Journal of Shanghai Jiao Tong University (Medical Science) ›› 2026, Vol. 46 ›› Issue (5): 612-623.doi: 10.3969/j.issn.1674-8115.2026.05.007
• Clinical research • Previous Articles
Liu Zhitong, Fan Zixu, Li Xiang, Zhang Min( )
)
Received:2025-11-24
Accepted:2026-01-19
Online:2026-05-28
Published:2026-05-28
Contact:
Zhang Min
E-mail:zhangminxk@126.com
Supported by:CLC Number:
Liu Zhitong, Fan Zixu, Li Xiang, Zhang Min. Safety outcomes of immunotherapy continuation versus permanent discontinuation after immune checkpoint inhibitor-associated myocarditis in patients with lung cancer[J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(5): 612-623.
Add to citation manager EndNote|Ris|BibTeX
URL: https://xuebao.shsmu.edu.cn/EN/10.3969/j.issn.1674-8115.2026.05.007
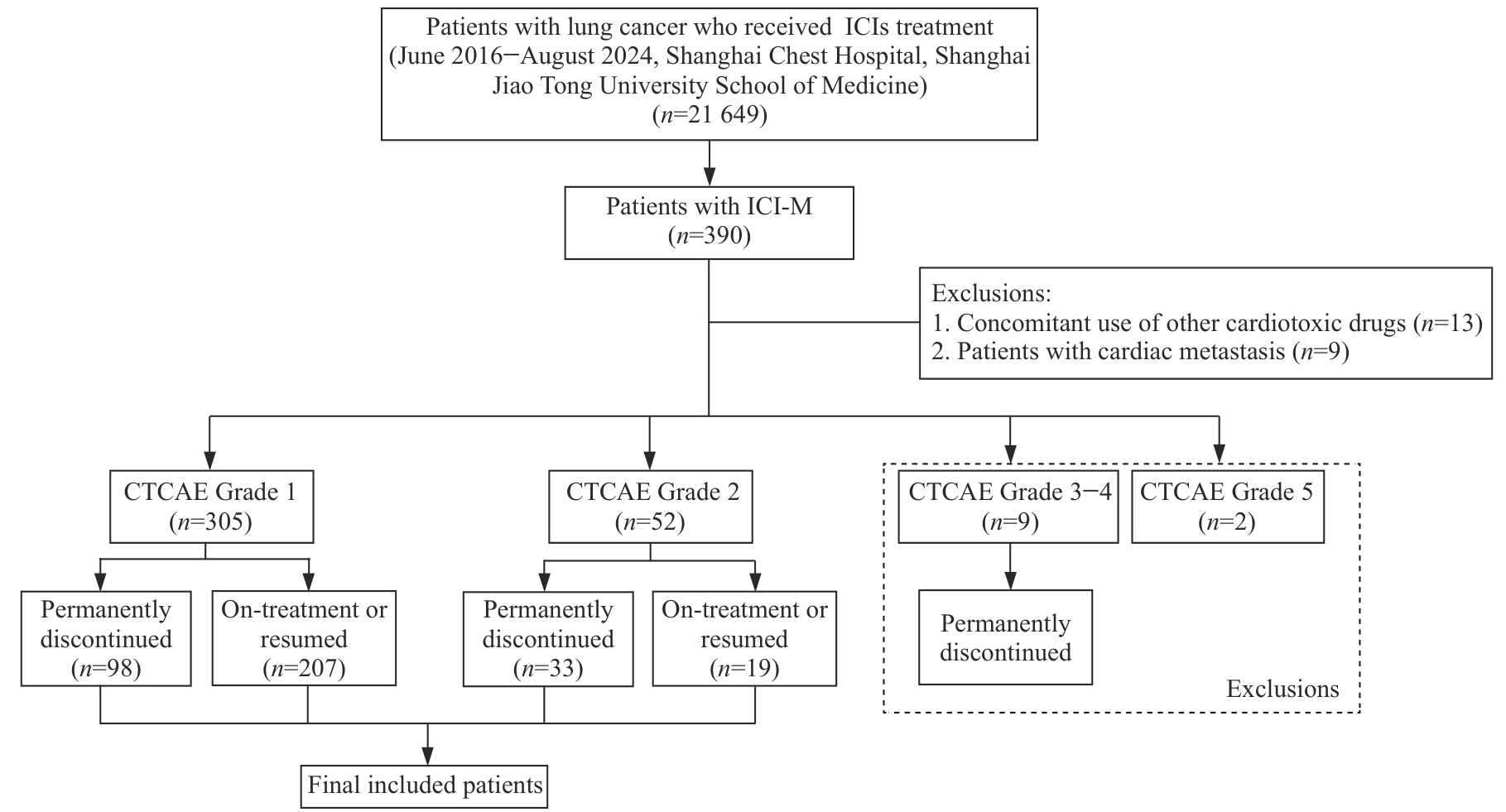
Fig 1 Flowchart of the study design
| Characteristic | CTCAE Grade 1 (n=305) | CTCAE Grade 2 (n=52) | P value | ||
|---|---|---|---|---|---|
| On-treatment or resumed (n=207) | Permanently discontinued (n=98) | On-treatment or resumed (n=19) | Permanently discontinued (n=33) | ||
| Clinical characteristic | |||||
| Age/year | 67.0 (61.0, 71.0) | 68.0 (61.0, 73.0) | 64.0 (61.0, 72.0) | 66.0 (62.0, 69.0) | 0.593 |
| Male/n(%) | 185 (89.4) | 74 (75.5) | 16 (84.2) | 27 (81.8) | 0.018 |
| BMI/(kg·m-2) | 22.6 (20.3, 24.7) | 22.5 (20.4, 24.9) | 23.1 (21.0, 24.5) | 22.9 (22.2, 25.6) | 0.392 |
| Coronary artery disease/n(%) | 33 (15.9) | 16 (16.3) | 6 (31.6) | 10 (30.3) | 0.091 |
| Hyperlipidemia/n(%) | 13 (6.3) | 7 (7.1) | 1 (5.3) | 3 (9.1) | 0.929 |
| Hypertension/n(%) | 77 (37.2) | 35 (35.7) | 4 (21.1) | 10 (30.3) | 0.497 |
| Diabetes/n(%) | 26 (12.6) | 13 (13.3) | 3 (15.8) | 6 (18.2) | 0.832 |
| Chronic kidney disease/n(%) | 5 (2.4) | 4 (4.1) | 0 (0) | 1 (3.3) | 0.739 |
| Histology/n(%) | 0.583 | ||||
| Squamous cell carcinoma | 74 (35.7) | 30 (30.6) | 7 (36.8) | 10 (30.3) | |
| Adenocarcinoma | 84 (40.6) | 47 (48.0) | 8 (42.1) | 14 (42.4) | |
| Other NSCLC | 26 (12.6) | 7 (7.1) | 2 (10.5) | 7 (21.2) | |
| SCLC | 23 (11.1) | 14 (14.3) | 2 (10.5) | 2 (6.1) | |
| Disease stage/n(%) | 0.265 | ||||
| Stage Ⅱ‒Ⅲ | 78 (37.7) | 28 (28.6) | 4 (21.1) | 11 (33.3) | |
| Stage Ⅳ | 129 (62.3) | 70 (71.4) | 15 (78.9) | 22 (66.7) | |
| ECOG performance status①/n(%) | 0.072 | ||||
| 0 | 24 (14.3) | 4 (5.2) | 0 (0) | 3 (12.5) | |
| 1 | 143 (85.1) | 71 (92.2) | 9 (90.0) | 20 (83.3) | |
| 2 | 1 (0.6) | 2 (2.6) | 1 (10.0) | 1 (4.2) | |
| Baseline laboratory test | |||||
| Hemoglobin/(g·L-1) | 129.0 (116.0, 141.0) | 126.5 (115.0, 139.0) | 132.0 (128.0, 144.0) | 127.0 (116.0, 139.0) | 0.550 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 41.0 (38.0, 42.0) | 39.0 (37.0, 42.0) | 0.794 |
| HbA1c/% | 5.8 (5.6, 6.3) | 5.8 (5.3, 6.5) | 5.8 (5.3, 6.7) | 6.0 (5.7, 6.2) | 0.803 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.8 (85.9, 101.1) | 94.3 (77.8, 100.9) | 99.0 (85.9, 103.4) | 91.5 (78.3, 95.9) | 0.237 |
| Anti-tumor therapy | |||||
| Radiotherapy/n(%) | 67 (32.4) | 33 (33.7) | 7 (36.8) | 11 (33.3) | 0.980 |
| Initial ICI type/n(%) | 0.522 | ||||
| PD-1i monotherapy | 170 (82.1) | 83 (84.7) | 18 (94.7) | 29 (87.9) | |
