Western Nephrology, 2025, 26(3): 234-236. | |
| [30] | Rodríguez-Carmona A, Fontán M P, López E G, et al. Use of icodextrin during nocturnal automated peritoneal dialysis allows sustained ultrafiltration while reducing the peritoneal glucose load: a randomized crossover study[J]. Perit Dial Int, 2007, 27(3): 260-266. |
| [31] | 彭凯月, 韩庆烽. 基于艾考糊精透析液的腹膜透析治疗进展[J]. 中国血液净化, 2022, 21(8): 595-598. |
| Peng K Y, Han Q F. Progress in peritoneal dialysis treatment based on icodextrin[J]. Chinese Journal of Blood Purification, 2022, 21(8): 595-598. | |
| [32] | 中华医学会肾脏病学分会, 中关村肾病血液净化创新联盟. 中国透析患者慢性心力衰竭管理指南[J]. 中华肾脏病杂志, 2022, 38(5): 465-496. |
| Chinese Society of Nephrology, Zhongguancun Nephrology & Blood Purification Innovation Alliance. Guidelines for the management of chronic heart failure in dialysis patients in China[J]. Chinese Journal of Nephrology, 2022, 38(5): 465-496. | |
| [33] | Woodrow G, Oldroyd B, Stables G, et al. Effects of icodextrin in automated peritoneal dialysis on blood pressure and bioelectrical impedance analysis[J]. Nephrol Dial Transplant, 2000, 15(6): 862-866. |
| [34] | Rangaswamy D, Guddattu V, Webster A C, et al. Icodextrin use for peritoneal dialysis in Australia: a cohort study using Australia and New Zealand Dialysis and Transplant Registry[J]. Perit Dial Int, 2020, 40(2): 209-219. |
| [35] | Han S H, Ahn S V, Yun J Y, et al. Effects of icodextrin on patient survival and technique success in patients undergoing peritoneal dialysis[J]. Nephrol Dial Transplant, 2012, 27(5): 2044-2050. |
| [36] | Wang I K, Li Y F, Chen J H, et al. Icodextrin decreases technique failure and improves patient survival in peritoneal dialysis patients[J]. Nephrology, 2015, 20(3): 161-167. |
| [37] | Wang I K, Chan C I, Lin A H, et al. The impact of icodextrin on the outcomes of incident peritoneal dialysis patients[J]. PLoS One, 2024, 19(3): e0297688. |
| [1] | 李玉, 张羽. 慢性肾脏病患者不良妊娠结局的危险因素分析[J]. 上海交通大学学报(医学版), 2024, 44(5): 560-566. |
| [2] | 李萍, 蒋惠如, 叶梦月, 王雅玉, 陈潇雨, 袁安彩, 徐文杰, 戴慧敏, 陈曦, 闫小响, 涂圣贤, 郑元琦, 张薇, 卜军. 基于上海社区老年人群队列的心血管疾病和恶性肿瘤的危险因素流行特征分析[J]. 上海交通大学学报(医学版), 2024, 44(5): 617-625. |
| [3] | 郑梦奕, 毛家亮, 邹治国, 张瑞雷, 张厚, 李世光. 全身免疫炎症指数及躯体化症状评分对首发心梗PCI术后发生院内主要不良心血管事件的预测价值[J]. 上海交通大学学报(医学版), 2024, 44(3): 334-341. |
| [4] | 吴丽蓉, 陈瑞华, 晁筱雯, 郭雨槐, 孙涛, 李梦慈, 陈天璐. 空腹血糖升高与认知功能恶化的代谢关联研究[J]. 上海交通大学学报(医学版), 2024, 44(2): 212-222. |
| [5] | 沈力, 黄亨烨, 于广军. 早中期早产儿校正18月龄神经发育状况和影响因素[J]. 上海交通大学学报(医学版), 2023, 43(4): 445-452. |
| [6] | 姜静, 卞勇, 郑吉建, 黄悦. 狭颅症儿童颅骨修补术中出血量的影响因素[J]. 上海交通大学学报(医学版), 2023, 43(4): 453-458. |
| [7] | 薛淋淋, 李秉翰, 常丽仙, 李卫昆, 刘春云, 刘立. 丙型病毒性肝炎肝硬化失代偿期患者发生细菌感染的列线图预测模型构建及评价[J]. 上海交通大学学报(医学版), 2023, 43(1): 52-60. |
| [8] | 魏珊, 纪鸥洋, 陈志豪, 黄泽慧, 李璞, 方均燕, 刘英莉. 维持性透析患者安全用药知信行现状调查及相关因素分析[J]. 上海交通大学学报(医学版), 2023, 43(1): 88-94. |
| [9] | 朱月悦, 张锦文, 马锐翔, 陈彩莲, 林羿, 刘晓瑞. 产后血栓性疾病的危险因素分析[J]. 上海交通大学学报(医学版), 2022, 42(4): 415-421. |
| [10] | 张彤, 田雪, 左颖婷, 郑曼琪, 张怡君, 吴寿岭, 陈朔华, 马高亭, 佟旭, 王安心, 莫大鹏. 无传统危险因素人群中TyG指数与心脑血管疾病的关系[J]. 上海交通大学学报(医学版), 2022, 42(3): 267-274. |
| [11] | 李爱求, 张潇潇, 姜允丽, 肖艳赏, 丁国栋, 吴蓓蓉, 董晓艳. 学龄前儿童反复喘息的相关危险因素分析[J]. 上海交通大学学报(医学版), 2022, 42(10): 1435-1440. |
| [12] | 黄泽慧, 胡春, 李璞, 张春丽, 方均燕, 宋阿会, 魏珊, 纪鸥洋, 佟琰, 邓海, 刘英莉. 居家腹膜透析患者自我管理量表的编制及信度、效度分析研究[J]. 上海交通大学学报(医学版), 2021, 41(7): 942-948. |
| [13] | 丁远森, 王枫, 孙家悦, 邵正威, 邹德荣, 陆家瑜. 不同年龄2型糖尿病患者牙周健康流行病学调查[J]. 上海交通大学学报(医学版), 2021, 41(2): 217-222. |
| [14] | 佟琰, 方均燕, 邓海, 宋阿会, 李璞, 刘英莉. 腹膜透析滤出液外泌体miR-200a在不同腹膜转运特性患者中的表达差异及其生物学功能预测[J]. 上海交通大学学报(医学版), 2021, 41(1): 42-48. |
| [15] | 马银珠*,陆光华*,钟 娜,王海红,和 申,赵 雪,江海峰,王 振. 酒精所致精神病性障碍男性患者临床特征及危险因素[J]. 上海交通大学学报(医学版), 2020, 40(9): 1256-1262. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||