| PD-L1i monotherapy | 29 (14.0) | 14 (14.3) | 1 (5.3) | 4 (12.1) | |
| Combination therapy | 8 (3.9) | 1 (1.0) | 0 (0) | 0 (0) | |
| Number of cycles received prior to ICI-M | 2.0 (1.0, 5.0) | 3.0 (2.0, 6.0) | 3.0 (2.0, 7.5) | 2.0 (1.0, 3.0) | 0.131 |
| Ongoing treatment/n(%) | 0.184 | ||||
| ICIs monotherapy | 42 (20.3) | 16 (16.3) | 7 (36.8) | 7 (21.2) | |
| Combination with chemotherapy | 138 (66.7) | 69 (70.4) | 10 (52.6) | 20 (60.6) | |
| Combination with targeted therapy | 17 (8.2) | 8 (8.2) | 0 (0) | 1 (3.0) | |
| Combination with chemotherapy and targeted therapy | 10 (4.8) | 5 (5.1) | 2 (10.5) | 5 (15.2) | |
| Clinical characteristics of initial ICI-M | |||||
| Time to initial ICI-M/month | 2.0 (1.0, 5.0) | 3.0 (1.0, 6.0) | 3.0 (1.0, 7.5) | 2.0 (1.0, 3.0) | 0.073 |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 140.0) | 90.0 (60.0, 190.0) | 310.0 (130.0, 550.0) | 390.0 (120.0, 610.0) | <0.001 |
| Peak CK-MB/(ng·mL-1) | 3.0 (1.8, 6.3) | 3.5 (1.8, 12.1) | 4.4 (2.8, 10.1) | 11.0 (3.5, 73.7) | <0.001 |
| Management/n(%) | |||||
| Hospitalization | 17 (8.2) | 24 (24.5) | 11 (57.9) | 22 (66.7) | <0.001 |
| Systemic steroids use | 13 (6.3) | 25 (25.5) | 3 (15.8) | 21 (63.6) | <0.001 |
Tab 1 Baseline characteristics of patients with ICI-M
| Characteristic | CTCAE Grade 1 (n=305) | CTCAE Grade 2 (n=52) | P value | ||
|---|---|---|---|---|---|
| On-treatment or resumed (n=207) | Permanently discontinued (n=98) | On-treatment or resumed (n=19) | Permanently discontinued (n=33) | ||
| Clinical characteristic | |||||
| Age/year | 67.0 (61.0, 71.0) | 68.0 (61.0, 73.0) | 64.0 (61.0, 72.0) | 66.0 (62.0, 69.0) | 0.593 |
| Male/n(%) | 185 (89.4) | 74 (75.5) | 16 (84.2) | 27 (81.8) | 0.018 |
| BMI/(kg·m-2) | 22.6 (20.3, 24.7) | 22.5 (20.4, 24.9) | 23.1 (21.0, 24.5) | 22.9 (22.2, 25.6) | 0.392 |
| Coronary artery disease/n(%) | 33 (15.9) | 16 (16.3) | 6 (31.6) | 10 (30.3) | 0.091 |
| Hyperlipidemia/n(%) | 13 (6.3) | 7 (7.1) | 1 (5.3) | 3 (9.1) | 0.929 |
| Hypertension/n(%) | 77 (37.2) | 35 (35.7) | 4 (21.1) | 10 (30.3) | 0.497 |
| Diabetes/n(%) | 26 (12.6) | 13 (13.3) | 3 (15.8) | 6 (18.2) | 0.832 |
| Chronic kidney disease/n(%) | 5 (2.4) | 4 (4.1) | 0 (0) | 1 (3.3) | 0.739 |
| Histology/n(%) | 0.583 | ||||
| Squamous cell carcinoma | 74 (35.7) | 30 (30.6) | 7 (36.8) | 10 (30.3) | |
| Adenocarcinoma | 84 (40.6) | 47 (48.0) | 8 (42.1) | 14 (42.4) | |
| Other NSCLC | 26 (12.6) | 7 (7.1) | 2 (10.5) | 7 (21.2) | |
| SCLC | 23 (11.1) | 14 (14.3) | 2 (10.5) | 2 (6.1) | |
| Disease stage/n(%) | 0.265 | ||||
| Stage Ⅱ‒Ⅲ | 78 (37.7) | 28 (28.6) | 4 (21.1) | 11 (33.3) | |
| Stage Ⅳ | 129 (62.3) | 70 (71.4) | 15 (78.9) | 22 (66.7) | |
| ECOG performance status①/n(%) | 0.072 | ||||
| 0 | 24 (14.3) | 4 (5.2) | 0 (0) | 3 (12.5) | |
| 1 | 143 (85.1) | 71 (92.2) | 9 (90.0) | 20 (83.3) | |
| 2 | 1 (0.6) | 2 (2.6) | 1 (10.0) | 1 (4.2) | |
| Baseline laboratory test | |||||
| Hemoglobin/(g·L-1) | 129.0 (116.0, 141.0) | 126.5 (115.0, 139.0) | 132.0 (128.0, 144.0) | 127.0 (116.0, 139.0) | 0.550 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 41.0 (38.0, 42.0) | 39.0 (37.0, 42.0) | 0.794 |
| HbA1c/% | 5.8 (5.6, 6.3) | 5.8 (5.3, 6.5) | 5.8 (5.3, 6.7) | 6.0 (5.7, 6.2) | 0.803 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.8 (85.9, 101.1) | 94.3 (77.8, 100.9) | 99.0 (85.9, 103.4) | 91.5 (78.3, 95.9) | 0.237 |
| Anti-tumor therapy | |||||
| Radiotherapy/n(%) | 67 (32.4) | 33 (33.7) | 7 (36.8) | 11 (33.3) | 0.980 |
| Initial ICI type/n(%) | 0.522 | ||||
| PD-1i monotherapy | 170 (82.1) | 83 (84.7) | 18 (94.7) | 29 (87.9) | |
| PD-L1i monotherapy | 29 (14.0) | 14 (14.3) | 1 (5.3) | 4 (12.1) | |
| Combination therapy | 8 (3.9) | 1 (1.0) | 0 (0) | 0 (0) | |
| Number of cycles received prior to ICI-M | 2.0 (1.0, 5.0) | 3.0 (2.0, 6.0) | 3.0 (2.0, 7.5) | 2.0 (1.0, 3.0) | 0.131 |
| Ongoing treatment/n(%) | 0.184 | ||||
| ICIs monotherapy | 42 (20.3) | 16 (16.3) | 7 (36.8) | 7 (21.2) | |
| Combination with chemotherapy | 138 (66.7) | 69 (70.4) | 10 (52.6) | 20 (60.6) | |
| Combination with targeted therapy | 17 (8.2) | 8 (8.2) | 0 (0) | 1 (3.0) | |
| Combination with chemotherapy and targeted therapy | 10 (4.8) | 5 (5.1) | 2 (10.5) | 5 (15.2) | |
| Clinical characteristics of initial ICI-M | |||||
| Time to initial ICI-M/month | 2.0 (1.0, 5.0) | 3.0 (1.0, 6.0) | 3.0 (1.0, 7.5) | 2.0 (1.0, 3.0) | 0.073 |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 140.0) | 90.0 (60.0, 190.0) | 310.0 (130.0, 550.0) | 390.0 (120.0, 610.0) | <0.001 |
| Peak CK-MB/(ng·mL-1) | 3.0 (1.8, 6.3) | 3.5 (1.8, 12.1) | 4.4 (2.8, 10.1) | 11.0 (3.5, 73.7) | <0.001 |
| Management/n(%) | |||||
| Hospitalization | 17 (8.2) | 24 (24.5) | 11 (57.9) | 22 (66.7) | <0.001 |
| Systemic steroids use | 13 (6.3) | 25 (25.5) | 3 (15.8) | 21 (63.6) | <0.001 |
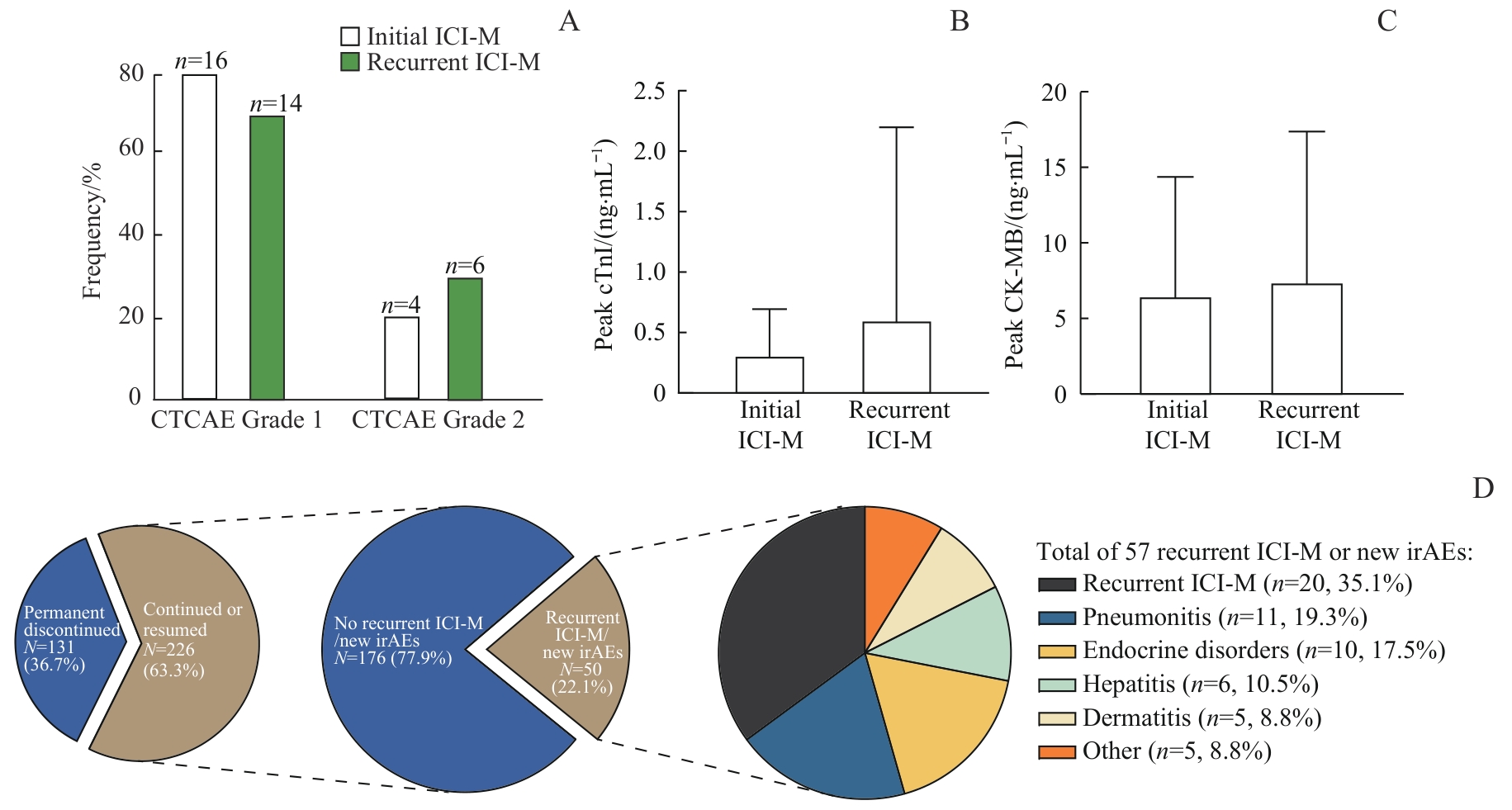
Fig 2 Clinical characteristics of recurrent ICI-M and new-onset irAEs
| Variable | No recurrent ICI-M/new irAEs (n=176) | Recurrent ICI-M/new irAEs (n=50) | P value |
|---|---|---|---|
| Age/year | 67.0 (61.0, 71.0) | 67.0 (62.0, 73.0) | 0.535 |
| Male/n(%) | 157 (89.2) | 44 (88.0) | 1.000 |
| BMI/(kg·m-2) | 22.9 ± 3.4 | 22.5 ± 3.3 | 0.483 |
| Coronary artery disease/n(%) | 28 (15.9) | 11 (22.0) | 0.427 |
| Hyperlipidemia/n(%) | 9 (5.1) | 5 (10.0) | 0.351 |
| Hypertension/n(%) | 63 (35.8) | 18 (36.0) | 1.000 |
| Diabetes/n(%) | 23 (13.1) | 6 (12.0) | 1.000 |
| Chronic kidney disease/n(%) | 2 (1.1) | 3 (6.0) | 0.129 |
| Histology/n(%) | 0.788 | ||
| Squamous cell carcinoma | 64 (36.4) | 17 (34.0) | |
| Adenocarcinoma | 69 (39.2) | 23 (46.0) | |
| Other NSCLC | 22 (12.5) | 6 (12.0) | |
| SCLC | 21 (11.9) | 4 (8.0) | |
| Disease stage/n(%) | 0.146 | ||
| Stage Ⅱ‒Ⅲ | 59 (33.5) | 23 (46.0) | |
| Stage Ⅳ | 117 (66.5) | 27 (54.0) | |
| ECOG performance status①/n(%) | 0.459 | ||
| 0 | 20 (14.8) | 4 (9.3) | |
| 1 | 113 (83.7) | 39 (90.7) | |
| 2 | 2 (1.5) | 0 (0) | |
| Hemoglobin/(g·L-1) | 130.0 (116.0, 140.5) | 128.5 (118.0, 142.0) | 0.951 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 0.366 |
| HbA1c/% | 5.8 (5.5, 6.3) | 5.8 (5.7, 6.3) | 0.384 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.9 (86.3, 101.3) | 94.1 (81.6, 101.2) | 0.655 |
| Radiotherapy/n(%) | 58 (33.0) | 16 (32.0) | 1.000 |
| ICI type after initial ICI-M/n(%) | 1.000 | ||
| PD-1 monotherapy | 150 (85.2) | 43 (86.0) | |
| PD-L1 monotherapy | 26 (14.8) | 7 (14.0) | |
| Anti-tumor treatment after initial ICI-M/n(%) | 0.244 | ||
| ICIs monotherapy | 45 (25.6) | 15 (30.0) | |
| Combination with chemotherapy | 109 (61.9) | 27 (54.0) | |
| Combination with targeted therapy | 12 (6.8) | 7 (14.0) | |
| Combination with chemotherapy and targeted therapy | 10 (5.7) | 1 (2.0) | |
| Number of cycles received prior to ICI-M | 3.0 (2.0, 6.0) | 2.0 (1.0, 4.0) | 0.029 |
| Time to initial ICI-M/d | 71.0 (43.0, 169.0) | 47.0 (27.0, 90.0) | 0.006 |
| CTCAE grade of initial ICI-M/n(%) | 0.864 | ||
| Grade 1 | 162 (92.0) | 45 (90.0) | |
| Grade 2 | 14 (8.0) | 5 (10.0) | |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 160.0) | 85.0 (40.0, 260.0) | 0.683 |
| Peak CK-MB/(ng·mL-1) | 2.8 (1.8, 5.9) | 4.8 (2.4, 9.1) | 0.019 |
| Hospitalization/n(%) | 21 (11.9) | 7 (14.0) | 0.882 |
| Systemic steroids use/n(%) | 10 (5.7) | 6 (12.0) | 0.221 |
| Temporary ICI discontinuation/n(%) | 41 (23.3) | 12 (24.0) | 1.000 |
Tab 2 Risk factors associated with recurrent ICI-M or new-onset irAEs
| Variable | No recurrent ICI-M/new irAEs (n=176) | Recurrent ICI-M/new irAEs (n=50) | P value |
|---|---|---|---|
| Age/year | 67.0 (61.0, 71.0) | 67.0 (62.0, 73.0) | 0.535 |
| Male/n(%) | 157 (89.2) | 44 (88.0) | 1.000 |
| BMI/(kg·m-2) | 22.9 ± 3.4 | 22.5 ± 3.3 | 0.483 |
| Coronary artery disease/n(%) | 28 (15.9) | 11 (22.0) | 0.427 |
| Hyperlipidemia/n(%) | 9 (5.1) | 5 (10.0) | 0.351 |
| Hypertension/n(%) | 63 (35.8) | 18 (36.0) | 1.000 |
| Diabetes/n(%) | 23 (13.1) | 6 (12.0) | 1.000 |
| Chronic kidney disease/n(%) | 2 (1.1) | 3 (6.0) | 0.129 |
| Histology/n(%) | 0.788 | ||
| Squamous cell carcinoma | 64 (36.4) | 17 (34.0) | |
| Adenocarcinoma | 69 (39.2) | 23 (46.0) | |
| Other NSCLC | 22 (12.5) | 6 (12.0) | |
| SCLC | 21 (11.9) | 4 (8.0) | |
| Disease stage/n(%) | 0.146 | ||
| Stage Ⅱ‒Ⅲ | 59 (33.5) | 23 (46.0) | |
| Stage Ⅳ | 117 (66.5) | 27 (54.0) | |
| ECOG performance status①/n(%) | 0.459 | ||
| 0 | 20 (14.8) | 4 (9.3) | |
| 1 | 113 (83.7) | 39 (90.7) | |
| 2 | 2 (1.5) | 0 (0) | |
| Hemoglobin/(g·L-1) | 130.0 (116.0, 140.5) | 128.5 (118.0, 142.0) | 0.951 |
| Albumin/(g·L-1) | 40.0 (37.0, 42.0) | 39.0 (36.0, 41.0) | 0.366 |
| HbA1c/% | 5.8 (5.5, 6.3) | 5.8 (5.7, 6.3) | 0.384 |
| eGFR/[mL·(min·1.73 m2)-1] | 94.9 (86.3, 101.3) | 94.1 (81.6, 101.2) | 0.655 |
| Radiotherapy/n(%) | 58 (33.0) | 16 (32.0) | 1.000 |
| ICI type after initial ICI-M/n(%) | 1.000 | ||
| PD-1 monotherapy | 150 (85.2) | 43 (86.0) | |
| PD-L1 monotherapy | 26 (14.8) | 7 (14.0) | |
| Anti-tumor treatment after initial ICI-M/n(%) | 0.244 | ||
| ICIs monotherapy | 45 (25.6) | 15 (30.0) | |
| Combination with chemotherapy | 109 (61.9) | 27 (54.0) | |
| Combination with targeted therapy | 12 (6.8) | 7 (14.0) | |
| Combination with chemotherapy and targeted therapy | 10 (5.7) | 1 (2.0) | |
| Number of cycles received prior to ICI-M | 3.0 (2.0, 6.0) | 2.0 (1.0, 4.0) | 0.029 |
| Time to initial ICI-M/d | 71.0 (43.0, 169.0) | 47.0 (27.0, 90.0) | 0.006 |
| CTCAE grade of initial ICI-M/n(%) | 0.864 | ||
| Grade 1 | 162 (92.0) | 45 (90.0) | |
| Grade 2 | 14 (8.0) | 5 (10.0) | |
| Peak cTnI/(pg·mL-1) | 80.0 (50.0, 160.0) | 85.0 (40.0, 260.0) | 0.683 |
| Peak CK-MB/(ng·mL-1) | 2.8 (1.8, 5.9) | 4.8 (2.4, 9.1) | 0.019 |
| Hospitalization/n(%) | 21 (11.9) | 7 (14.0) | 0.882 |
| Systemic steroids use/n(%) | 10 (5.7) | 6 (12.0) | 0.221 |
| Temporary ICI discontinuation/n(%) | 41 (23.3) | 12 (24.0) | 1.000 |
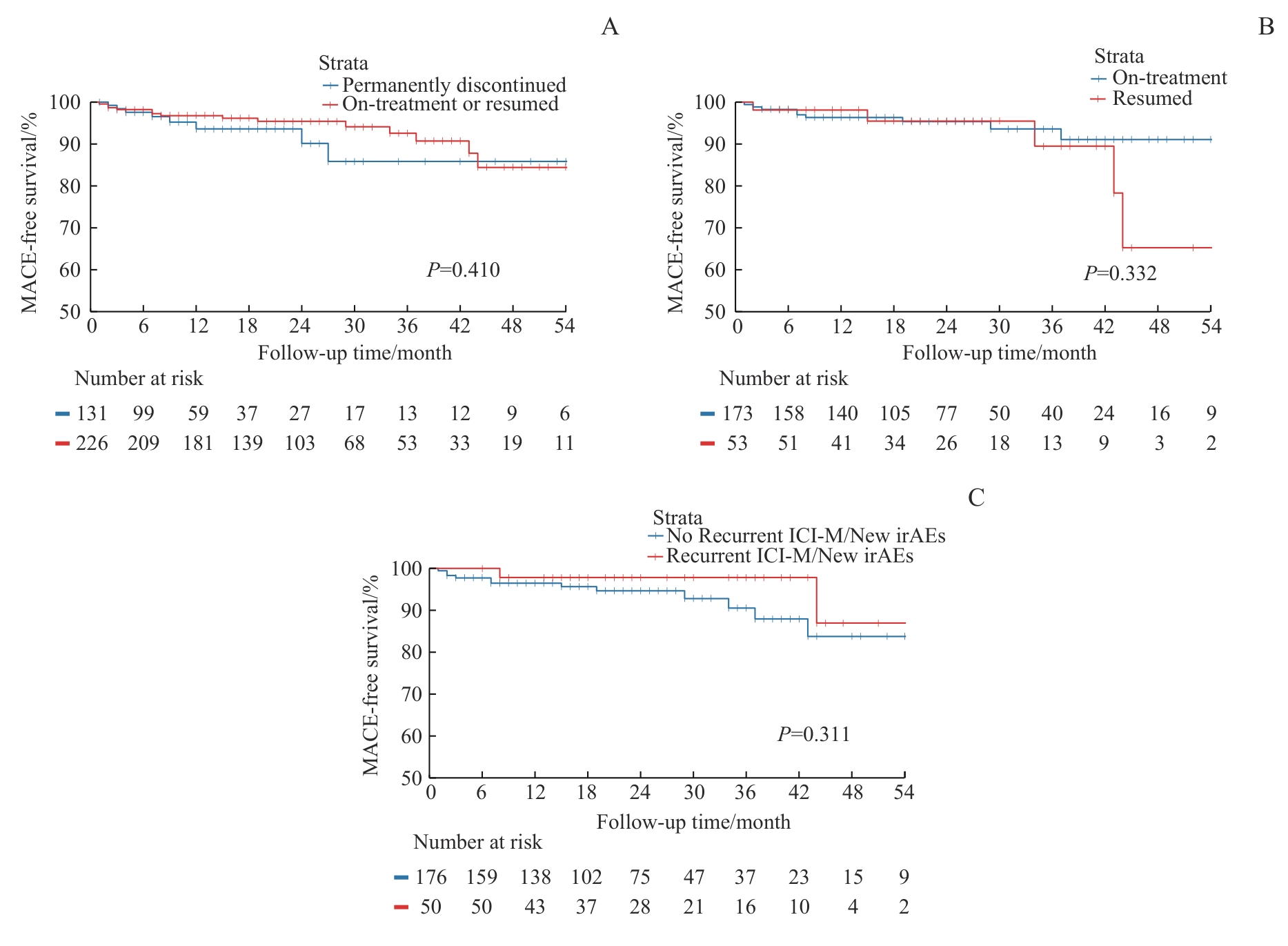
Fig 3 Kaplan-Meier curves for MACE incidence
| Factor | Multivariable analysis | |
|---|---|---|
| HR (95%CI) | P value | |
| On-treatment or resumed ICIs | 0.75 (0.28‒1.98) | 0.556 |
| Coronary artery disease | 2.53 (1.04‒6.17) | 0.041 |
| CTCAE grade of initial ICI-M | ||
| Grade 1 | Ref | |
| Grade 2 | 5.26 (1.91‒14.46) | 0.001 |
| Systemic steroids use for initial ICI-M | 0.63 (0.18‒2.18) | 0.469 |
| ECOG performance status | ||
| 0 | Ref | |
| 1 | 1.62 (0.20‒13.20) | 0.652 |
| 2 | 1.45 (0.06‒32.45) | 0.815 |
| Number of cycles received prior to ICI-M | 1.03 (0.97‒1.09) | 0.359 |
| Ongoing anti-tumor treatment | ||
| ICIs monotherapy | Ref | |
| Combination with chemotherapy | 0.70 (0.25‒1.95) | 0.500 |
| Combination with targeted therapy | 2.38 (0.56‒10.20) | 0.243 |
| Combination with chemotherapy and targeted therapy | 0.65 (0.07‒5.98) | 0.700 |
Tab 3 Multivariable Cox regression analysis of factors associated with MACE in patients with ICI-M
| Factor | Multivariable analysis | |
|---|---|---|
| HR (95%CI) | P value | |
| On-treatment or resumed ICIs | 0.75 (0.28‒1.98) | 0.556 |
| Coronary artery disease | 2.53 (1.04‒6.17) | 0.041 |
| CTCAE grade of initial ICI-M | ||
| Grade 1 | Ref | |
| Grade 2 | 5.26 (1.91‒14.46) | 0.001 |
| Systemic steroids use for initial ICI-M | 0.63 (0.18‒2.18) | 0.469 |
| ECOG performance status | ||
| 0 | Ref | |
| 1 | 1.62 (0.20‒13.20) | 0.652 |
| 2 | 1.45 (0.06‒32.45) | 0.815 |
| Number of cycles received prior to ICI-M | 1.03 (0.97‒1.09) | 0.359 |
| Ongoing anti-tumor treatment | ||
| ICIs monotherapy | Ref | |
| Combination with chemotherapy | 0.70 (0.25‒1.95) | 0.500 |
| Combination with targeted therapy | 2.38 (0.56‒10.20) | 0.243 |
| Combination with chemotherapy and targeted therapy | 0.65 (0.07‒5.98) | 0.700 |
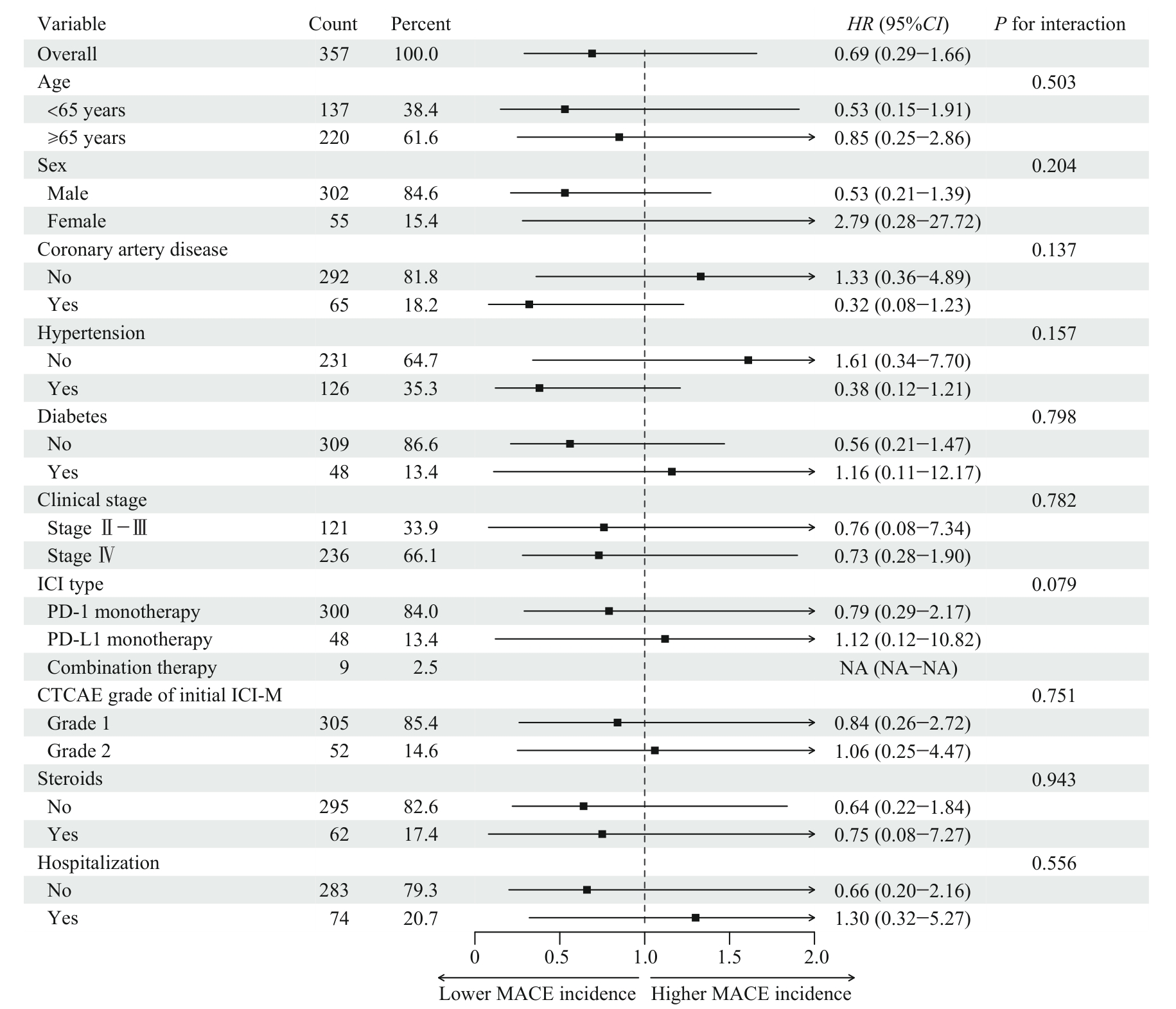
Fig 4 Subgroup analysis of the effect of on-treatment or resumption of ICIs therapy on MACE
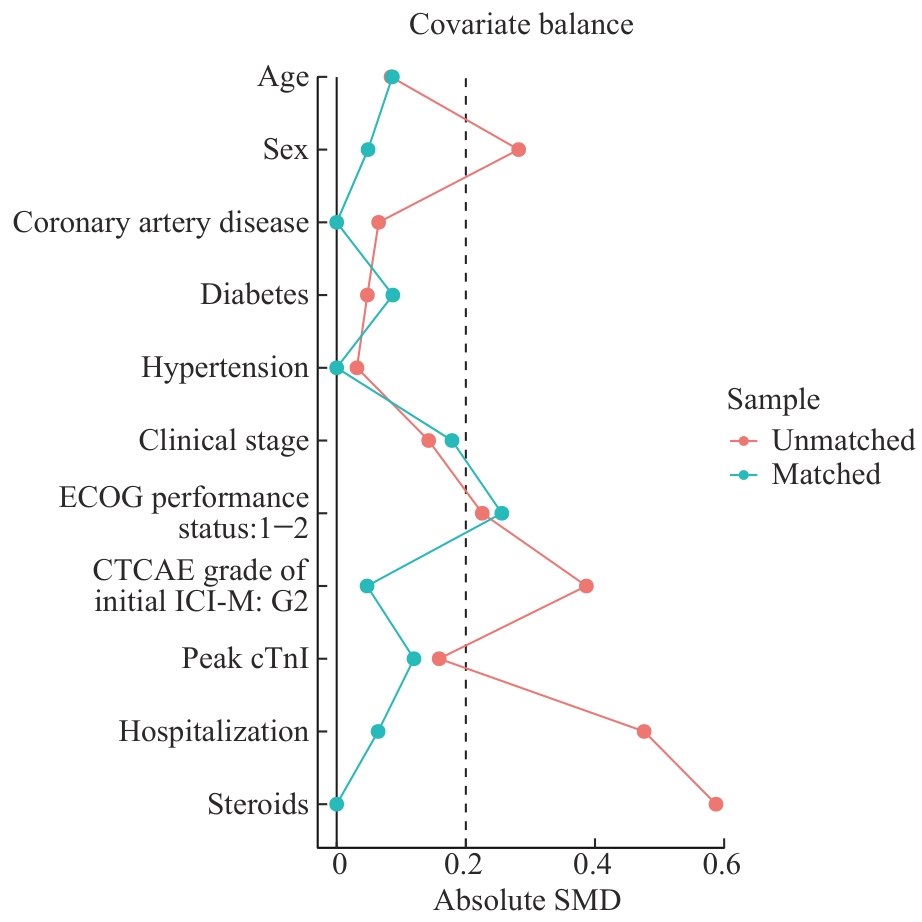
Fig 5 Comparison of SMDs before and after propensity score matching
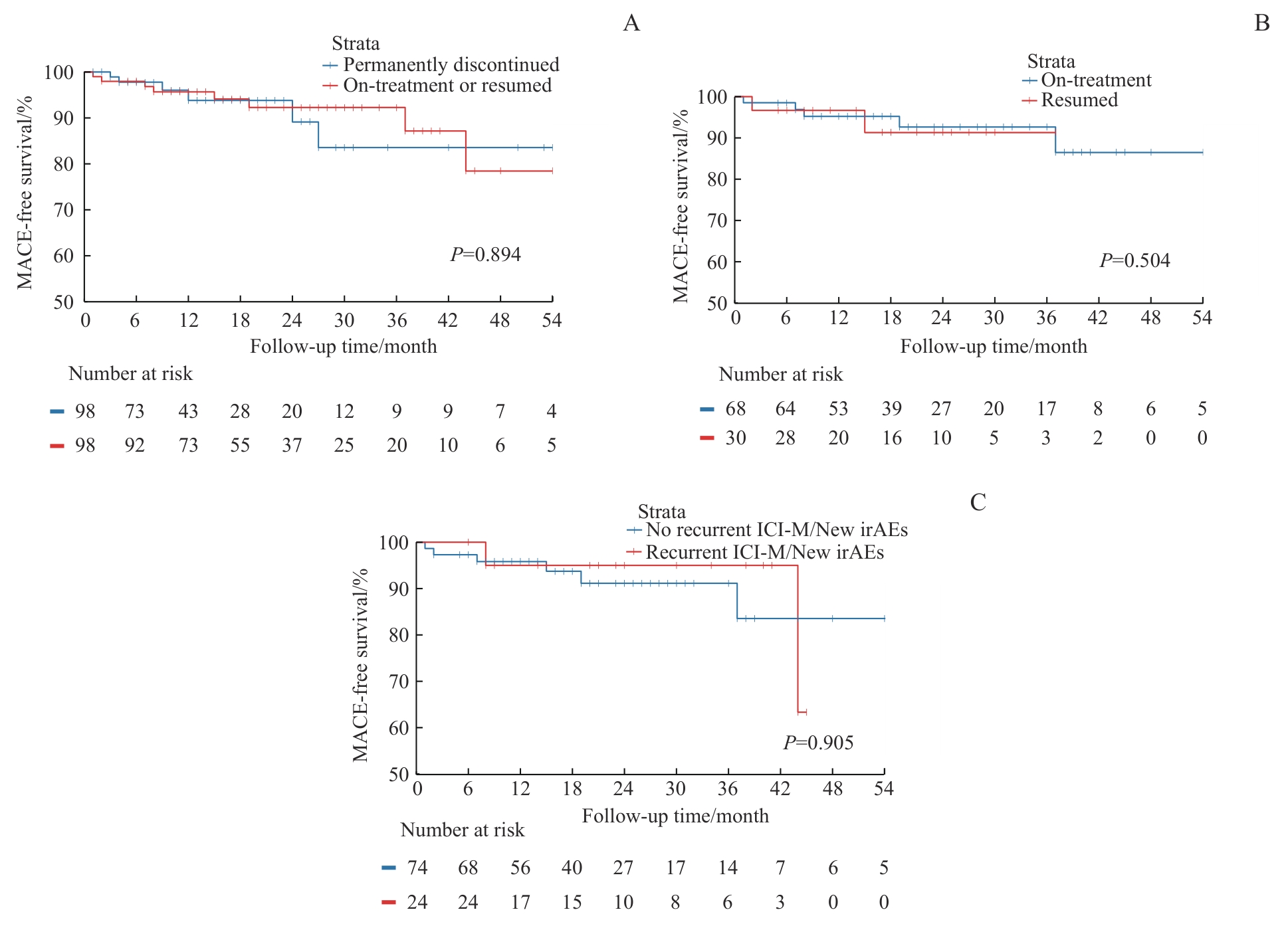
Fig 6 Kaplan-Meier curves for MACE after propensity score matching
| [1] | Ribas A, Wolchok J D. Cancer immunotherapy using checkpoint blockade[J]. Science, 2018, 359(6382): 1350-1355. |
| [2] | Schneider B J, Ismaila N, Aerts J, et al. Lung cancer surveillance after definitive curative-intent therapy: ASCO guideline[J]. J Clin Oncol, 2020, 38(7): 753-766. |
| [3] | Schonfeld S J, Tucker M A, Engels E A, et al. Immune-related adverse events after immune checkpoint inhibitors for melanoma among older adults[J]. JAMA Netw Open, 2022, 5(3): e223461. |
| [4] | Wang D Y, Salem J E, Cohen J V, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis[J]. JAMA Oncol, 2018, 4(12): 1721-1728. |
| [5] | Mahmood S S, Fradley M G, Cohen J V, et al. Myocarditis in patients treated with immune checkpoint inhibitors[J]. J Am Coll Cardiol, 2018, 71(16): 1755-1764. |
| [6] | Salem J E, Manouchehri A, Moey M, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study[J]. Lancet Oncol, 2018, 19(12): 1579-1589. |
| [7] | Vasbinder A, Chen Y, Procureur A, et al. Biomarker trends, incidence, and outcomes of immune checkpoint inhibitor-induced myocarditis[J]. JACC CardioOncol, 2022, 4(5): 689-700. |
| [8] | Curigliano G, Lenihan D, Fradley M, et al. Management of cardiac disease in cancer patients throughout oncological treatment: ESMO consensus recommendations[J]. Ann Oncol, 2020, 31(2): 171-190. |
| [9] | Schneider B J, Naidoo J, Santomasso B D, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update[J]. J Clin Oncol, 2021, 39(36): 4073-4126. |
| [10] | 中国抗癌协会整合肿瘤心脏病学分会, 中华医学会心血管病学分会肿瘤心脏病学学组, 中国医师协会心血管内科医师分会肿瘤心脏病学专业委员会, 等. 免疫检查点抑制剂相关心肌炎监测与管理中国专家共识(2020版)[J]. 中国肿瘤临床, 2020, 47(20): 1027-1038. |
| Society of Integrative Cardio-Oncology China Anti-Cancer Association, The Cardio-Oncology Group of the Chinese Society of Cardiovascular Diseases of Chinese Medical Association, Chinese College of Cardiovascular Physicians Specialized Committee on Cardio-Oncology Chinese Medical Docotor Association, et al. Chinese expert consensus on the surveillance and management of immune checkpoint inhibitor-related myocarditis (2020 version)[J]. Chinese Journal of Clinical Oncology, 2020, 47(20): 1027-1038. | |
| [11] | Herrmann J, Lenihan D, Armenian S, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement[J]. Eur Heart J, 2022, 43(4): 280-299. |
| [12] | Zannad F, Cannon C P, Cushman W C, et al. Heart failure and mortality outcomes in patients with type 2 diabetes taking alogliptin versus placebo in EXAMINE: a multicentre, randomised, double-blind trial[J]. Lancet, 2015, 385(9982): 2067-2076. |
| [13] | Dziura J D, Post L A, Zhao Q, et al. Strategies for dealing with missing data in clinical trials: from design to analysis[J]. Yale J Biol Med, 2013, 86(3): 343-358. |
| [14] | Austin P C. Some methods of propensity-score matching had superior performance to others: results of an empirical investigation and Monte Carlo simulations[J]. Biom J, 2009, 51(1): 171-184. |
| [15] | Coustal C, Vanoverschelde J, Quantin X, et al. Prognosis of immune checkpoint inhibitors-induced myocarditis: a case series[J]. J Immunother Cancer, 2023, 11(5): e004792. |
| [16] | Dolladille C, Ederhy S, Sassier M, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer[J]. JAMA Oncol, 2020, 6(6): 865-871. |
| [17] | L'Orphelin J M, da Silva A, Cabon J, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events: a retrospective study from VigiBase update in 2024 looking for emergent safety signals[J]. BMJ Open, 2024, 14(12): e091708. |
| [18] | Pollack M H, Betof A, Dearden H, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma[J]. Ann Oncol, 2018, 29(1): 250-255. |
| [19] | Simonaggio A, Michot J M, Voisin A L, et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer[J]. JAMA Oncol, 2019, 5(9): 1310-1317. |
| [20] | Santini F C, Rizvi H, Plodkowski A J, et al. Safety and efficacy of re-treating with immunotherapy after immune-related adverse events in patients with NSCLC[J]. Cancer Immunol Res, 2018, 6(9): 1093-1099. |
| [21] | Mulholland M, Chalou A, Andersson S H A, et al. Progenitor exhausted PD-1+ T cells are cellular targets of immune checkpoint inhibition in atherosclerosis[J]. Nat Cardiovasc Res, 2025, 4(10): 1311-1328. |
| [22] | Barcia Durán J G, Das D, Gildea M, et al. Immune checkpoint landscape of human atherosclerosis and influence of cardiometabolic factors[J]. Nat Cardiovasc Res, 2024, 3(12): 1482-1502. |
| [23] | van Dorst D C H, Uyl T J J, van der Veldt A A M, et al. Onset and progression of atherosclerosis in patients with melanoma treated with immune checkpoint inhibitors[J]. J Immunother Cancer, 2025, 13(4): e011226. |
| [24] | Drobni Z D, Gongora C, Taron J, et al. Impact of immune checkpoint inhibitors on atherosclerosis progression in patients with lung cancer[J]. J Immunother Cancer, 2023, 11(7): e007307. |
| [25] | Drobni Z D, Alvi R M, Taron J, et al. Association between immune checkpoint inhibitors with cardiovascular events and atherosclerotic plaque[J]. Circulation, 2020, 142(24): 2299-2311. |
| [26] | Guo M N, VanderWalde A M, Yu X H, et al. Immune checkpoint inhibitor rechallenge safety and efficacy in stage Ⅳ non-small cell lung cancer patients after immune-related adverse events[J]. Clin Lung Cancer, 2022, 23(8): 686-693. |
| [27] | Chen X, Jiang A M, Zhang R, et al. Immune checkpoint inhibitor-associated cardiotoxicity in solid tumors: real-world incidence, risk factors, and prognostic analysis[J]. Front Cardiovasc Med, 2022, 9: 882167. |
| [28] | Lee D H, Armanious M, Huang J, et al. Case of pembrolizumab-induced myocarditis presenting as torsades de pointes with safe re-challenge[J]. J Oncol Pharm Pract, 2020, 26(6): 1544-1548. |
| [29] | Eslinger C, Walden D, Barry T, et al. Rechallenge with switching immune checkpoint inhibitors following autoimmune myocarditis in a patient with lynch syndrome[J]. J Natl Compr Cancer Netw, 2023, 21(9): 894-899. |
| [30] | Shalata W, Attal Z G, Shhadi R, et al. Tolerated re-challenge of immunotherapy in a patient with ICI associated myocarditis: a case report and literature review[J]. Medicina (Kaunas), 2023, 59(11): 1946. |
| [1] | Jia Yuanwang, Qu Ming, Xin Ran, Liu Zinuan, Yang Shiyi, Kang Wen, Wang Weiran, Liu Xiao, Yang Junjie, Chen Yundai. Preliminary study on a mechanics-parameter-based strategy for real-time vascular angle prediction and safety warning in vascular interventional robots [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2026, 46(3): 265-274. |
| [2] | ZHENG Mengyi, MAO Jialiang, ZOU Zhiguo, ZHANG Ruilei, ZHANG Hou, LI Shiguang. Predictive value of systemic immune inflammation index and somatic symptom scale-China in the occurrence of in-hospital major adverse cardiovascular events after first-episode of acute myocardial infarction undergoing PCI [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2024, 44(3): 334-341. |
| [3] | HUANG Huayan, XU-ZHANG Wendi, XIA Liliang, YU Yongfeng, LU Shun. Advances in immunotherapy of advanced non-small cell lung cancer with EGFR mutation [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(5): 611-618. |
| [4] | YANG Xiaoxuan, ZHU Shan, QIAN Cheng, CHU Xiaoying. Effect of intraoperative use of low-dose dexmedetomidine on the prognosis of patients undergoing breast cancer surgery [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(2): 194-200. |
| [5] | TU Juanjuan, JIN Zhiming. Research progress of immune checkpoint inhibitors in the treatment of metastatic colorectal cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(2): 250-255. |
| [6] | WU Lei, XIA Yimeng. Anesthetic application of PetCO2 monitoring nasopharyngeal airway to magnifying endoscopy in patients with obstructive sleep apnea syndrome [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(12): 1542-1547. |
| [7] | WEI Shan, JI Ouyang, CHEN Zhihao, HUANG Zehui, LI Pu, FANG Junyan, LIU Yingli. A prevalence study on knowledge, attitude, belief and practice of safe medication and analysis of related factors in dialysis patients [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2023, 43(1): 88-94. |
| [8] | HAN Ting, LÜ Chunxin, ZHUO Meng, XIA Qing, LIU Tengfei, WU Xiuqi, LIN Xiaolin, XIAO Xiuying. Related factors and prognostic analysis of adverse events of immunotherapy in advanced gastric cancer [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(8): 1053-1061. |
| [9] | JIN Lei, XU Wenbin, YE Chenjing, YAN Hua. Prophylactic antifungal effect of posaconazole on patients with hematological malignant tumor undergoing chemotherapy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(6): 792-796. |
| [10] | ZHU Tianyu, ZONG Chunyan, XU Shiqiong, GE Shengfang, FAN Xianqun, JIA Renbing. Relationship between histopathological features, Ki-67 expression and prognosis of conjunctival melanoma [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(5): 617-623. |
| [11] | DENG Lu, LI Jiayi. Research progress of fractional CO2 laser therapy in female stress urinary incontinence [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(5): 685-689. |
| [12] | Xuehong WANG, Xuzhuo CHEN, Yi MAO, Da SHEN, Shanyong ZHANG. Difference in recurrence rates after temporomandibular joint disc repositioning surgery with miniscrew anchor at different developmental stages in adolescents [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2022, 42(2): 173-177. |
| [13] | Yanyan LIN, Yan XU, Hui LI. Progress in research on the mechanism of drug resistance to conventional chemotherapeutic drugs in children with acute lymphoblastic leukemia [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2022, 42(2): 211-217. |
| [14] | HU Ningning, ZHANG Dan, ZOU Jun, ZHANG Chong, LIN Fujun, JIANG Gengru. Efficacy and safety evaluation of tacrolimus monotherapy in the treatment of idiopathic membranous nephropathy [J]. Journal of Shanghai Jiao Tong University (Medical Science), 2022, 42(12): 1685-1692. |
| [15] | Yihuan WANG, Ruokun LI, Huanhuan CHONG, Fuhua YAN. Research progress of Gd-EOB-DTPA-enhanced magnetic resonance imaging in the evaluation of biological behavior of hepatocellular carcinoma [J]. JOURNAL OF SHANGHAI JIAOTONG UNIVERSITY (MEDICAL SCIENCE), 2022, 42(1): 130-134. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||